Download presentation
Presentation is loading. Please wait.

1
Pathophysiology of the liver Tornóci László Institute of Pathophysiology Semmelweis University http://xenia.sote.hu/depts/pathophysiology

2
Significance of the liver Large organ of vital importance, 1-1.5 kg Filter, getting 1/4 of cardiac output –20% a. hepatica (systemic, oxygenated) –80% v. portae (rich in nutrients, deoxygenated) The central organ of biochemistry: –synthesis, excretion, metabolism, biotransformation (“detoxification”) Storage (nutrients, iron) Digestion (emulsification of fat)
 –80% v. portae (rich in nutrients, deoxygenated) The central organ of biochemistry: –synthesis, excretion, metabolism, biotransformation ( detoxification ) Storage (nutrients, iron) Digestion (emulsification of fat).")
3
Metabolic consequences of liver diseases carbohydrates –hyperglycemia (postprandial) –hypoglycemia (in alcoholics, after prolonged fasting) proteins: albumin, coagulation factors lipids:fatty liver decrease of catabolic/excretory function –e.g. estrogens, many drugs!

4
Clinical signs of liver diseases Nausea, temperature, fatigue Physical examination: –Palpable, tender liver, splenomegaly –jaundice (icterus), palmar erythema, spider naevi, excorations, less body hair –foetor hepatis Symptoms of portal hypertension –ascites, caput Medusae, esophageal varices Bleeding tendency Confusion, coma
, palmar erythema, spider naevi, excorations, less body hair –foetor hepatis Symptoms of portal hypertension –ascites, caput Medusae, esophageal varices Bleeding tendency Confusion, coma")
5
Major laboratory signs of liver diseases Enzyme activities –parenchymal (ALT, AST) –obstructive (alkaline phosphatase, GGT) bilirubin albumin, A/G prothrombin time antigens, antibodies
 –obstructive (alkaline phosphatase, GGT) bilirubin albumin, A/G prothrombin time antigens, antibodies")
6
Classification of liver diseases CauseClinical appearance hepatocellular (parenchymal) acute liver injury - atrophia hepatis flava chronic hepatitis cirrhosis hepatobiliar (cholestatic)obstructive jaundice vascular, other vascular, systemic, storage etc. diseases

7
Parenchymal liver diseases acquired –toxic effects (alcohol, mushroom, drug) –infections (hepatotropic and other viruses, etc) –autoimmune disorders congenital –inherited hyperbilirubinemias –other genetic syndromes (e.g. Wilson’s disease)
.")
8
Effect of alcoholism on the liver Fatty liver, alcoholic hepatitis, cirrhosis Threshold dose for liver injury –In men 60-80 g/day over years –In women 20-40 g/day It turns into severe, irreversible process in only 15 % of the cases The risk factors for this are unknown Undernutrition is not a risk factor

9
Less alcohol causes cirrhosis in women

10
Drug induced liver injury Dose dependent –acetaminophen: minimum 10-15 g, but 2 g may be enough in alcoholics (because of inducing P450 2E1) Idiosyncratic (independent of dose) –toxic reacion: halothane, methyldopa, phenytoin, “alternative medicines” –cholestasis: chlorpromazine, erythromycin, oral contraceptives, TPN
 Idiosyncratic (independent of dose) –toxic reacion: halothane, methyldopa, phenytoin, alternative medicines –cholestasis: chlorpromazine, erythromycin, oral contraceptives, TPN")
11
Hepatotropic viruses HAV (infectious hepatitis) HBV (serum hepatitis) HDV (delta agent, defect virus) HCV (parenteral nonA-nonB) HEV (enteral nonA-nonB) NANE (nonA-nonE) HGV (not significant clinically)
 HBV (serum hepatitis) HDV (delta agent, defect virus) HCV (parenteral nonA-nonB) HEV (enteral nonA-nonB) NANE (nonA-nonE) HGV (not significant clinically)")
12
Overview of viral hepatitis types Major route of infection Fulminant course % Becomes chronic % Prevention A fecal-oral0.1neverIG, vaccine B percutaneous perinatal sexual 0.1-11-10IG, vaccine C percutaneous0.150-70none D see HBV5-20 * see HBVHBV vaccine E water1-2 ** nevernone * : low in coinfection, high in superinfection **: 10-20% in pregnant women

13
Chronic hepatitis Caused by virus, drug or autoimmune disease Types of health problems caused –epidemiological (carriers of virus) –progressive liver damage is possible –may turn into cirrhosis –may cause hepatocellular carcinoma
 –progressive liver damage is possible –may turn into cirrhosis –may cause hepatocellular carcinoma")
14
Classification of chronic hepatitis The new classification is based on: –cause –grade (histologic assessment) –stage (by the degree of fibrosis) The old (histological) classification –chronic persistent hepatitis –chronic lobular hepatitis –chronic active hepatitis
 –stage (by the degree of fibrosis) The old (histological) classification –chronic persistent hepatitis –chronic lobular hepatitis –chronic active hepatitis")
15
Chronic viral hepatitis Huge epidemiological problem –no HBV vaccination programs in the developing countries yet The age and immune status determines whether the infection turns chronic –e.g. HBV infection becomes chronic in 90 % of newborns! Chronic HBV infections diagnosed in adults are not preceded by apparent acute hepatitis

