Download presentation
Presentation is loading. Please wait.

1
Arrhythmias

2
ECG ECG is a graphic representation of the sequence of myocardial depolarisation and repolarisation. Each noarmal cardiac cycle consists of a P wave QRS complex T wave

3
Anatomy of the conduction system in relation to ECG

4
Normal Heart Rate by Age

5
Placement of electrodes for ECG Monitoring

6
Cardiac Rhythm Disturbances
Recognize that rhythm disturbances are an uncommon cause of cardiovascular arrest in children Define 3 classes of rhythm disturbances Assess and manage rhythm disturbances associated with shock (unstable)
")
7
Treatment - Stable Versus Unstable
Unstable rhythms require emergency therapy Rhythms that cause circulatory instability Rhythms that may deteriorate and cause circulatory instability

8
Assessment of Cardiovascular Function
Assess Ventilation, Heart rate, Peripheral pulses, End organ perfusion, Blood pressure. Is CPR needed? Is cardiovascular instability present? Compensated shock Hypotensive shock Cardiopulmonary arrest

9
Definition of Rhythm Groups by Pulse (central) Rate Fast pulse = Tachyarrhythmia Slow pulse = Bradyarrhythmia Absent pulse = Collapse rhythms Rate Infant Child Fast >220 >180 Slow <80 <60

10
Development of Shock From Pulse Rate Disturbances Cardiac Output = Heart Rate X Stroke Volume
HR X SV FAST Low High SLOW Normal , High or Low ABSENT

11
Assessment of Cardiac Rhythm Group
Is the pulse rate slow, fast or absent? Is the perfusion compromised? Are the ventricular complexes wide or narrow? Is there a diagnostic pattern to the ECG?

12
Assessment Of Tachycardia ( Fast Pulse )
Tachycardia appropriate for clinical condition= Sinus tachycardia Tachycardia excessive for clinical condition= Tachyarrhythmia Narrow QRS Complex Sinus Tachycardia Supraventricular Tachycardia Wide QRS Complex Ventricular Tachycardia

13
Supraventricular Tachycardia
Sinus Tachycardia Supraventricular Tachycardia History Possible history of fever, pain, or volume loss (eg. Diarrhea, vomiting, bleeding) Nonspecific history of irritability, lethargy, poor feeding, tachypnea, sweating, pallor, or hypothermia Heart Rate P waves present and normal Variable RR with constant PR Infants rate <220bpm Children <180bpm P waves absent or abnormal Abrupt rate change to or from normal Infants rate usually>220bpm Children >180bpm
 Nonspecific history of irritability, lethargy, poor feeding, tachypnea, sweating, pallor, or hypothermia. Heart Rate. P waves present and normal. Variable RR with constant PR. Infants rate <220bpm. Children <180bpm. P waves absent or abnormal. Abrupt rate change to or from normal. Infants rate usually>220bpm. Children >180bpm.")
14
Sinus Rhythm

