Download presentation
Presentation is loading. Please wait.

1
Urethral Obstruction Jerry G. Blaivas, MD Clinical Professor of Urology Weil Cornell Medical College New York Presbyterian Medical Center Adjunct Professor of Urology SUNY Downstate Medical Center

2
Urethral Obstruction Incidence: 2 - 29% of women with persistent LUTS Symptoms: nothing characteristic – storage 29% – voiding 8% – both 63% B Blaivas & Groutz,, Neurourol & Urodynam 19:553, 2000; Nitti et al, J Urol, 1999

3
Diagnosis Suspect in: –all women with low Q –with grade 3 & 4 POP –sx onset after incontinence/ prolapse surgery Urodynamics (synchronous pdet / Q) Cystoscopy
 Cystoscopy")
4
Urethral obstruction High detrusor pressure (pdet > 20 cm H 2 0) Low uroflow (Qmax < 12 ml/S)
 Low uroflow (Qmax < 12 ml/S)")
5
2 Strss High pressure Low flow

6
Impaired Detrusor Contractility Weak & or poorly sustained detrusor contraction (pdet < 20 cm H 2 0) Low flow (Qmax < 12 ml/S)
 Low flow (Qmax < 12 ml/S)")
7
JK Low pressure Low flow

8
Blaivas - Groutz Nomogram

9
Diagnosis ”…radiographic evidence of obstruction…in the presence of a sustained detrusor contraction.” No specific UDS criteria Obstructed women had: –lower Qmax –higher Pdet@Qmax –higher PVR 23% of 331 women were obstructed Nitti et al, J Urol, 1999

10
Caveats A pressure flow diagnosis is usually definitive, but An acontractile detrusor or impaired detrusor contractility does not rule out obstruction Persistent voiding dysfunction after incontinence surgery is usually due to obstruction

11
Etiology Groutz et al, Neurourol Urodyn 19:213,2000; Nitti et al., 1999 Prior surgery 14 - 30% Prolapse 29% Stricture 15% 1 O bladder neck obstruction 10 - 16% DESD 6% Dysfunction voiding 6 - 33% Urethral diverticulum 4%

12
Urethral Obstruction in women Anatomic Functional

13
Anatomic Urethral Obstruction Compression Post surgical Prolapse Urethral Diverticulum Tumor Urethral stricture Post surgical Traumatic Idiopathic Atrophy

14
Functional Urethral Obstruction Primary vesical neck Neurogenic Acquired behavior

15
Rx Anatomic Urethral Obstruction Intermittent catheterization Surgery - depends on the cau se: –correct prolapse –sling incision / urethrolysis –urethral diverticulectomy –urethroplasty

16
Rx Functional Urethral Obstruction Primary vesical neck TUI / TUR of vesical neck ? Alpha adrenergic antagonists Neurogenic Intermittent catheterization +/- anticholinergics Botox enterocystoplasty Dysfunctional voiding Bmod / biofeedback / neuromodulation

17
Anatomic Urethral Obstruction Compression Post surgical Prolapse Urethral Diverticulum Tumor Urethral stricture Post surgical Traumatic Idiopathic Atrophy

18
MSCO High pressure Low flow

21
Rx of Post-op Obstruction First 3 months – monitoring vs intervention May experience improvement Depends on procedure done After 3 months Improvement unlikely Definitive treatment

