Download presentation
Presentation is loading. Please wait.

1
TUMOURS OF THE BRONCHUS AND LUNG 4th year Medical (1)
Dr.Dhaher JS Al-habbo FRCP London UK Assistant Professor in Medicine DEPARTMENT OF MEDICINE

2
The burden of lung cancer
Strikes men and women each year Accounts for 18% of all cancer deaths More than a threefold increase in deaths since 1950 Rates rising in women: female lung cancer deaths outnumber male in some Nordic countries Has overtaken breast cancer in several countries, making it the most common cause of cancer death in men and women

3
The burden of lung cancer
Cigarette smoking is by far the most important cause of lung cancer., for at least 90 being proportional to the amount smoked and to the tar content of cigarettes. The death rate from the disease in heavy smokers is 40 times that in non-smokers. Risk falls slowly after smoking cessation, but remains above that in non-smokers for many years Exposure to naturally occurring radon is another risk. The incidence of lung cancer is slightly higher in urban than in rural dwellers.which may reflect differences in atmospheric .

4
Bronchial carcinoma The incidence of bronchial carcinoma increased dramatically during the 20th century as a direct result of the tobacco epidemic . In women, smoking prevalence and deaths from lung cancer continue to increase, and more women now die of lung cancer than breast cancer in the USA and the UK

5
Bronchial carcinoma Bronchial carcinomas arise from the bronchial epithelium or mucous glands. The common cell types are: Squamous35%, Adenocarcinoma30%, Small-cell20%, and Large-cell 15%. Tumour occurs in a large bronchus, symptoms arise early, but tumours originating in a peripheral bronchus can grow very large without producing symptoms, resulting in delayed diagnosis. Peripheral squamous tumours may undergo central necrosis and cavitation, and may resemble a lung abscess on X-ray .

6
Bronchial carcinoma Bronchial carcinoma may involve the pleura either directly or by lymphatic spread and may extend into the chest wall, invading the intercostal nerves or the brachial plexus and causing pain. Lymphatic spread to mediastinal and supraclavicular lymph nodes frequently occurs prior to diagnosis. Blood-borne metastases occur most commonly in liver, bone, brain, adrenals and skin. Even a small primary tumour may cause widespread metastatic deposits and this is a particular characteristic of small-cell lung cancers.

7
Clinical Presentation of Bronchial carcinoma
Cough. The most common early symptom, cough is often dry; however, secondary infection may cause purulent sputum. A change in the character of a smoker's cough, particularly if associated with other new symptoms, should always raise suspicion of bronchial carcinoma. Haemoptysis. This is common, especially with central bronchial tumours. Although it may be benign, haemoptysis in a smoker should always be investigated to exclude a bronchial carcinoma. Occasionally, central tumours invade large vessels, causing sudden massive haemoptysis which may be fatal