15
Supraventricular Tachycardia

16
Ventricular Tachycardia

19
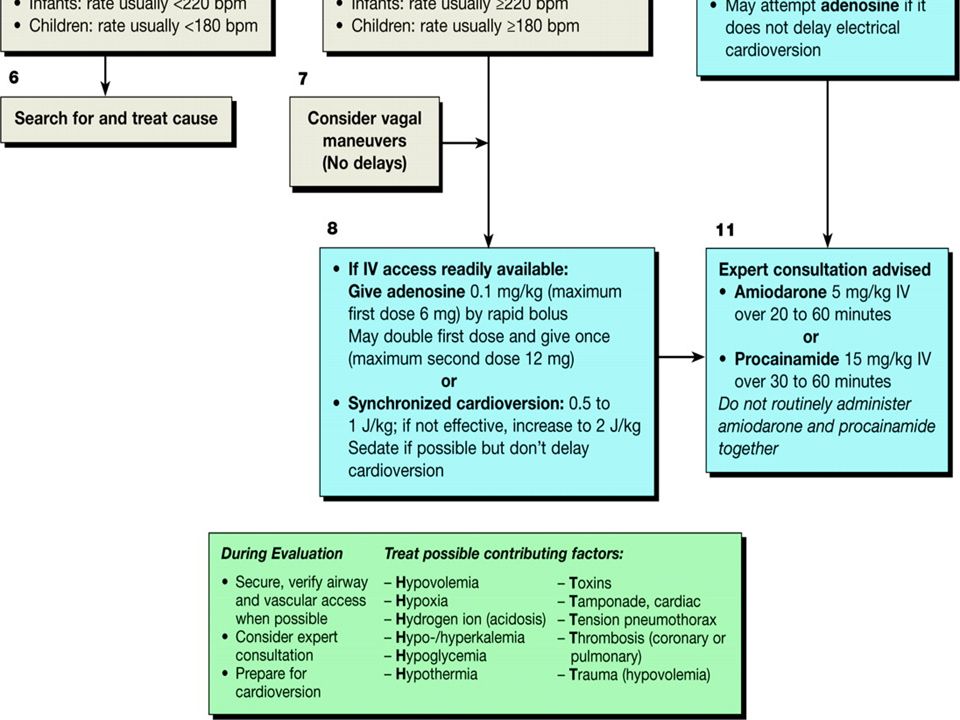
SUMMARY - FAST RATE Etiology Treatment Narrow QRS (Probable SVT)
Vagal Maneuver Adenosine (if IV access) Synchronized Cardio version Wide QRS (Probable VT) Amiodarone / Lidocaine / Procaineamide / Magnesium Sulphate
 Synchronized Cardio version. Wide QRS. (Probable VT) Amiodarone / Lidocaine / Procaineamide / Magnesium Sulphate.")
20
Drug Treatment of SVT- Adenosine
0.1 to 0.2 mg/kg Maximum single dose:12 mg

21
Bradyarrhythmia

22
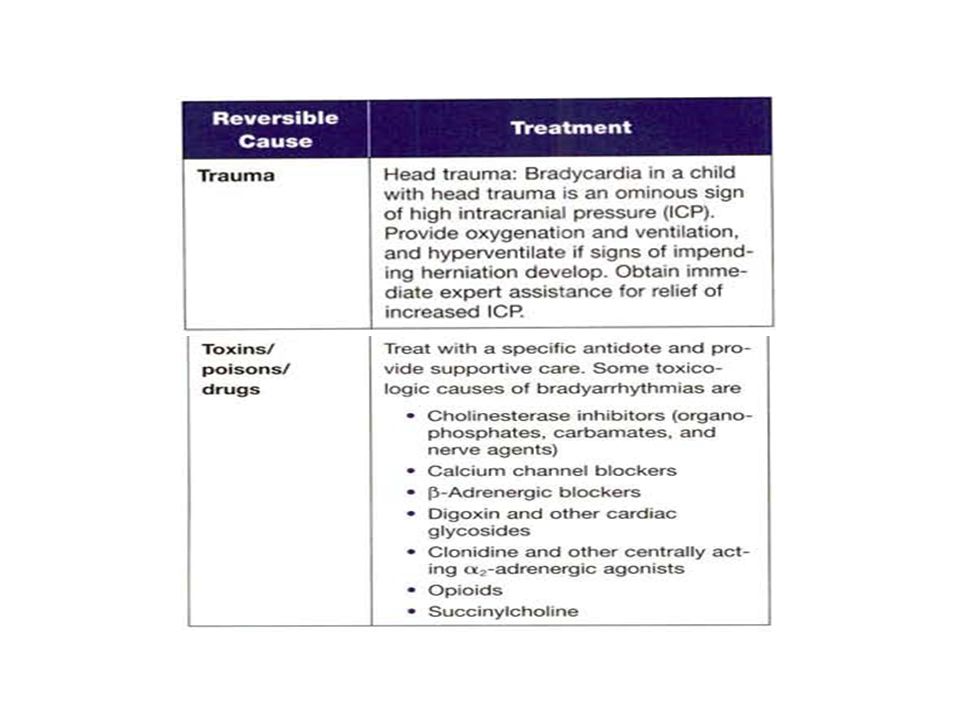
Etiology of Bradycardia
Hypoxia Hypothermia Head injury Heart Block Heart Transplant Toxins/poisons/drugs