22
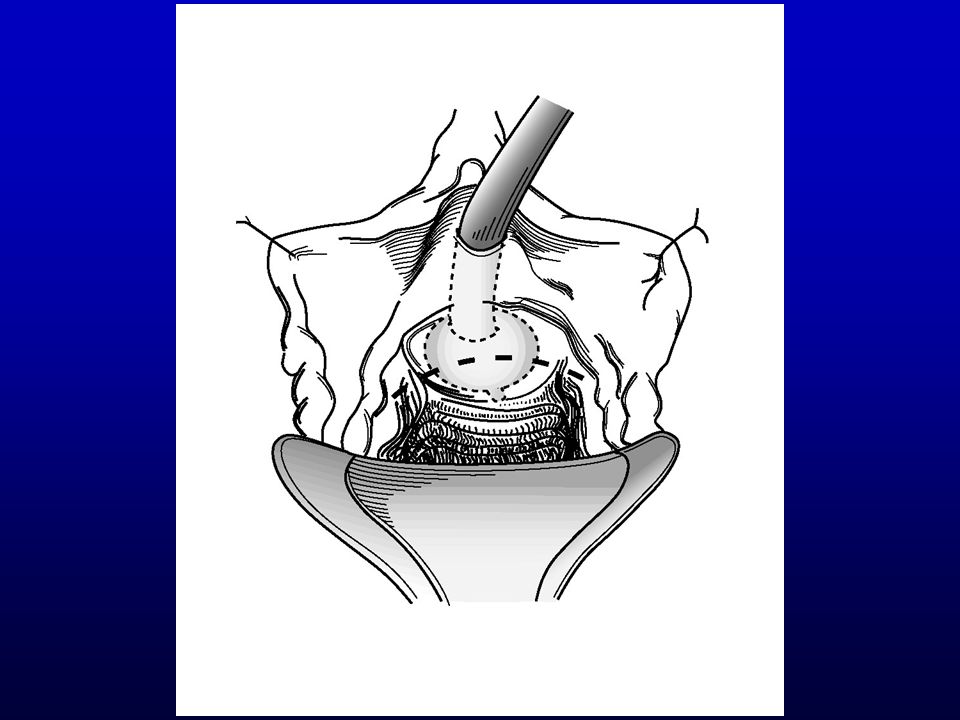
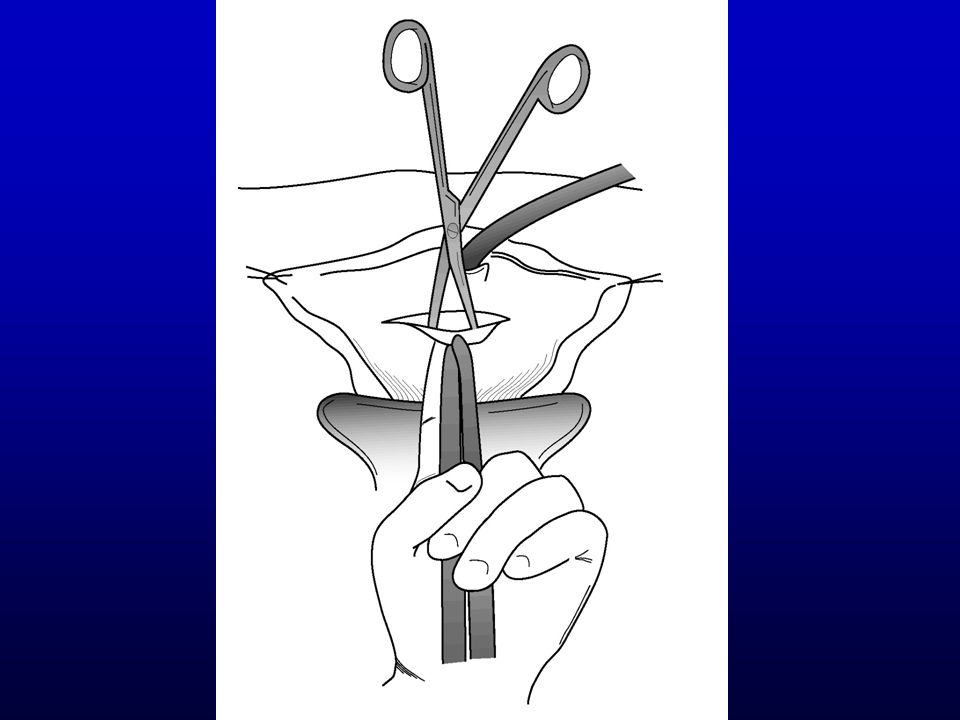
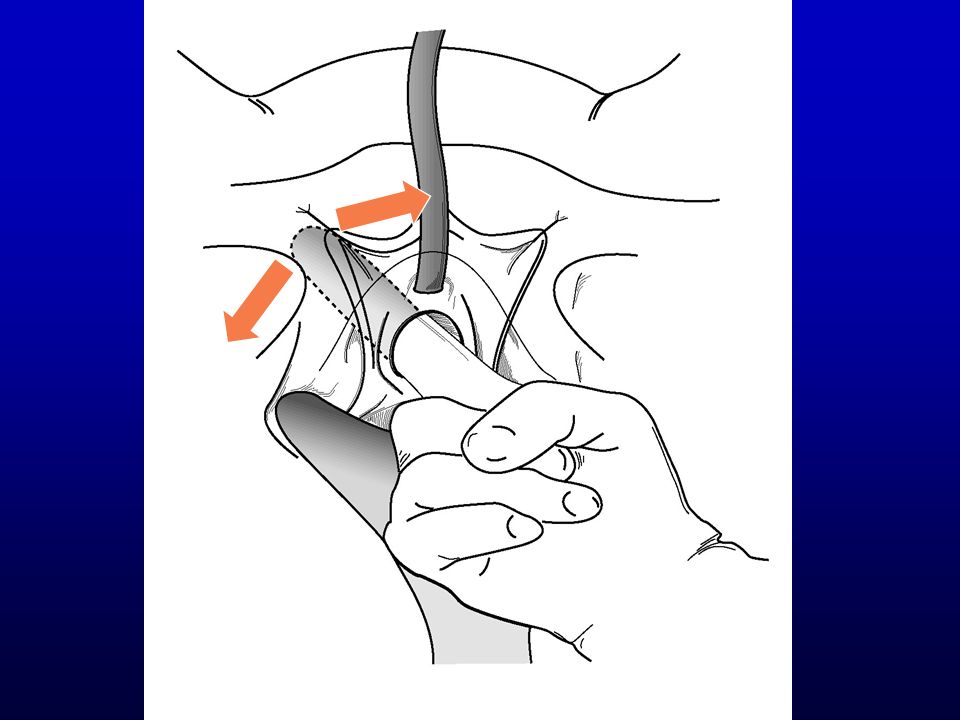
Mid Urethral Sling Loosening (1-2 weeks) Local anesthesia Open vaginal suture line Hook sling with a right-angle clamp