Download presentation
Presentation is loading. Please wait.

1
Optimisation of Computed Radiography chest imaging utilising a digitally reconstructed radiograph simulation technique Craig Moore Radiation Physics Service Hull & East Yorkshire Hospitals NHS Trust www.hullrad.org.uk

2
Introduction - Literature Lots of publications have shown that patient anatomy is the limiting factor in the reading normal structures, and detection of lesions (lung nodules) in chest images –Bochud et al 1999 –Samei et al 1999, 2000 –Burgess et al 2001 –Huda et al 2004 –Keelan et al 2004 –Sund et al 2004 –Tingberg et al 2004 European wide RADIUS chest trial (2005)
 in chest images –Bochud et al 1999 –Samei et al 1999, 2000 –Burgess et al 2001 –Huda et al 2004 –Keelan et al 2004 –Sund et al 2004 –Tingberg et al 2004 European wide RADIUS chest trial (2005)")
3
Introduction - Literature Chest radiography is now generally considered to be limited by the projected anatomy Patient anatomy = anatomical noise So if we want to optimize digital system for chest imaging, vital that anatomical noise is present in the images!!!

4
Introduction However, the radiation dose/image quality relationship must not be ignored Doses must be kelp ALARP –ICRP 2007 –IR(ME)R2000 – (required legally in the UK) We would therefore want system (quantum) noise present in an image for dose reduction studies
R2000 – (required legally in the UK) We would therefore want system (quantum) noise present in an image for dose reduction studies")
5
Digitally Reconstructed Radiograph (DRR) Hypothesis: –Can use CT data of humans to provide realistic anatomy (anatomical noise) Clinically realistic computerized ‘phantom’ –Simulate the transport of x-rays through the ‘phantom’ and produce a digitally reconstructed radiograph (DRR – a simulation of a conventional 2D x-ray image created from CT data) –Add frequency dependent system noise post DRR calculation –Add radiation scatter post DRR calculation –Validate –Use for optimization studies
 Hypothesis: –Can use CT data of humans to provide realistic anatomy (anatomical noise) Clinically realistic computerized ‘phantom’ –Simulate the transport of x-rays through the ‘phantom’ and produce a digitally reconstructed radiograph (DRR – a simulation of a conventional 2D x-ray image created from CT data) –Add frequency dependent system noise post DRR calculation –Add radiation scatter post DRR calculation –Validate –Use for optimization studies")
6
DRR Algorithm: Virtual Patient Virtual patient derived from chest portion of real CT datasets Voxel resolution = 0.34 x 0.34 x 0.8 mm CT number converted to linear attenuation coefficient (LAC) using tissue equivalent inserts –Measure mean CT No. in each insert –We know elemental composition of each so can derive LAC –Can derive relationship between CT No. and LAC

7
PA slice 1 PA slice N CT axial batch 1 (i.e. CT slices 1 to 20) CT axial batch 2 (i.e. CT slices 21 to 40) Final CT axial batch (i.e. slices 681 to 700) CT dataset re- orientated in the ‘PA’ direction X-ray spectra derived from IPEM 78 X-ray attenuated exponentially through CT dataset using a ray casting method of DRR calculation Energy absorbed in CR phosphor Intensity of X-rays exiting is calculated
 Final CT axial batch (i.e. slices 681 to 700) CT dataset re- orientated in the ‘PA’ direction X-ray spectra derived from IPEM 78 X-ray attenuated exponentially through CT dataset using a ray casting method of DRR calculation Energy absorbed in CR phosphor Intensity of X-rays exiting is calculated.")
8
Scatter Addition Must add to DRR generated image –DRR algorithm does not calculate scatter Measured scatter in CR chest images using lead pellet array Use chest portion of RANDO phantom

9
Noise Addition Uniform noise image Corrected noise image lung spine diaphragm Based on slightly modified work by Bath et al, 2005

10
Lung Nodule Simulation Added artificial nodules to the CT data prior to X- ray projection Baed on work by Li et al 2009