16
HBV infection worldwide

17
Cirrhosis hepatis chronic, fibrotic process, leading to the progressive, irreversible destruction of liver parenchyma it can be caused by a number of chronic processes damaging the liver cells: –alcohol (Laennec cirrhosis) –chronic infection –biliary obstruction –congestion (cardiogenic cirrhosis) –inherited, metabolic disease
 –chronic infection –biliary obstruction –congestion (cardiogenic cirrhosis) –inherited, metabolic disease")
18
Survival of cirrhosis patients

19
Factors playing a role in the development of ascites

20
Factors that help hepatic coma to develop increased protein intake –e.g. bleeding from esophageal varices increased protein catabolism (infection, fever) alkalosis (intracellular trapping of ammonium)
 alkalosis (intracellular trapping of ammonium).")
21
Hepatic coma and blood ammonia levels

23
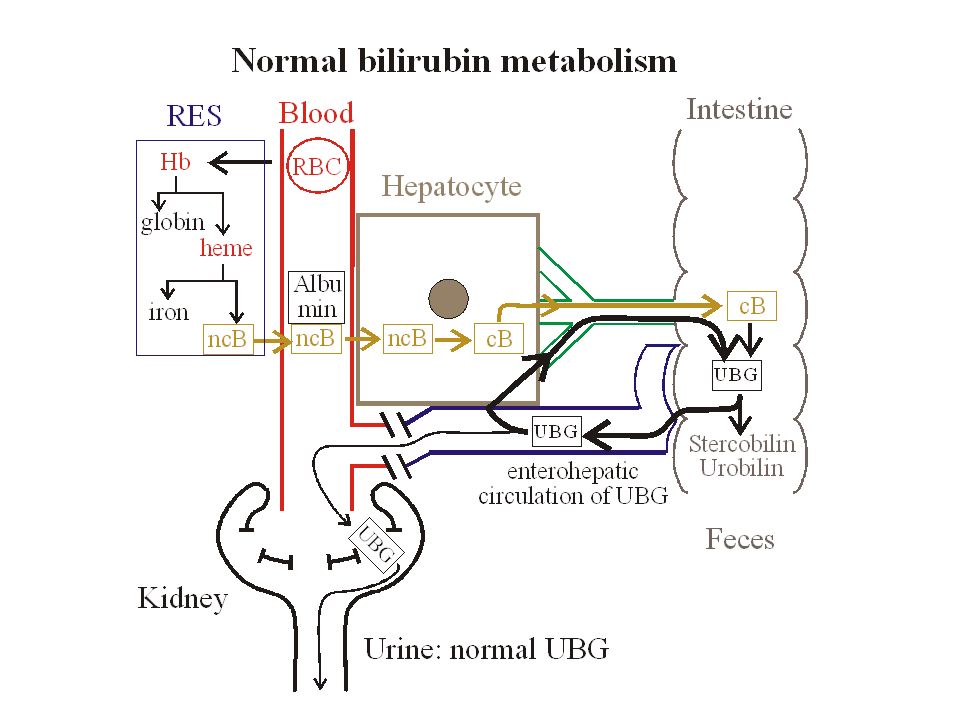
Inherited hyperbilirubinemias unconjugated –Gilbert (low UGT1A1 act., abnormal uptake) –Crigler-Najjar type I (no UGT1A1 act.) –Crigler-Najjar type II (medium UGT1A1 act.) conjugated –Dubin-Johnson (mutation of MRP2) –Rotor (unknown) UGT1A1 = bilirubin - UDP glucuronyl transferase MRP2 = multidrug resistance associated protein 2 (transports conjugated bilirubin into the bile)
 –Crigler-Najjar type I (no UGT1A1 act.) –Crigler-Najjar type II (medium UGT1A1 act.) conjugated –Dubin-Johnson (mutation of MRP2) –Rotor (unknown) UGT1A1 = bilirubin - UDP glucuronyl transferase MRP2 = multidrug resistance associated protein 2 (transports conjugated bilirubin into the bile)")
Similar presentations










>")
 LIVER FUNCTION AND THE BILIARY TRACT LECTURE FOUR Dr. Essam H. Aljiffri.>")
 that progresses to cirrhosis Replacement of liver tissue.>")
 LIVER FUNCTION AND THE BILIARY TRACT LECTURE FIVE Dr. Essam H. Aljiffri.>")