8
Clinical Presentation of Bronchial carcinoma
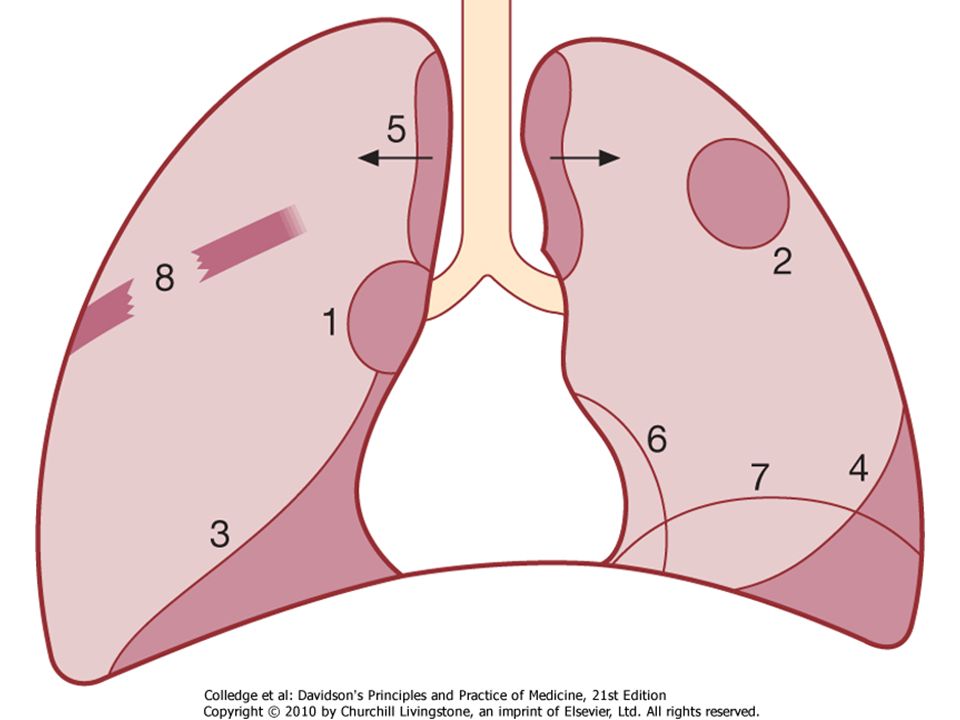
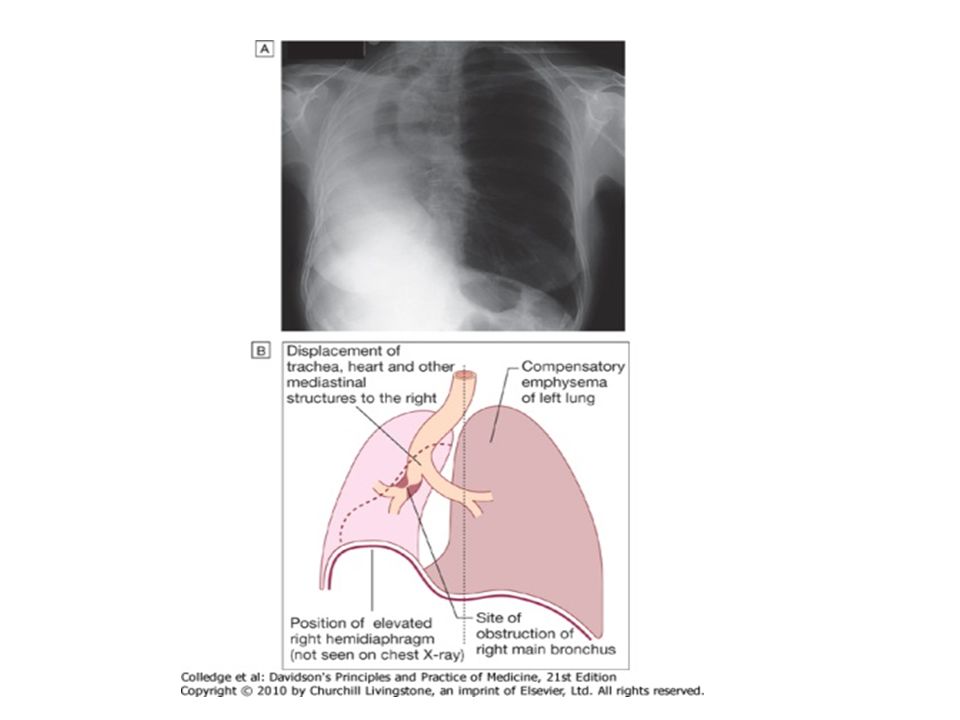
Bronchial obstruction. The clinical and radiological manifestations depend on the site and extent of the obstruction, any secondary infection, and the extent of coexisting lung disease. Complete obstruction causes collapse of a lobe or lung, with breathlessness, mediastinal displacement and dullness to percussion with reduced breath sounds. Partial bronchial obstruction may cause a monophonic, unilateral wheeze that fails to clear with coughing and may also impair the drainage of secretions sufficiently to cause pneumonia or lung abscess as a presenting problem.