11
Human DRR v Human CR DRR CR

12
DRRs: 50 kVp v 150 kVp

13
Scatter Rejection The DRR algorithm can produce images with scatter rejection (b) (c) (a) DRR CR DRR No RejectionDRR GridCR Grid
 (c) (a) DRR CR DRR No RejectionDRR GridCR Grid")
14
Obese Patients DRR algorithm can also produce images of large/obese patients (a) (b) DRRCR
 (b) DRRCR")
15
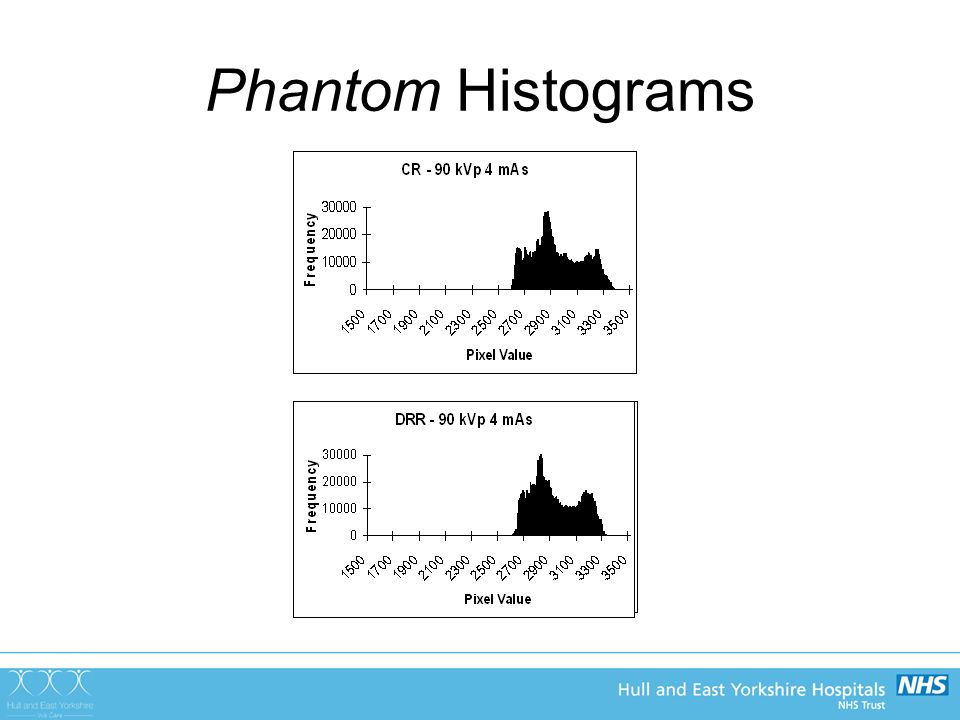
Validation Decided to validate with RANDO and real patient images: –Histogram of pixel values –Signal to noise ratios (SNR) Important because signal and noise affects the visualisation of pathology –Tissue to rib ratios (TRR) Pixel value ratio of soft tissue to that of rib Important as rib can distract the Radiologist from detecting pathology
 Important because signal and noise affects the visualisation of pathology –Tissue to rib ratios (TRR) Pixel value ratio of soft tissue to that of rib Important as rib can distract the Radiologist from detecting pathology")
16
Phantom Histograms a b c d

18
PATIENT - Histograms Typical histogram of average patient DRR Typical histogram of average patient CR image

19
SNRs Good agreement in lung, spine and diaphragm areas of chest Maximum deviation approx 15% –Mean deviation = 7% Addition of frequency dependent noise not perfect: –CR system noise is ergodic (changes with time) –Noise added here is a snapshot (and so not ergodic) –However, quantum noise dominates over ‘ergodic noise’ so not such an issue –DQE is NOT constant with dose variation in image
 –Noise added here is a snapshot (and so not ergodic) –However, quantum noise dominates over ‘ergodic noise’ so not such an issue –DQE is NOT constant with dose variation in image")
20
Validation - TRRs Good agreement –Within 2% As tube potential increases TRR decreases –Due to rib attenuating higher percentage in incident photons at lower potentials than soft tissue, thus forcing up TRR

21
Validation - Radiologists Have told me DRR images contain sufficient clinical data to allow diagnosis and subsequent optimisation They have scored the images out of 10 –‘are the images sufficiently like real CR images? –Average score of 7.8

