Download presentation
Presentation is loading. Please wait.

1
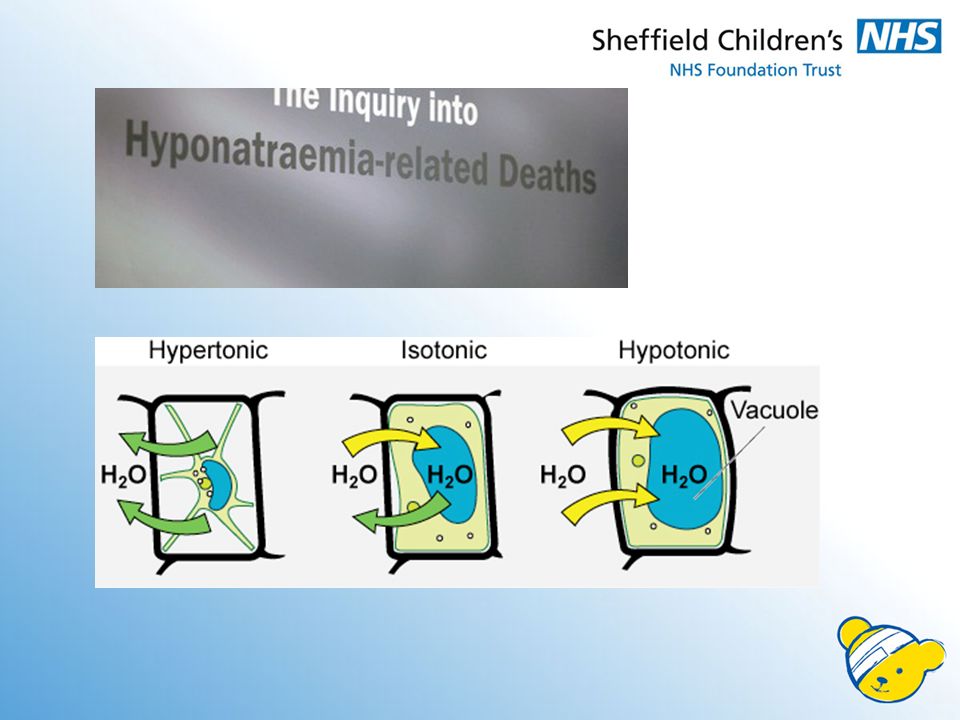
Isotonic fluids – are they better than hypotonic fluids for children? Journal Club Thursday 16 th April 2015 Charlotte Elder

2
The maintenance need for water in parenteral fluid therapy Holliday and Segar Pediatrics 1957

4
0.9% 0.45% 0.18% Hypernatraemia Hyperchloraemic acidosis Fluid overload Hyponatraemia Dehydration

6
The Clinical Question PopulationIn children requiring intravenous fluid InterventionIsotonic fluid (Na140) ComparisonHypotonic fluid (Na77) OutcomeReduce hyponatraemia DesignRandomised, double-bind, placebo controlled trial
 ComparisonHypotonic fluid (Na77) OutcomeReduce hyponatraemia DesignRandomised, double-bind, placebo controlled trial")
8
50% - 150% maintenance Recruited from ED and pre-ops

9
Na >150 mmol/L Na <130 mmol/L IVI < 6 hours LOT OF exclusions – basically any condidtion in which “standard fluid” may not be given DI, neuro surg, meningitis,

10
1:1 NA140:Na77 Stratified by baseline Na >135, 135-145, >145 All HCP Fluid bags A-H Identical looking

11
Normal saline: 154 mEq/L sodium and 154 mEq/L chloride.

12
Methods Serum Na within 4 hours Post-op – serum Na end of procedure Rate determined by clinicians Study fluid for 72 hrs or <50% maintenance Study fluid stopped if: –Na <130 –Na >150 –With Δ baseline 3+ mmol/L –Clincian decided not in pt’s best interest –Intention to treat data

13
Methods Serum electrolytes –6, 24, 48, 72 –Na, K, Cl, HCO 3, U, Cr, Gl Blood gas analyser OR Vitros lab assay Urine electrolytes at ~24 hours Clinical team monitored fluid status: –Standardised hydration assessment – if indicated and when fluid stopped SAEs recorded e.g. ITU admissions

14
Outcome measures Primary –Occurrance of hyponatraemia within 72 hours Na <135 mmol/L with 3 mmol/L Secondary –Severe hyponatraemia <130 mmol/L –Hypernatraemia >145 mmolL –Severe hypernatraemia >150 mmolL –Hyperchloraemia >110 mmol/L –Hypermagnesaemia >1.2 mmol/L –Hypercarbia >30 mmol/L –Mean serum Na and wt at 6, 24, 48, 72 hours –Others: fits, CO, coma, recannulation, hydration changes

15
Stats Sample size: 320 per arm –Reduction of hyponatraemia from 10% Na77 to 4% Na140 –Power: 80% Intention to treat analysis OR – measure of association between an exposure and an outcome –Odds of hyponatraemia occurring with Na77 –>1 is association Sensitivity and subgroup analyses –Age, total fluid, ITU/surgery, contaminated samples,

16
Study flow chart

21
http://www.casp-uk.net/

25
Hyponatraemia 4% vs 11% Significant difference 0.16-0.61 p=0.001

27
Limitations Blood gas vs lab assay Not a trial of 0.9% fluid Not powered for symptomatic hyponatraemia Multiple exclusions

28
Summary and Conclusion Very well designed study CLINICAL BOTTOM LINE –Don’t use IV fluids unless clinically indicated –Watch for signs of hypoNa EARLY - within first 6 hrs –Consider use of isotonic fluids as routine?

Similar presentations











>")

:>")












 DKA or Hyperglycemia coma is defined when blood sugar 300- 800mg/dl Is primarily seen in I.D.DM - can be seen in NIDDM. DKA.>")

. 2 Hyperglycaemia Learning objectives >Can state what hyperglycaemia is >Is aware of the short term and.>")