9
Clinical Presentation of Bronchial carcinoma
Pneumonia that recurs at the same site or responds slowly to treatment, particularly in a smoker, should always suggest an underlying bronchial carcinoma. Stridor (a harsh inspiratory noise) occurs when the lower trachea, carina or main bronchi are narrowed by the primary tumour or by compression from malignant enlargement of the subcarinal and paratracheal lymph nodes. Breathlessness. This may be caused by collapse or pneumonia, or by tumour causing a large pleural effusion or compressing a phrenic nerve causing diaphragmatic paralysis.
 occurs when the lower trachea, carina or main bronchi are narrowed by the primary tumour or by compression from malignant enlargement of the subcarinal and paratracheal lymph nodes. Breathlessness. This may be caused by collapse or pneumonia, or by tumour causing a large pleural effusion or compressing a phrenic nerve causing diaphragmatic paralysis.")
10
Clinical Presentation of Bronchial carcinoma
Pain and nerve entrapment. Pleural pain usually indicates malignant pleural invasion, although it can occur with distal infection. Intercostal nerve involvement causes pain in the distribution of a thoracic dermatome. Carcinoma in the lung apex may cause Horner's syndrome (ipsilateral partial ptosis, enophthalmos, miosis and hypohidrosis of the face) due to involvement of the sympathetic chain at or above the stellate ganglion. Pancoast's syndrome (pain in the shoulder and inner aspect of the arm, sometimes with small muscle wasting in the hand) indicates malignant destruction of the T1 and C8 roots in lower part of the brachial plexus by an apical lung tumour.
 due to involvement of the sympathetic chain at or above the stellate ganglion. Pancoast s syndrome (pain in the shoulder and inner aspect of the arm, sometimes with small muscle wasting in the hand) indicates malignant destruction of the T1 and C8 roots in lower part of the brachial plexus by an apical lung tumour.")
11
Clinical Presentation of Bronchial carcinoma
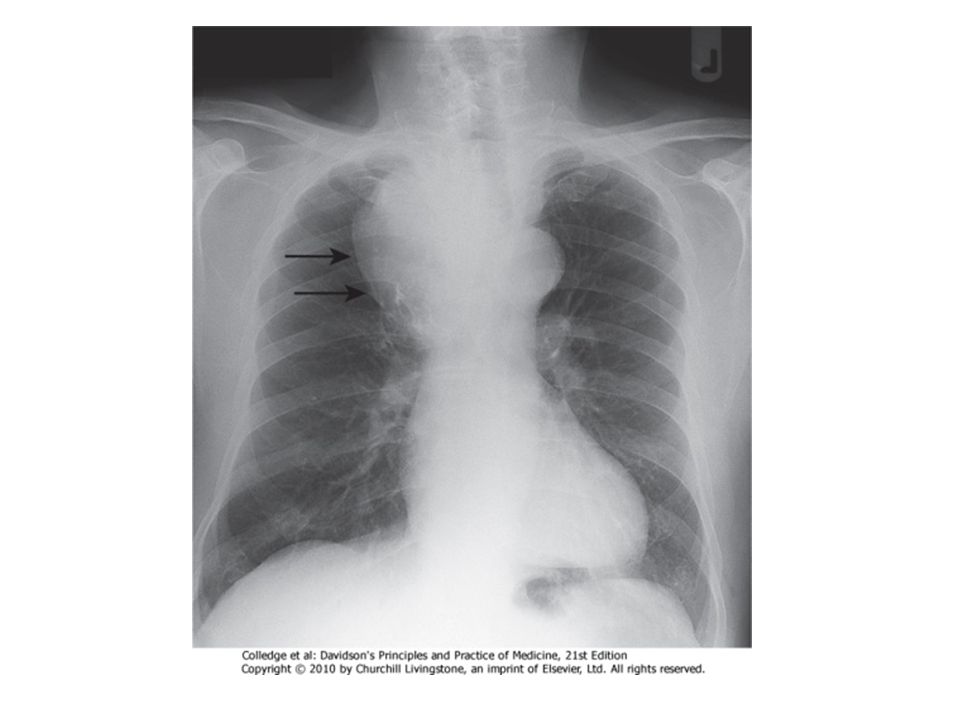
Mediastinal spread. Involvement of the oesophagus may cause dysphagia. If the pericardium is invaded, arrhythmia or pericardial effusion may occur. Superior vena cava obstruction by malignant nodes causes suffusion and swelling of the neck and face, conjunctival oedema, headache and dilated veins on the chest wall, and is most commonly due to bronchial carcinoma.