Spread clamp or downward traction on the tape will usually loosen it (1-2 cm) If the tape is fixed, it can be cut
 Local anesthesia Open vaginal suture line Hook sling with a right-angle clamp Spread clamp or downward traction on the tape will usually loosen it (1-2 cm) If the tape is fixed, it can be cut")
23
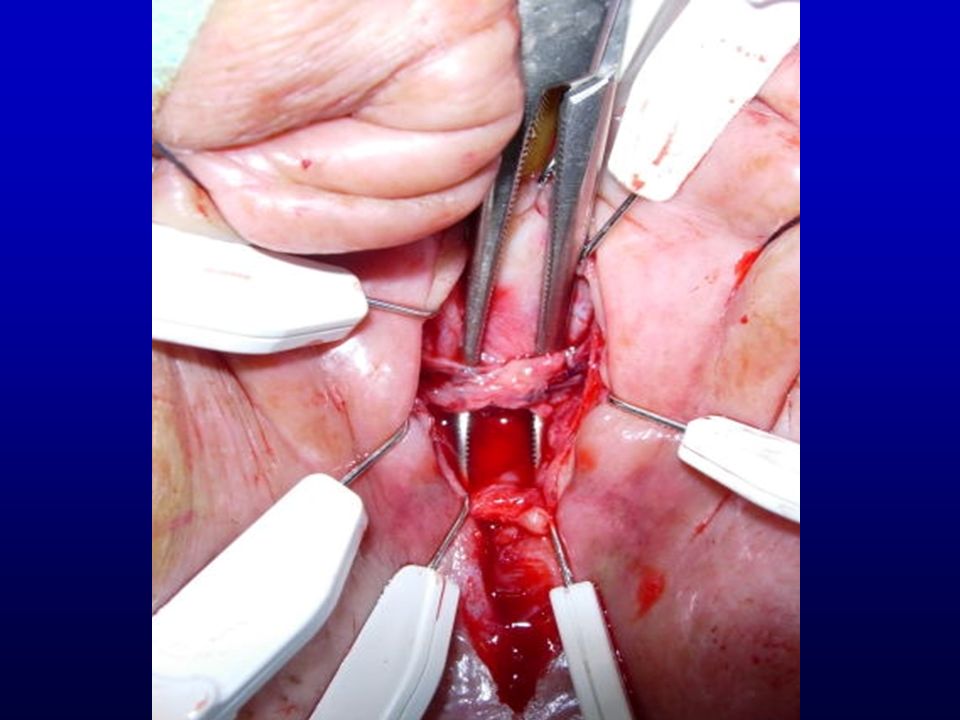
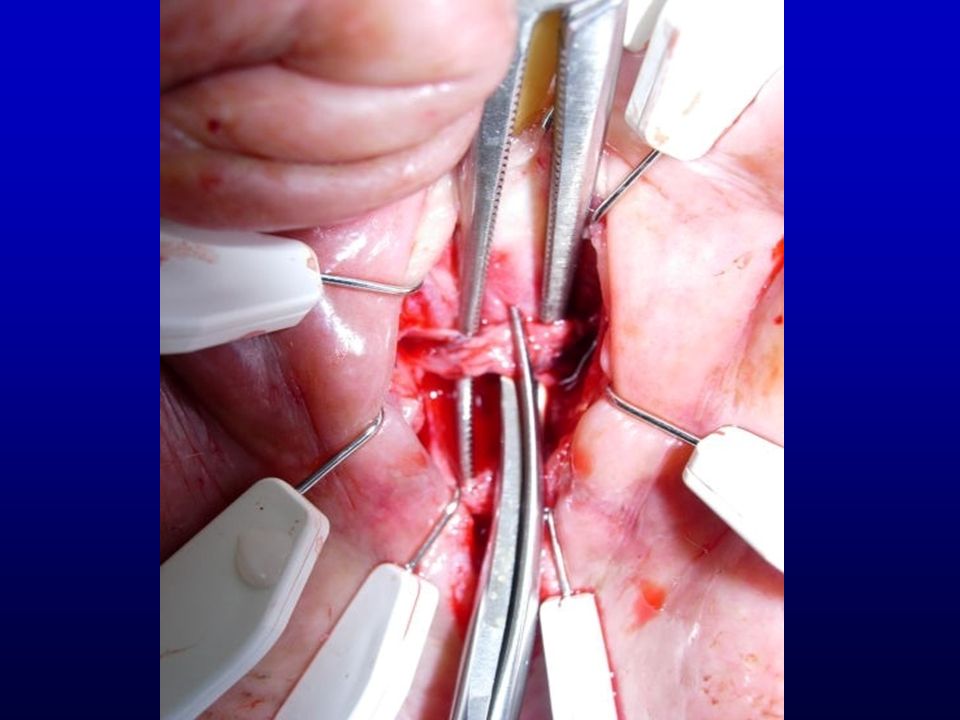
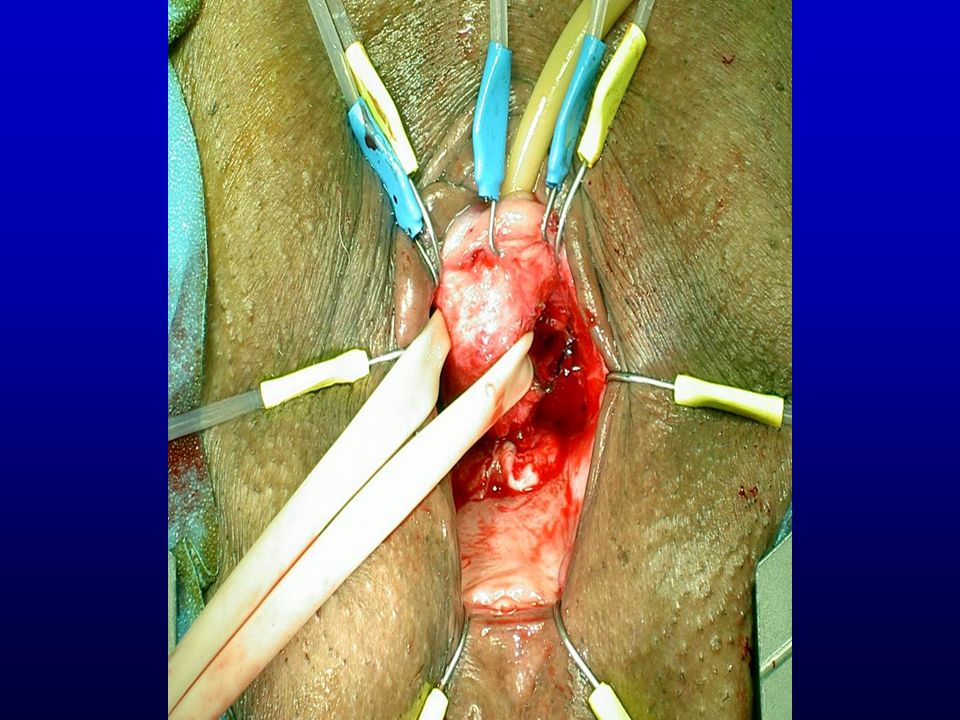
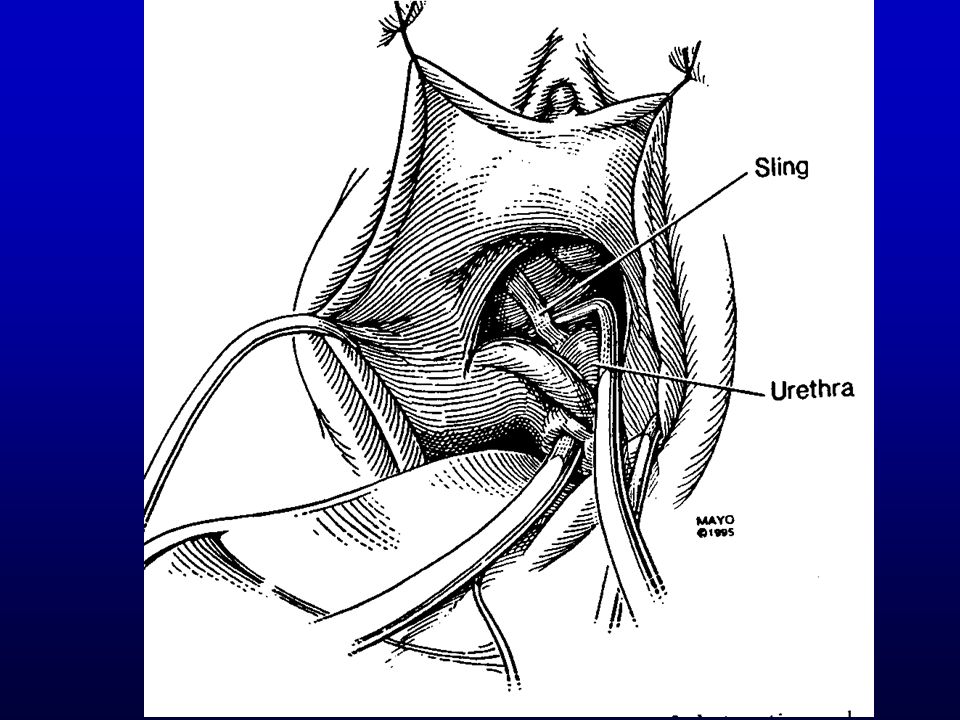
Sling Incision Pull down on Foley and palpate sling Inverted U or midline incision Begin urethral dissection just proximal to sling Isolation of sling in the midline or lateral Incision of the sling Nitti VW, Carlson KV, Blaivas JG, Dmochowski RR, Urology 59:47, 2002

