Download presentation
Presentation is loading. Please wait.

4
Infectious arthritis Bacterial Viral Other Postinfectious (reactive) arthritis Rheumatic fever Reactive arthritis Enteric infection Other seronegative spondyloarthritides Ankylosing spondylitis Psoriatic arthritis Inflammatory bowel disease Rheumatoid arthritis Inflammatory OA Crystal-induced arthritis Systemic rheumatic illnesses: SLE, vasculitis, SSc, PM/DM Other systemic illnesses: sarcoidosis, malignancy, subacute endocarditis Quinn et al. How do you diagnose rheumatoid arthritis early. Best Pract Res Clin Rheumatol 2001;15a:49-66

5
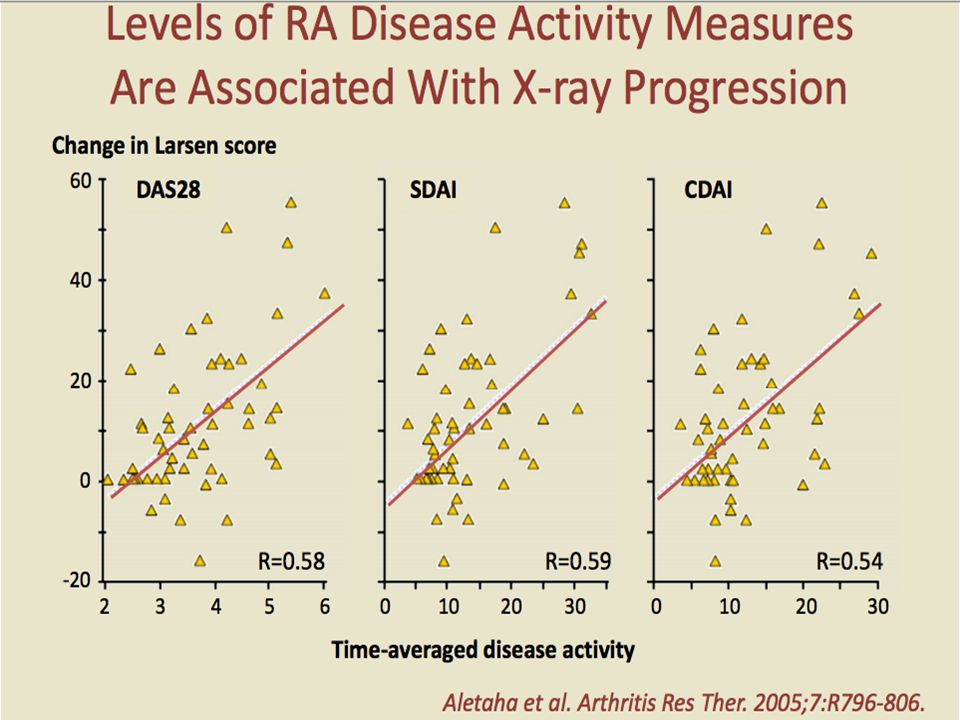
In Rheumatoid arthritis and Psoriatic arthritis: Radiographic damage within weeks of onset Window of opportunity with early DMARD for possible “cure” Both radiographic damage and disease activity are independent predictors disability Polyarthritis may be 1 st indicatior of systemic illness (HIV, cancer, SLE)
")
7
2010 ACR/EULAR Classification Criteria for RA JOINT DISTRIBUTION (0-5) 1 large joint 0 2-10 large joints1 1-3 small joints (large joints not counted)2 4-10 small joints (large joints not counted)3 >10 joints (at least one small joint) 5 SEROLOGY (0-3) Negative RF AND negative ACPA0 Low positive RF OR low positive ACPA2 High positive RF OR high positive ACPA3 SYMPTOM DURATION (0-1) <6 weeks0 ≥6 weeks1 ACUTE PHASE REACTANTS (0-1) Normal CRP AND normal ESR0 Abnormal CRP OR abnormal ESR1 ≥6 = definite RA What if the score is <6? Patient might fulfill the criteria… Prospectively over time (cumulatively) Retrospectively if data on all four domains have been adequately recorded in the past
 Retrospectively if data on all four domains have been adequately recorded in the past.")
8
30-40% of patients presenting with synovitis will remain unclassified As many as half will go into remission, and be off of medications in one year About 1/3 will go onto to develop persistant synovitis, rheumatoid arthritis Studies indicate that earlyDMARD use if started w/in critical window (<3months)may prevent progression to chronic arthritis
may prevent progression to chronic arthritis")
11
Hydroxychloroquine Sulfasalazine Methotrexate Leflunomide Azathioprine Gold Minocycline TNF inhibitors Combination of above Based on multiple studies ≈ 30% of patients will achieve DAS28 of ≤ 3.2 on MTX monotherapy (1-3) 1.BeSt. 2 year data. Ann Int Med 2007; 146:406-15 2.Swefot. Lancet 2009; 374:459-66 3.TEAR. Arthritis Rheum 2009; 60:S707