22
Conclusions – DRR Algorithm DRR computer program has been produced that adequately simulates chest radiographs of average and obese patients –Anatomical noise simulated by real human CT data –System noise and scatter successfully added post DRR generation that provides: SNRs TRRs Histograms –in good agreement with those measured in real CR images Provides us with a tool that can be used by Radiologists to grade image quality with images derived with different x-ray system parameters WITHOUT THE NEED TO PERFORM REPEAT EXPOSURE ON PATIENTS ACCEPTED FOR PUBLICATION IN THE BJR –AUGUST 2011

23
Optimisation of CR Chest Radiography using DRR Generated Images In Hull chest exposure factors were not standardised (historical reasons!!!!) Three main hospital sites: –60 kVp & 10 mAs –70 kVp & 5 mAs –80 kVp & 5 mAs In the last 6 months, four expert image evaluators have scored DRR reconstructed images –Two Consultant Radiologists –Two Reporting Radiographers Scoring criteria based on European guidelines (CEC)
 Three main hospital sites: –60 kVp & 10 mAs –70 kVp & 5 mAs –80 kVp & 5 mAs In the last 6 months, four expert image evaluators have scored DRR reconstructed images –Two Consultant Radiologists –Two Reporting Radiographers Scoring criteria based on European guidelines (CEC)")
24
What to Optimise? Optimum tube potential for Average Patients (70 kg ± 10 kg) –Without scatter rejection (as per Hull protocol) –With scatter rejection (grid and air gap) Optimum tube potential for Obese patients –Without scatter rejection –With scatter rejection Is Scatter rejection indicated? Dose reduction?
 –Without scatter rejection (as per Hull protocol) –With scatter rejection (grid and air gap) Optimum tube potential for Obese patients –Without scatter rejection –With scatter rejection Is Scatter rejection indicated. Dose reduction .")
25
Scoring Criteria Images scored on a dual PACS monitor system Image on right hand screen held at a constant kVp Images on left hand screen displayed from 50 to 150 kVp in steps of 10kVp (approx) –Image 1 = 50 kV –Image 2 = 60 kV –Image 10 = 150 kV Test images scored against reference image All images matched effective dose
 –Image 1 = 50 kV –Image 2 = 60 kV –Image 10 = 150 kV Test images scored against reference image All images matched effective dose")
26
GRADINGVISIBILITY OF STRUCTURE -3Definitely inferior to the reference image -2Reasonably inferior to the reference image Slightly inferior to the reference image 0Equal to the reference image +1Slightly better than the reference image +2Reasonably better than the reference image +3Definitely better than the reference image [1][1] European guidelines on quality criteria for diagnostic radiographic images. CEC European Commission EUR 16260 EN (Luxembourg 1996) STUCTURE – NORMAL ANATOMYGRADING IMAGE 1IMAGE 2 IMAGE 3IMAGE 4 Vessels seen approx approx 3 cm from the pleural margin Thoracic vertebrae behind the heart Retrocardiac vessels Pleural margin Vessels seen en face in the central area Hilar region STUCTURE – LUNG NODULES GRADING Nodule in lateral pulmonary region Nodule in hilar region Are the ribs a distraction? Y/N
![GRADINGVISIBILITY OF STRUCTURE -3Definitely inferior to the reference image -2Reasonably inferior to the reference image Slightly inferior to the reference image 0Equal to the reference image +1Slightly better than the reference image +2Reasonably better than the reference image +3Definitely better than the reference image [1][1] European guidelines on quality criteria for diagnostic radiographic images.](http://images.slideplayer.com/28/9290174/slides/slide_26.jpg "CEC European Commission EUR EN (Luxembourg 1996) STUCTURE – NORMAL ANATOMYGRADING IMAGE 1IMAGE 2 IMAGE 3IMAGE 4 Vessels seen approx approx 3 cm from the pleural margin Thoracic vertebrae behind the heart Retrocardiac vessels Pleural margin Vessels seen en face in the central area Hilar region STUCTURE – LUNG NODULES GRADING Nodule in lateral pulmonary region Nodule in hilar region Are the ribs a distraction. Y/N.")
27
Tube Potential Optimisation

