Download presentation
Presentation is loading. Please wait.

1
South Dakota Perinatal Association (SDPA) 40th Annual Conference September 10-11, 2015
 40th Annual Conference September 10-11, 2015")
2
Gastroschisis Case Review Michael McNamara, DO Sanford Maternal Fetal Medicine

3
Case Presentation 16 year old G1,P0 Presented at 14+4 weeks for care History of tobacco use, +THC on intake Ultrasound - gastroschisis

4
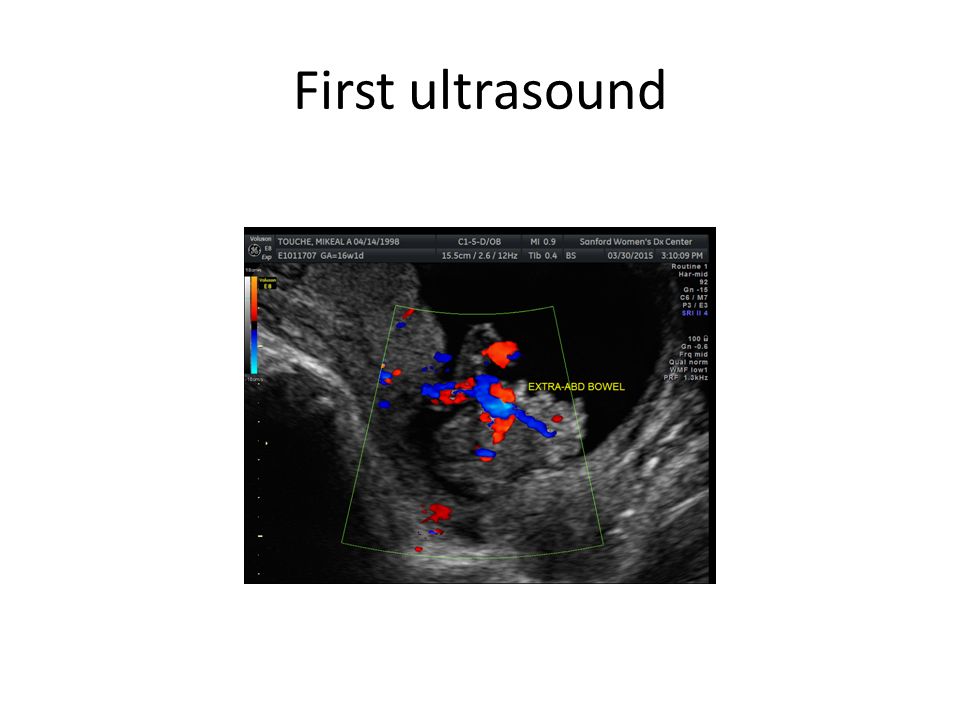
First ultrasound

7
Gastroschisis Greek, “belly cleft” Incomplete closure of lateral folds Occurs 6 th week of gestation

8
Gastroschisis Quad screen – Elevated MSAFP – 10% of highly elevated MSAFP due to gastroschisis – Not seen if has 1 st trimester screen Ultrasound – Free floating loops of small bowel – Physiological herniation of bowel until week 10

9
Gastroschisis Incidence – 1/2500 – 1/1100 with age < 20 years old Risk factors – Age; four fold increase < 20 years old – Cigarette use; 2.1 fold increase risk – Medications – acetaminophen, pseudoephedrine – Drugs – Cocaine, marijuana, methamphetamines

10
Gastroschisis Diagnosis Ultrasound Defect usually right of cord insertion Cord inserts separately No peritoneal membrane coverage Multiple loops of free floating small bowel

11
Gastroschisis Complications antenatal Fetal distress Intrauterine growth restriction (IUGR) 30-70% Associated anomalies 10-20% Usually of the gastrointestinal tract
 30-70% Associated anomalies 10-20% Usually of the gastrointestinal tract")
12
Gastroschisis Survival Greater than 90% Cause of death – Bowel ischemia – Necrotizing enterocolitis (NEC) – Sepsis – Liver failure
 – Sepsis – Liver failure")
13
Gastroschisis Clinical Course Consults – Pediatric Surgery – Neonatology – NICU tour – Pediatric Cardiology – suspected ASD