12
Clinical Presentation of Bronchial carcinoma
Involvement of the left recurrent laryngeal nerve by tumours at the left hilum causes vocal cord paralysis, voice alteration and a 'bovine' cough (lacking the normal explosive character). Supraclavicular lymph nodes may be palpably enlarged; if so, a needle aspirate may provide a simple means of cytological diagnosis. Metastatic spread. This may lead to focal neurological defects, epileptic seizures, personality change, jaundice, bone pain or skin nodules. Lassitude, anorexia and weight loss usually indicate metastatic spread.
. Supraclavicular lymph nodes may be palpably enlarged; if so, a needle aspirate may provide a simple means of cytological diagnosis. Metastatic spread. This may lead to focal neurological defects, epileptic seizures, personality change, jaundice, bone pain or skin nodules. Lassitude, anorexia and weight loss usually indicate metastatic spread.")
13
Clinical Presentation of Bronchial carcinoma
Digital clubbing. Overgrowth of the soft tissue of the terminal phalanx leading to increased nail curvature is often seen . This may be associated with hypertrophic pulmonary osteoarthropathy (HPOA), characterised by periostitis of the long bones, most commonly the distal tibia, fibula, radius and ulna. This causes pain and tenderness over the affected bones and often pitting oedema over the anterior aspect of the shin. X-rays reveal subperiosteal new bone formation. While most frequently associated with bronchial carcinoma, HPOA can occur with other tumours.
, characterised by periostitis of the long bones, most commonly the distal tibia, fibula, radius and ulna. This causes pain and tenderness over the affected bones and often pitting oedema over the anterior aspect of the shin. X-rays reveal subperiosteal new bone formation. While most frequently associated with bronchial carcinoma, HPOA can occur with other tumours.")
14
Clinical Presentation of Bronchial carcinoma
Non-metastatic extrapulmonary effects .Syndrome of inappropriate antidiuretic hormone secretion (SIADH) and ectopic adrenocorticotrophic hormone secretion are usually associated with small-cell lung cancer Hypercalcaemia is usually caused by squamous cell carcinoma. Associated neurological syndromes may occur with any type of bronchial carcinoma
 and ectopic adrenocorticotrophic hormone secretion are usually associated with small-cell lung cancer. Hypercalcaemia is usually caused by squamous cell carcinoma. Associated neurological syndromes may occur with any type of bronchial carcinoma.")
15
EARLY SYMPTOMS LATE SYMPTOMS Cough/chronic cough Dyspnea Hemoptysis
Chest/shoulder pain Recurring temperature Recurring respiratory infections Bone pain, spinal cord compression Chest pain/tightness Dysphagia Head and neck edema Blurred vision, headaches Weakness, anorexia, weight-loss, cachexia Pleural effusion Liver metastasis/regional spread Early Signs Late signs

16
Causes of large bronchus obstruction
Common causes: Carcinoma or adenoma Enlarged tracheobronchial lymph nodes (malignant or tuberculous) Inhaled foreign bodies (especially right lung and in children) Bronchial casts or plugs consisting of inspissated mucus or blood clot (especially asthma, cystic fibrosis, haemoptysis, debility) Collections of mucus or mucopus retained in the bronchi as a result of ineffective expectoration (especially post-operative following abdominal surgery)
 Inhaled foreign bodies (especially right lung and in children) Bronchial casts or plugs consisting of inspissated mucus or blood clot (especially asthma, cystic fibrosis, haemoptysis, debility) Collections of mucus or mucopus retained in the bronchi as a result of ineffective expectoration (especially post-operative following abdominal surgery)")
17
Causes of large bronchus obstruction
Rare causes: Aortic aneurysm Giant left atrium Pericardial effusion Congenital bronchial atresia Fibrous bronchial stricture (e.g. following TB or bronchial surgery/lung transplant)
")
18
Non-metastatic extrapulmonary manifestations of bronchial carcinoma
Endocrine Inappropriate antidiuretic hormone secretion causing hyponatraemia Ectopic adrenocorticotrophic hormone secretion Hypercalcaemia due to secretion of parathyroid hormone-related peptides Carcinoid syndrome Gynaecomastia