24
DS

25
Sling Incision Sling should spring apart If not, dissect it from urethra +/- urethrolysis

29
TVT Intervention Results N Type Success Klutke, et al* 17 Midline Incision100% normal emptying Rardin, et al** 23 Midline Incision 100% normal emptying Loosening 30% complete resol. irritative sx 70% partial resol. irritative sx * Recurrent SUI in 6% ** Significant recurrent SUI 13% 26% recurrent SUI, but significantly better than prior to TVT

30
Sling Incision Results N Type Success SUI Klutke, et al Urology 58:697, 2001 Nitti, et al 19Midline Incision84% 17% Amundsen, et al 32Various 94% retention 9% 67% UUI Goldman 14Midline Incision93% 21%

31
Ureth rolysis Transvaginal Anterior vaginal wall Suprameatal Retropubic

32
Transvaginal Urethrolysis Inverted U incision Lateral dissection superficial to PCV Endopelvic fascia perforated & retropubic space entered

33
Transvaginal Urethrolysis Sharp and blunt dissection urethra freed from lateral attachments & undersurface of the pubic bone Index finger placed between pubic bone and urethra +/- Martius flap interposition

43
Suprameatal Urethrolysis

48
Urethrolysis Results N Type SuccessSUI Foster & McGuire 48Transvaginal 65% 0 Nitti & Raz 42Transvaginal 71% 0 Cross, et al 39Transvaginal 72% 3% Goldman, et al 32Transvaginal 84% 19% Petrou, et al 32Suprameatal 67% 3% Webster & Kreder 15Retropubic 93% 13% Petrou & Young12Retropubic 83% 18% Carr & Webster 54Mixed 78% 14%

49
Retropubic Urethrolysis Mobilization of urethra by sharp dissection Restore complete mobility to anterior vaginal wall Paravaginal repair Interposition of omentum between urethra and pubic bone

50
Anatomic Urethral Obstruction Compression Post surgical Prolapse Urethral Diverticulum Tumor Urethral stricture Post surgical Traumatic Atrophy

51
Pdet @ Qmax = 36cm H2O Qmax = 8 ml/S

52
symphysis urethra

53
Pdet @ Qmax = 54 cm H2O Qmax = 2 ml/S,

54
symphysis Prolapsed bladder

55
Anatomic Urethral Obstruction Compression Post surgical Prolapse Urethral Diverticulum Tumor Urethral stricture Post surgical Traumatic Atrophy

56
FS pdet@Qmax = 68 cm H 2 0 Qmax = 5 ml/S Tic

57
Anatomic Urethral Obstruction Compression Post surgical Prolapse Urethral Diverticulum Tumor Urethral stricture Post surgical Traumatic Atrophy

59
Anatomic Urethral Obstruction Compression Post surgical Prolapse Urethral Diverticulum Tumor Urethral stricture Post surgical Traumatic Idiopathic Atrophy

60
pdet@Qmax = 25 cm H20 Qmax = 0.5 mL/S

61
Urethral diverticulum Bladder diverticulum Urethra

62
Anatomic Urethral Obstruction Compression Post surgical Prolapse Urethral Diverticulum Tumor Urethral stricture Post surgical Traumatic Idiopathic Atrophy

63
JTJT JT pdet@Qmax = 75 cm H 2 0 Qmax = 8 ml/S Urethral obstruction

64
stricture

65
Anatomic Urethral Obstruction Compression Post surgical Prolapse Urethral Diverticulum Tumor Urethral stricture Post surgical Traumatic Idiopathic Atrophy

