Download presentation
Presentation is loading. Please wait.

1
Renovascular hypertension Dr Saad Al Shohaib KAUH

2
Incidence Renovascular disease is an important and treatable cause of hypertension and renal impairment It accounts for less than 1% of mild and moderate hypertension but may be seen in 10 to 40% of hypertensive crises Renal disease is the comments cause of secondary hypertension

3
Target population for screening Acute rise in serum creatinine shortly after ACE inhibitor therapy or unexplained rapid deterioration in renal function with minimal proteinuria Moderate to sever hypertension in a patient with diffuse atherosclerosis Hypertension in a patient with a symmetric renal size or hypokalemia Moderate to severe hypertension in patients with recurrent episodes of acute (flash) pulmonary edema or otherwise unexplained congestive heart failure
 pulmonary edema or otherwise unexplained congestive heart failure")
5
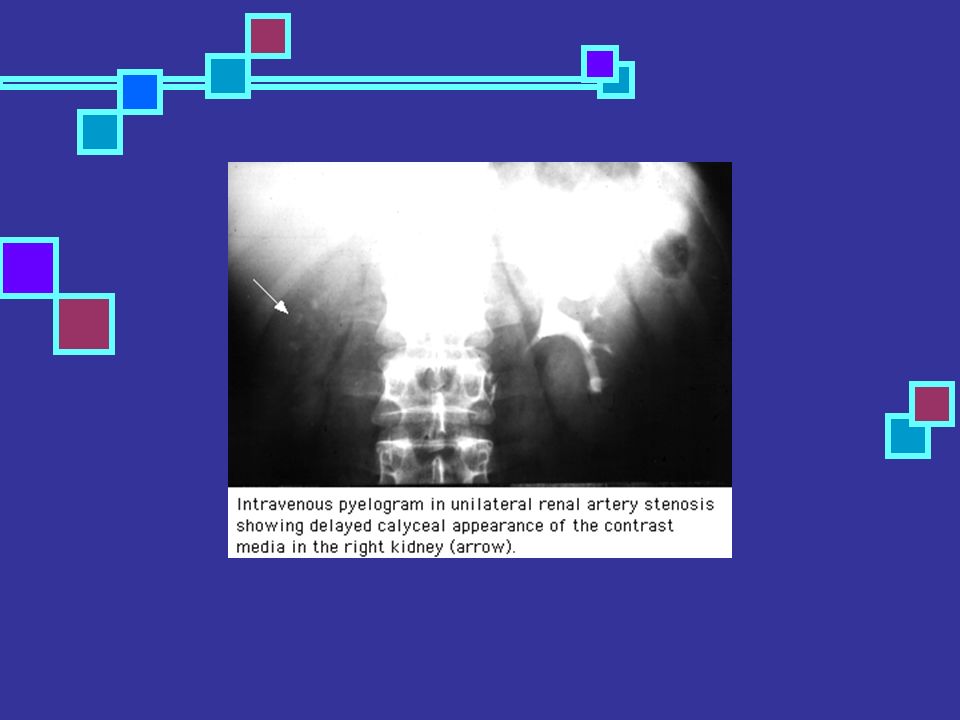
Screening tests Intravenous pyelogram – There are two major findings on intravenous pyelography that suggest the presence of unilateral ischemia: a decrease in renal size; and delayed caliceal appearance time when compared to the contralateral kidney

7
Screening Plasma renin activity – The baseline plasma renin activity is elevated in only 50 to 80 percent of patients with renovascular hypertension. The predictive value can be increased by measuring the rise in the plasma renin activity one hour after the administration of 25 to 50 mg of captopril

8
screening Renogram following ACE inhibitor the predictive value of radioisotope scanning can be increased by enhancement with captopril.

9
Screening Duplex Doppler ultrasonography has the advantage of providing both anatomic and functional assessment of the renal arteries Time consuming Operator dependent and difficult It can be done after captopril

10
Recommendations In high risk patients may use subs traction angiogram as an initial test MR angiography is a non invasive alternative test particularly if combined with doppler

11
Postma CT Joosten FB etal AM J Hyper sept 1997 In one study 38 patients with hypertension were screened using MRA and subs traction angiogram One patient was excluded 14 patients had renal artery steno sis 12 patients had more than 50% stenosis

12
All these stenos is were recognized by MRA There were one false positive case by MRA MRA has 100% sensitivity and 96% specifity Postma CT; Joosten FB; Rosenbusch G; Thien T SO - Am J Hypertens 1997 Sep;10(9 Pt 1):957-63
:957-63")
13
Conclusion MRA has a great accuracy in detecting clinically significant main renal artery stenos is

14
Significant stenosis Hem dynamically significant stenos only should be corrected Good response to ACE inhibitors suggest the presence of significant stenos increased Renal vein renin may suggest a significant stenosis but this is not widely used Other tests used to screen for renovascular hypertension would help to determine significance

15
CRF AND ISCHAEMIA Ischemia might be responsible for decreased renal function in a significant number of patients with renal failure in older patients Correction of ischemia would improve renal function

16
Renal insufficiency Unexplained progressive renal failure Benign urine sediment with sever renal impairment Unilateral very small kidney with renal impairment Testing should be done with progressive renal impairment uncontrolled pressure and recurrent pulmonary edema Contrast may induce further renal damage

17
Ischemia and CRF Presence of diffuse atherosclerosis make Reno vascular disease more likely There is usually minimal proteinuria Uncontrolled hypertension Flash pulmonary edema Progressive renal failure with benign urine sediment

18
Renovascular disease The earlier the intervention the better the prognosis Contrast may cause further renal damage Reversibility is more likely in patients with rapid deterioration of renal function

19
Conclusion Renovascular hypertension should be suspected in hypertensive crisis uncontrolled hypertension patients with hypokalemia and high BP Presence of unequal kidney size or flash pulmonary edema make the diagnosis more likely

20
Conclusion The homodynamic effect of ِِACE inhibitors help in the diagnosis reversibility of renal function as well as the significance of the stenosis Uncontrolled hypertension in a patient with diffuse atherosclerosis particularly if associated with renal impairment is highly suggestive of renovascular hypertension

21
Conclusion MRA with Doppler ultrasound are good screening tests Revascularization should be done in hem dynamically significant stenosis Correction of significant bilateral stenosis may improve renal failure and help to avoid dialysis in selected cases

22
Thank you

Similar presentations


 Sepehr Khashaei, MD Assistant professor Department of Internal Medicine.>")


:>")






>")