19
Non-metastatic extrapulmonary manifestations of bronchial carcinoma
Neurological Polyneuropathy Myelopathy Cerebellar degeneration Myasthenia (Lambert-Eaton syndrome). Other Digital clubbing Hypertrophic pulmonary osteoarthropathy Nephrotic syndrome Polymyositis and dermatomyositis Eosinophilia
. Other. Digital clubbing. Hypertrophic pulmonary osteoarthropathy. Nephrotic syndrome. Polymyositis and dermatomyositis. Eosinophilia.")
20
Investigations for Bronchial carcinoma
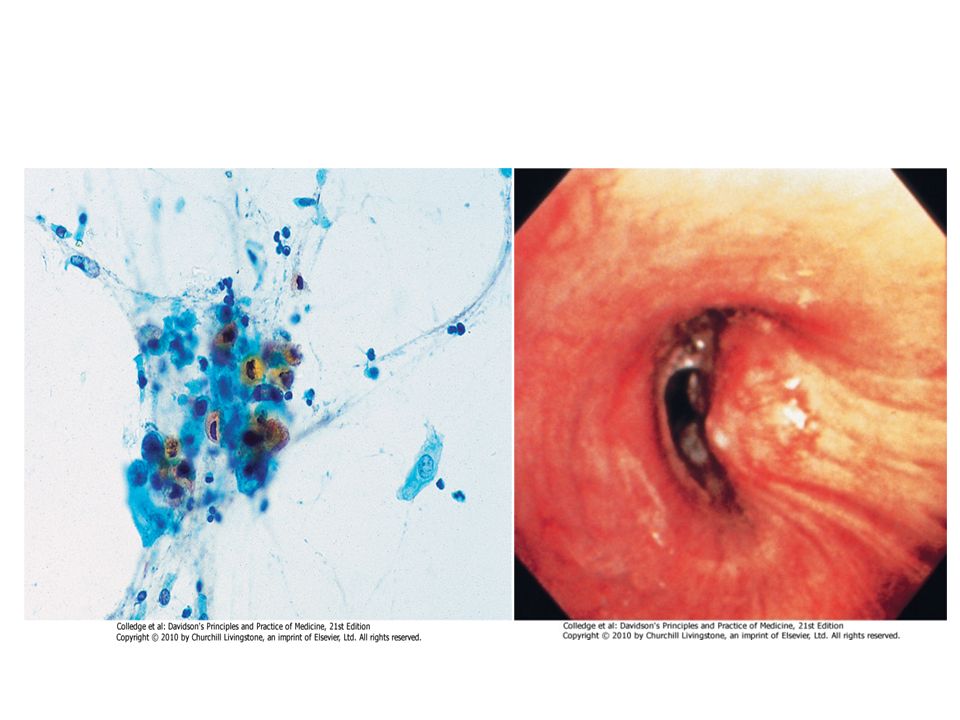
Plain X-rays CT is usually performed for : localization,operability, metastatic spread and for accessible or not by bronchoscopy . Bronchoscopy ;three-quarters of primary lung tumours can be visualised and sampled directly by biopsy and brushing using a flexible bronchoscope. Percutaneous needle biopsy under CT or ultrasound guidance; more reliable way to obtain a histological diagnosis for tumours which are too peripheral

22
Large cavitated bronchial carcinoma in left lower lobe

24
Pan cost left lung↓ with Rib eroson
↓Adenocarcinoma Pan cost left lung↓ with Rib eroson

25
↓Pancost Right lung Pancostleft lung↓

26
MRI top CT lower Cavity Squ.carc

29
To be continued in the 2nd lecture
ان شاء الله

Similar presentations










 SHEN JIN The First Affiliated Hospital of Kunming Medical College.>")