66
pdet@Qmax = 100 cm H 2 0 Qmax = 0.5 mL/S

67
stricture

68
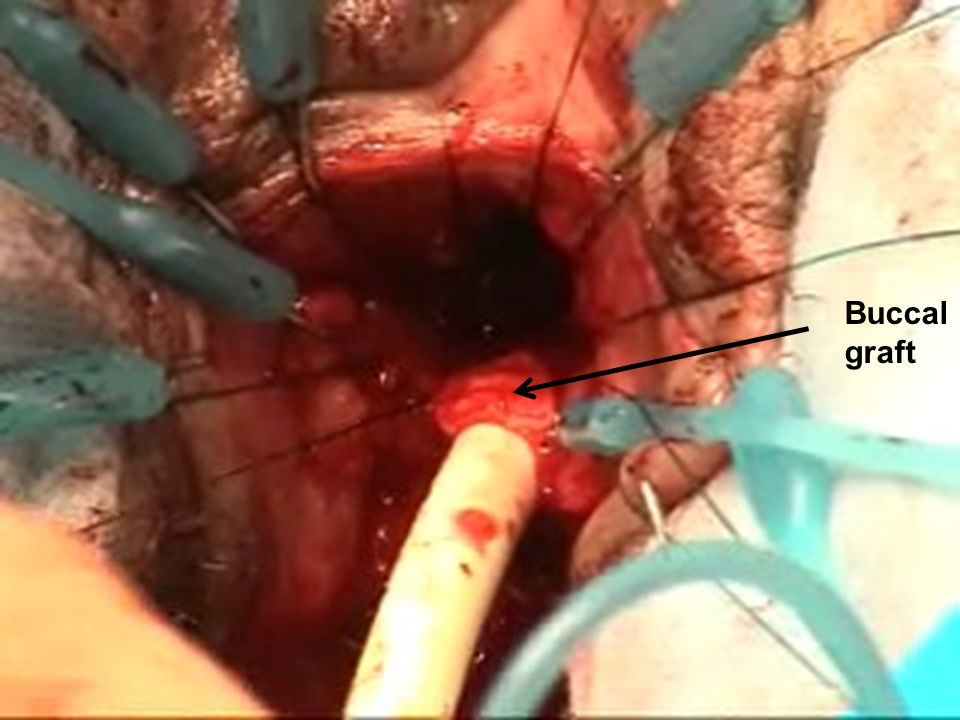
Surgical Rx of Stricture Urethral dilation Urethrotomy Urethroplasty Ventral flap Dorsal graft

69
Buccal graft

71
Anatomic Urethral Obstruction Compression Post surgical Prolapse Urethral Diverticulum Tumor Urethral stricture Post surgical Traumatic Idiopathic Atrophy

72
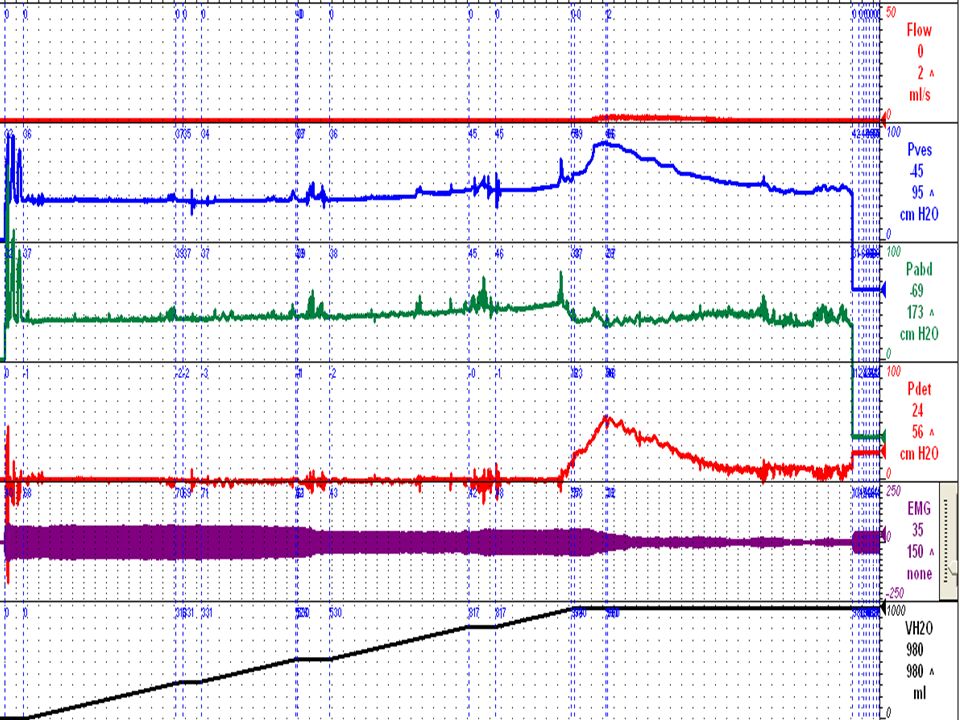
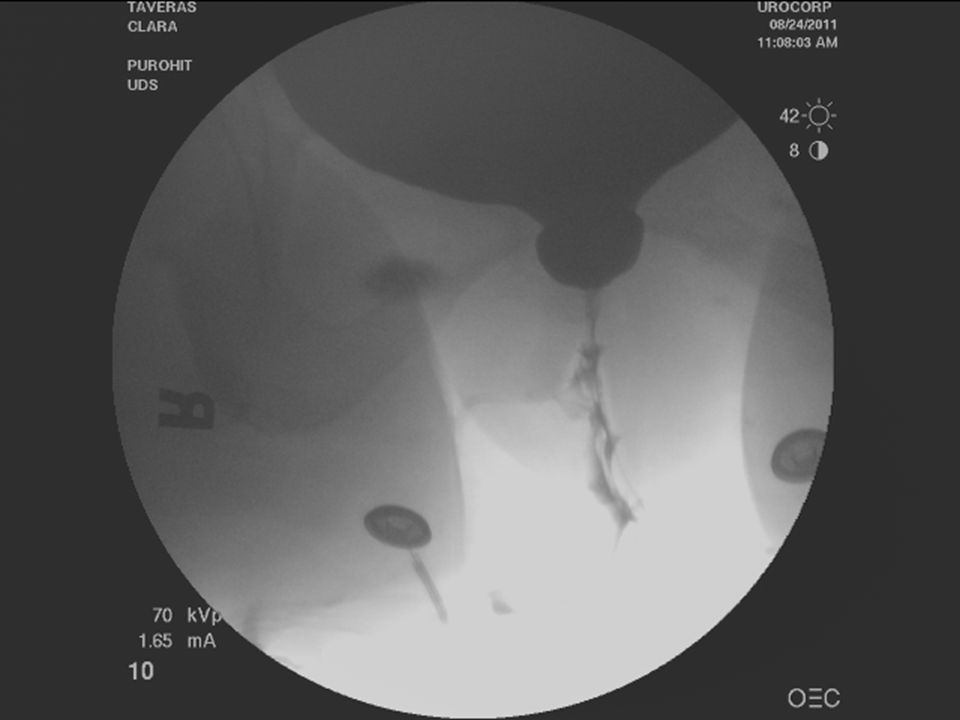
RSN pdetmax = 90 cm H 2 0 Qmax = 7 ml/S