12
Patients with disease duration < 2years (mean duration 4 months) Compared SSZ monotherapy with combination therapy of: Oral prednisone (60mg 7.5mg by 6 weeks d/cd by week 28 MTX 15mg po (stopped at week 40) Sulfasalazine Significant clinical improvement in combo group, but only while steroid on board Less radiographic damage at week 56 with combination therapy 5 year follow up showed sustained suppression of the rate of radiographic progression, independent of subsequent treatment.
 Compared SSZ monotherapy with combination therapy of: Oral prednisone (60mg 7.5mg by 6 weeks d/cd by week 28 MTX 15mg po (stopped at week 40) Sulfasalazine Significant clinical improvement in combo group, but only while steroid on board Less radiographic damage at week 56 with combination therapy 5 year follow up showed sustained suppression of the rate of radiographic progression, independent of subsequent treatment.")
13
SulfasalazinePlus Methotrexate and HydroxychloroquineDose escalationOral prednisoneMethotrexate and CyclosporineOther DMARD 110 pts randomized, active RA < 5 years duration for 18 months. Two groups: usual therapy versus intensive therapy *Intra-articular steroid injections used but biologics were not. Grigor, Porter, Stirling, Capell. Lancet 2004:364:263-9

14
Intensive group n = 55 Routine group N = 55 Odds ration (95%) (p<0.001) EULAR good response 80%44%3.6 (1.5-8.7) EULAR remission65%16%9.6 (3.8-24.3) ACR 2089%64%4.0 (1.5-10.5) ACR 5082%45%4.9 (2.1 – 11.4) ACR 7070%18%9.5 (3.9 – 23.0) Grigor et al. Lancet 2004: 364:263-69

15
MonoDoubleTripleI vs III vs IIIII vs III (P Values) ACR 5049.1%73.5%87.9%<0.001 Remission31.5%44.6%60.3%0.007 No Xray progression 24.5%64.2%68.9%0.001 0.210 Calguneri et al. Clin Exp Rheumatology 1999:17:699-704 *ERA trial: 63% no radiographic progression at 2 years

16
Should we use combinations initially in all new patients or use a rapid step-up to combinations only in those that need it? COBRA, FINRa-Co, Calguneri, PREMIER, all favor combinations initially. TICORA shows that rapid step-up can be very effective, as does 2 year BeSt data and TEAR TEAR shows no penalty for waiting (step up at 4-6 month mark)
.")
17
Studies out of the UK have shown a dramatic reduction in delays to rheumatologic evaluation Studies in the 1980’s, found the median delay from symptom onset to referral was over 20 months, in one large teaching hospital in Glasgow, UK Subsequent studies in the 90’s indicated that most of the delay stemmed from time to seek initial medial care (avg 4months) and time to seeing rheumatologist another month In Austria, nation-wide public campaign advising people with signs of inflammatory arthritis to contact their GP
 and time to seeing rheumatologist another month In Austria, nation-wide public campaign advising people with signs of inflammatory arthritis to contact their GP")
18
Several studies suggest that the very early phase of disease may be pathologically distinct from established RA, which may represent a therapeutic window in which “cure” may be possible. Rapid control of inflammation even in established RA with DMARD therapy has been shown to slow the progression of joint damage and disability. Patients should be regularly followed to ensure “tight control” aiming for low disease activity or remission.

Similar presentations


 Immunomodulatory and immunosuppresive Xenobiotic – Gold salts – Azathioprine – Methotrexate Biological.>")









¹ Five or more of the following criteria must be fulfilled for at least.>")