28
Results – Average Sized Patients, no scatter rejection VGAS = average of Radiologists results

29
Results – Average Patients with scatter rejection - grid

30
Results – Average Patients with scatter rejection – air gap

31
Results – Obese Patients without scatter rejection

32
Very weak trend for better image quality with higher kVp Lower kVps probably ‘worse’ due to combination of: –Lack of penetration through obese patient –Increased scatter from obese patient (scatter to cassette changes very little with kVp) This is not so with average patients –Less tissue (fat) so more radiation penetration –Less scatter from fat It is likely that poorer radiation penetration and increased scatter from obese patient outweighs the inherent benefit of photoelectric contrast obtained from lower kVps
 This is not so with average patients –Less tissue (fat) so more radiation penetration –Less scatter from fat It is likely that poorer radiation penetration and increased scatter from obese patient outweighs the inherent benefit of photoelectric contrast obtained from lower kVps")
33
Results – Obese Patients with scatter rejection - grids

34
Results – Obese Patients with scatter rejection – air gap

35
Scatter Rejection

36
Scatter Rejection vs no scatter rejection – average patients

37
Superior image quality with scatter rejection technique Grids performed much better than air gap Statistically significant differences BUT: –Image evaluators were asked if increase in dose due to use of grids was justified, even with better image quality –Answer in 100% of cases was NO –SCATTER REJECTION FOR AVERAGE PATIENTS IS NOT INDICATED

38
Exposure time for average patients without scatter rejection and low tube potentials? Scatter rejection not indicated Therefore low kVps should be used (remember the graph) European guidance recommends exposure times < 20 ms Can we achieve this with low kVps?? Modern Philips X-ray generator: –For lgM = 2 (Agfa CR specific Dose Indicator) –With 630 mA, all kVps are possible –Max exp time = 16 ms At the expense of increased tube loading
 European guidance recommends exposure times < 20 ms Can we achieve this with low kVps . Modern Philips X-ray generator: –For lgM = 2 (Agfa CR specific Dose Indicator) –With 630 mA, all kVps are possible –Max exp time = 16 ms At the expense of increased tube loading.")
39
Scatter Rejection vs no scatter rejection – obese patients

40
Superior image quality with scatter rejection technique Grids performed much better than air gap Statistically significant differences BUT: –Image evaluators were asked if increase in dose due to use of grids was justified, even with better image quality –Answer in 100% of cases was YES –ANTI SCATTER GRID USE FOR OBESE PATIENTS IS INDICATED

41
Exposure times for obese patients with an anti-scatter grid Remember that low tube potentials were superior with an anti-scatter grid!!!! Need exposure times < 20ms Is this possible with low kVps and scatter grid for lgM = 2?? Scatter grid is a focused grid so have to use it in a fixed range of FDD –Nominal distance = 140 cm FDD –Range allowed = 115cm – 180cm At 140 cm FDD lowest exp time = 17.6ms @ 109 kVp At 115cm FDD lowest exp time = 20 ms @ 90 kVp So are limited to 90 kVp

42
Dose Reduction

43
Dose Reduction? Images were also presented at different doses

44
Dose reduction? Results suggest doses can be reduced by around 50% before image quality begins to suffer and become unacceptable Therefore could half exposure mAs

45
Conclusions – Use of DRR algorithm to optimise CR chest imaging Average patients: –No scatter rejection is indicated –Therefore, low kVps (< 102 kVp) are indicated –Can have exposure times < 20 ms for all kVps Obese patients –Anti-scatter grid is indicated –So low kVps (<102kVp) should be used –For exposure times < 20ms, are limited to 90 kVp Doses –As low as 50% reduction possible ACCEPTED FOR PUBLICATION IN BJR
 are indicated –Can have exposure times < 20 ms for all kVps Obese patients –Anti-scatter grid is indicated –So low kVps (<102kVp) should be used –For exposure times < 20ms, are limited to 90 kVp Doses –As low as 50% reduction possible ACCEPTED FOR PUBLICATION IN BJR")
46
Optimisation & Standardisation in Hull? Agreed with Consultant Radiologists: –60 kVp & 10 mAs After a ‘settling in’ period: –60 kVp & 8 mAs –Want to go lower than 8mAs eventually!!! Implication on patient dose? –Using PCXMC effective dose calculation software: –80 kVp/5 mAs = 0.011 mSv –60 kVp/8 mAs = 0.006 mSv –Approx 45% drop in effective dose

Similar presentations