73
RSN urethra diverticula

74
Functional Urethral Obstruction Primary vesical neck Neurogenic Acquired behavior

75
2 Strss pdet@Qmax = 150 cm H20 Qmax = 1 ml/S

77
Rx Primary Vesical Neck Obstruction Alpha adrenergic blockade Bladder neck incision Bladder neck resection

78
Functional Urethral Obstruction Primary vesical neck Neurogenic Acquired behavior

79
PS Involuntary detrusor contraction Involuntary sphincter contraction Obstruction due to sphincter contraction

80
CG Involuntary detrusor contraction Involuntary sphincter contraction Vesical neck obstruction

81
Functional Urethral Obstruction Primary vesical neck Neurogenic Acquired behavior

82
Detrusor contraction Sphincter contraction Low, interrupted flow Obstruction by sphincter

83
Impaired Detrusor Contractility Low flow Weak or poorly sustained detrusor contraction Pressure flow criteria: –Qmax < 12 ml/s –Pdet@Qmax < 20 cm H2O Groutz et al, Neurourol Urodyn 19:213,2000

84
amb pdetmax = 10 cm H 2 0) Qmax = 8 ml/S
 Qmax = 8 ml/S")
85
Impaired Detrusor Contractility: Etiology Neurogenic –Thoracic, lumbar & sacral lesions –Diabetes mellitus Myogenic –Primary / idiopathc –Urethral obstruction –Bladder overdistension Urethral obstruction Post-surgical –Ischemia Groutz et al, Neurourol Urodyn 19:213,2000

86
Impaired Detrusor Contractility: Treatment Observation Double voiding Timed voiding Intermittent catheterization ? Medications –Cholinergic agonists –Alpha adrenergic antagonists

87
Conclusion Urethral obstuction not uncommon Prevalence: 2 - 29% of pts with LUTS Symptoms – non-specific –irritative 29% –obstructive 8% –both 63% Diagnosis based on p/Q studies Rx based on underlying cause usually effective for both voiding and OAB sx

Similar presentations


















 in women Ingrid Nygaard, MD, MS Professor University of Utah.>")