23
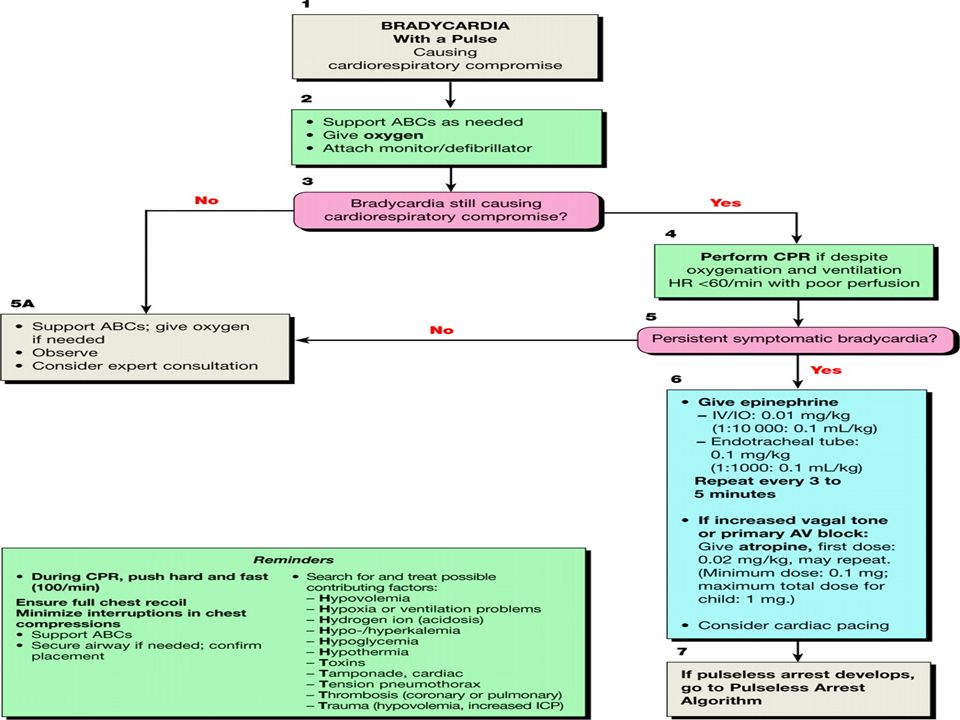
What Is the Rhythm? BRADYCARDIA

24
Management of Bradycardia
Oxygenation (FiO2 = 1.00) and ventilation Chest Compressions Epinephrine Dose: IO/IV, ml /kg of 1:10000 ET, 0.1 ml /kg of 1:1000 Atropine Dose : IO/IV: 0.02 mg/kg, Minimum 0.1 mg Maximum Single Dose (may repeat once) Child: 0.5mg, Adolescent: 1 mg ?? Pacing
 and ventilation. Chest Compressions. Epinephrine. Dose: IO/IV, 0.1 ml /kg of 1: ET, 0.1 ml /kg of 1:1000. Atropine. Dose : IO/IV: 0.02 mg/kg, Minimum 0.1 mg. Maximum Single Dose (may repeat once) Child: 0.5mg, Adolescent: 1 mg. Pacing.")
25
Treat potential reversible causes of Bradycardia

28
Case Study 8 year old submersion victim with Apnea No palpable pulses What Arrhythmias could be present?

29
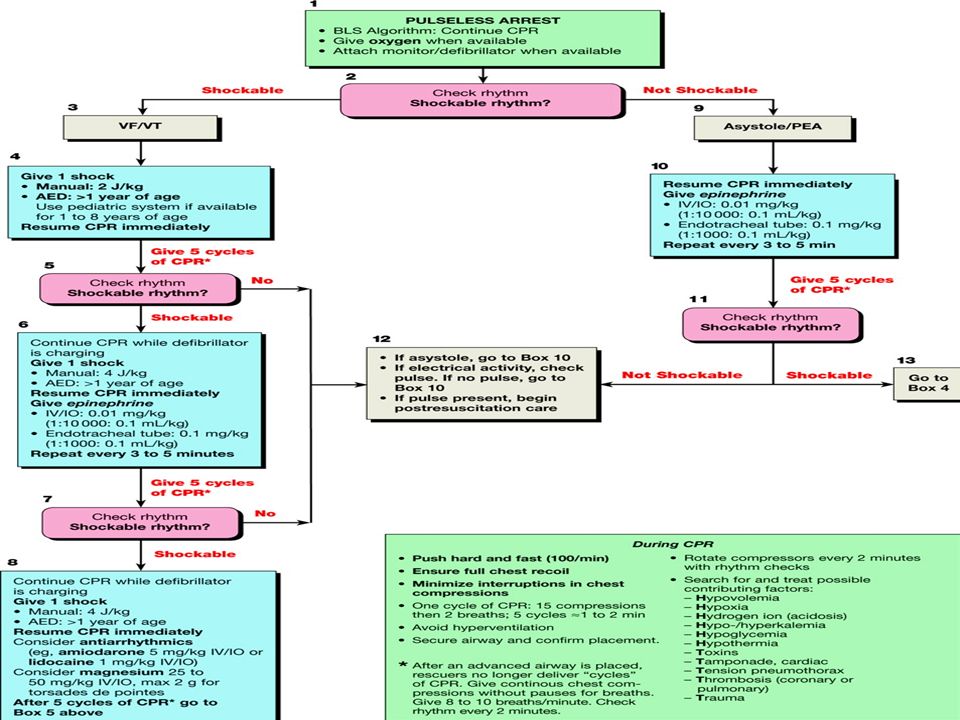
Absent Pulse Asystole Ventricular fibrillation Pulseless ventricular tachycardia Pulseless electrical activity / electromechanical dissociation