14
Gastroschisis Clinical Course Pediatric Cardiology Suspected ASD, suspected SVC emptying into the coronary sinus

15
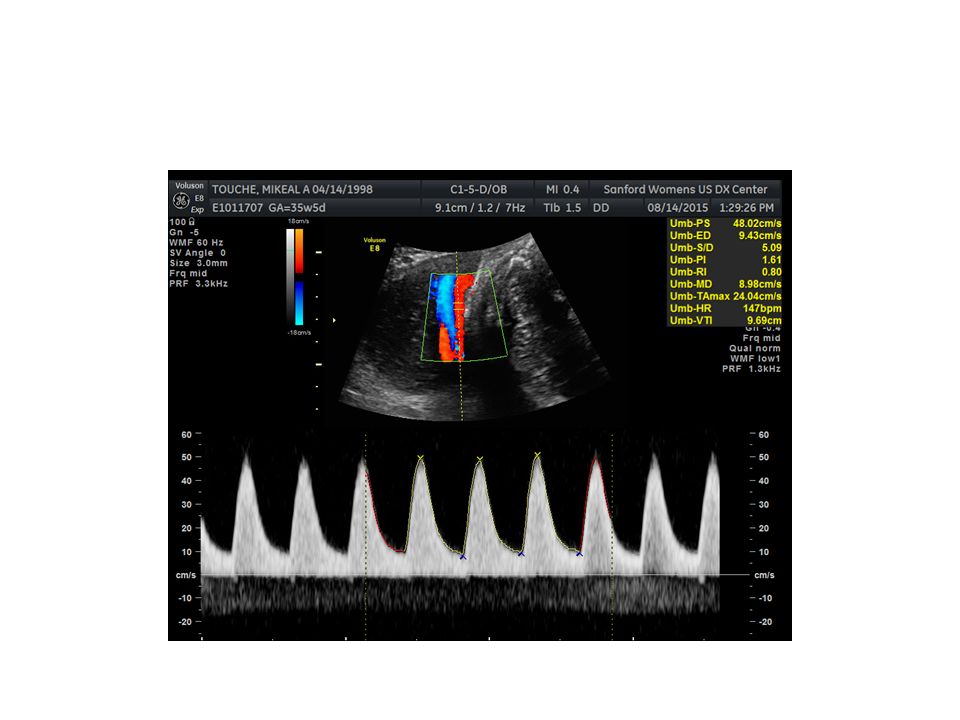
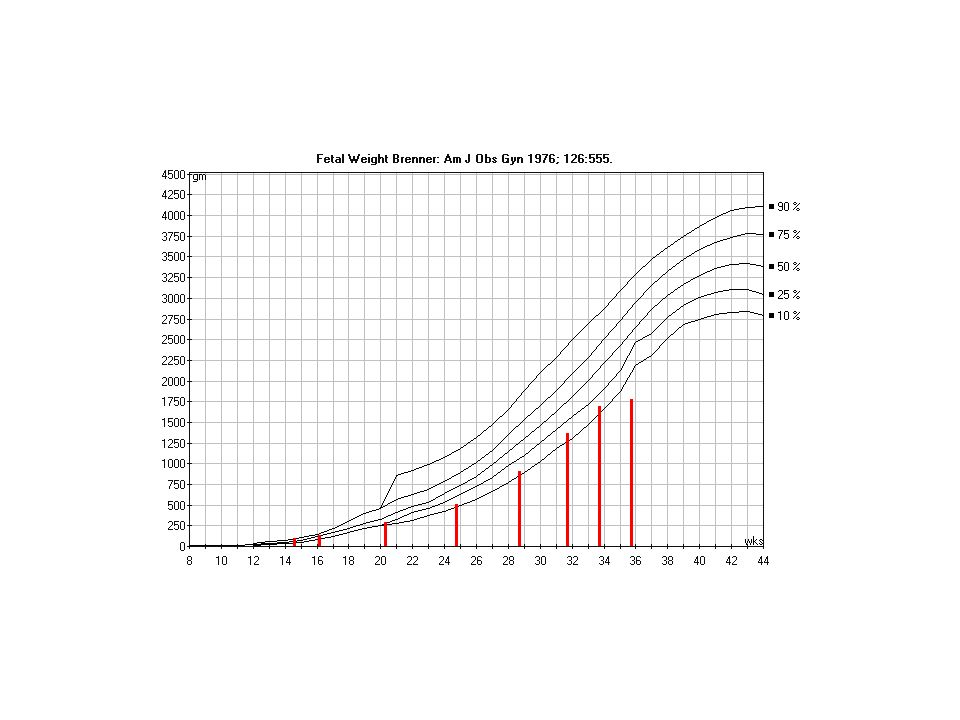
Gastroschisis Clinical Course Twice weekly antenatal testing (NST/BPP) Growth ultrasound every two weeks 35+5 weeks – Suspected IUGR with EFW < 10%, 1771 grams (previous 18%) – FL and AC < 3% – Elevated umbilical artery doppler, SD of 5.1 (previous 3.88)
 Growth ultrasound every two weeks 35+5 weeks – Suspected IUGR with EFW < 10%, 1771 grams (previous 18%) – FL and AC < 3% – Elevated umbilical artery doppler, SD of 5.1 (previous 3.88)")
16
Gastroschisis 35+5

20
Gastroschisis Delivery decision 36+ weeks IUGR, elevated SD ratio umbilical artery Suspected cardiac abnormality Discussion with Pediatric Surgery, Neonatology, Pediatric Cardiology Controlled delivery, middle of day / week Primary cesarean

21
Gastroschisis Delivery Timing – 36 weeks vs 39-40 weeks – No difference in outcomes Route of delivery – Vaginal vs cesarean – No difference in outcomes – 39 % attempting vaginal have cesarean for fetal distress

22
Gastroschisis Cesarean delivery at 36+2 weeks Neonatal weight 2260 grams 4 lbs, 15 oz Stabilized and taken to Main OR for evaluation and repair Recurrence risk 2.4%

Similar presentations


>")







 Guidelines ( )>")