30
ASYSTOLE

31
Absent Pulse (Collapse Rhythms)-Asystole Treatment
CPR Secure airway Ventilate with 100% oxygen Obtain IV or IO access Epinephrine q 3-5 min

32
VENTRICULAR FIBRILLATION

34
Defibrillation - updates
First dose – 2 J / kg Second & subsequent dose – 4 J / kg Superiority & greater safety of biphasic over monophasic shocks & less energy requirement Drug administration during CPR Minimum interruptions in Chest Compressions

35
Defibrillation

36
starting with chest compression needed in all 3 post shock situations
High quality CPR starting with chest compression needed in all 3 post shock situations

37
Case Study A 2 year old child was struck by an automobile Respiratory rate = 0 Central pulse = absent

38
What are the priorities for treatment?
PULSELESS ELECTRICAL ACTIVITY Rhythm 60 beats/min What are the priorities for treatment?

39
Treat Cause

40
SUMMARY: Rx by Pulse Rate in a Child with Shock
TREATMENT FAST Synchronized Cardioversion Adenosine (in SVT if IV access +) SLOW Ventilation, oxygenation, compressions, epinephrine ABSENT CPR (beginning with chest compressions) VF/VT: immediate defibrillation PEA/EMD: Identify and treat the cause Epinephrine
 SLOW. Ventilation, oxygenation, compressions, epinephrine. ABSENT. CPR (beginning with chest compressions) VF/VT: immediate defibrillation. PEA/EMD: Identify and treat the cause. Epinephrine.")
41
Questions to answer in order to identify an unknown arrhythmia: :
Is the rate slow (<60 bpm) or fast (>100 bpm)? Slow - Suggests sinus bradycardia, sinus arrest, or conduction block Fast -Suggest increased/abnormal automaticity or reentry Is the rhythm irregular? Irregular -Suggests atrial fibrillation, 2nd degree AV block, Multifocal atrial tachycardia, or atrial flutter with variable AV block Is the QRS complex narrow or wide? Narrow - Rhythm must originate from the AV node or above Wide - Rhythm may originate from anywhere
 or fast (>100 bpm) Slow - Suggests sinus bradycardia, sinus arrest, or conduction block. Fast -Suggest increased/abnormal automaticity or reentry. 2. Is the rhythm irregular Irregular -Suggests atrial fibrillation, 2nd degree AV block, Multifocal atrial tachycardia, or atrial flutter with variable AV block. 3. Is the QRS complex narrow or wide Narrow - Rhythm must originate from the AV node or above. Wide - Rhythm may originate from anywhere.")
42
Questions to answer in order to identify an unknown arrhythmia: :
4. Are there P waves? Absent P waves - Suggests atrial fibrillation, ventricular tachycardia, or rhythms originating from the AV node 5. What is the relationship between the P waves and QRS complexes? More P waves than QRS complexes - Suggests 2nd or 3rd degree AV block More QRS complexes than P waves - Suggests an accelerated junctional or ventricular rhythm 6. Is the onset/termination of the rhythm abrupt or gradual? Abrupt - Suggests reentrant rhythm Gradual - Suggests altered automaticity

43
Treat The Patient Not The Rhythm

Similar presentations