Download presentation
Presentation is loading. Please wait.

1
Monitoring the National Cancer Standards for dummies…… ……….by dummies Louise Carrington. Programme Co-ordinator CSCG Andrew Graham. HSW

2
Today Quick summary of the target Run through the software from log-in to reporting –Changes and definitions –Key messages and top tips Q&A session lastly one-to-one tuition on specifics if anyone is interested

3
Standards? What standards? Published August 2005 WHC (051) 2005 expectation of full compliance by March 2009…. ……Which is now
 2005 expectation of full compliance by March 2009…. ……Which is now.")
4
Yeah, but……? Which standards are the critical ones? What does “comply with” mean? “by March 2009”, is that: the beginning of March? the end of March? from the first of April? Will we get more money if we’re seen to be doing badly or doing well?

5
Which standards are the critical ones? All Cancer Standards are created equal: none are more equal than others. (Sorry George)
.")
6
What does “compliance” mean? Compliance = 100% at the level of each standard. Each is pass or fail Advisable to complete full data entry even if you think you’re only a little way there: a.You might comply b.Assessment of partial compliance may be used to trigger further phases in the monitoring process

7
What does “by March 2009” mean? The end of March 2009 But … must be able to demonstrate that you are compliant by the end of March 2009

8
Example A e.g. people, services and things –do you have a policy in place? –do you have 2 breast surgeons? »Can be implemented on the 31 st March 2009 and be compliant.

9
Example B e.g. activity and whole year data –Have each of your breast surgeons seen 50 patients in the last year? –Has your Head and Neck MDT managed at least 80 patients during the year? »Will need activity data from the entire period April 1 st 2008 to March 31 st 2009 to demonstrate compliance

10
Example C Analysis of how things are working –Audits (of policies, referral pathways) –Have your core MDT members attended more than 50% of the MDTMs? »Will need to have been in place long enough to assess/audit and report on

11
Will we get more money if we are seen to be doing badly or doing well? Accurate data ……

12
Getting started

15
What sort of MDT are we? Cancer site and level A: Breast, colorectal, gynaecological, haematological etc B: Local/Network/SupraNetwork level Full list of expected MDTs is published on the CSCG webpage, with –their specialty –level –MDT lead clinician

16
What does the level mean? Specialisation, rare, complex and patient flow Defined by NICE/IOG Designated and agreed by the Network Central Team

17
Local MDTs May refer patients on to a Network or supranetwork MDT act as purely diagnostic services manage local patients only manage patients from further afield be many or few within a network Be more than one in a single health organisation Local MDT 1° Care Emergencies Screening

18
Network MDTs Will receive patients referred on from local MDTs Be more specialised than local MDTs: treatments, cancer types be only one per network (for most cancer types) May also act as a local MDT for their local patients Network MDT 1° Care Emergencies Screening Local MDT 1° Care Emergencies Screening
 May also act as a local MDT for their local patients Network MDT 1° Care Emergencies Screening Local MDT 1° Care Emergencies Screening")
19
More specialised than Network MDTs Cover more than 1 Network May receive referrals from network and local MDTs be only one in Wales for their cancer type (or cancer sub-type) act as local MDT for their local population act as a Network MDT for their Network SupraNetwork MDTs Network MDT 1° Care Emergencies Local MDT 1° Care Emergencies Screening Supranetwork MDT Network MDT 1° Care Emergencies Local MDT 1° Care Emergencies Screening
 act as local MDT for their local population act as a Network MDT for their Network SupraNetwork MDTs Network MDT 1° Care Emergencies Local MDT 1° Care Emergencies Screening Supranetwork MDT Network MDT 1° Care Emergencies Local MDT 1° Care Emergencies Screening")
20
–Doing Network level work (e.g complex surgeries) –Working in more than one Trust/Health organisation/network –Having MDT members from more than one Trust/Health organisation/network –Holding joint MDTMs with other MDTs If in doubt ask your central Network Team X
 –Working in more than one Trust/Health organisation/network –Having MDT members from more than one Trust/Health organisation/network –Holding joint MDTMs with other MDTs If in doubt ask your central Network Team X")
21
But…… If you are carrying out the functions of a network MDT (i.e. the complex surgeries, treating the rare cancers etc) make sure this information is recorded in the database.
 make sure this information is recorded in the database..")
22
The following Cancer sites only have MDTs/SPCTs operating at one level (“local” level) breast, lung, head and neck, thyroid, specialist palliative care, MDTs in these cancer sites: do not refer on to more specialist MDTs. may have patients referred to them from the entire Network (& other areas) in order to fulfil activity criteria The remainder have tiers of MDT levels
 in order to fulfil activity criteria The remainder have tiers of MDT levels.")
23
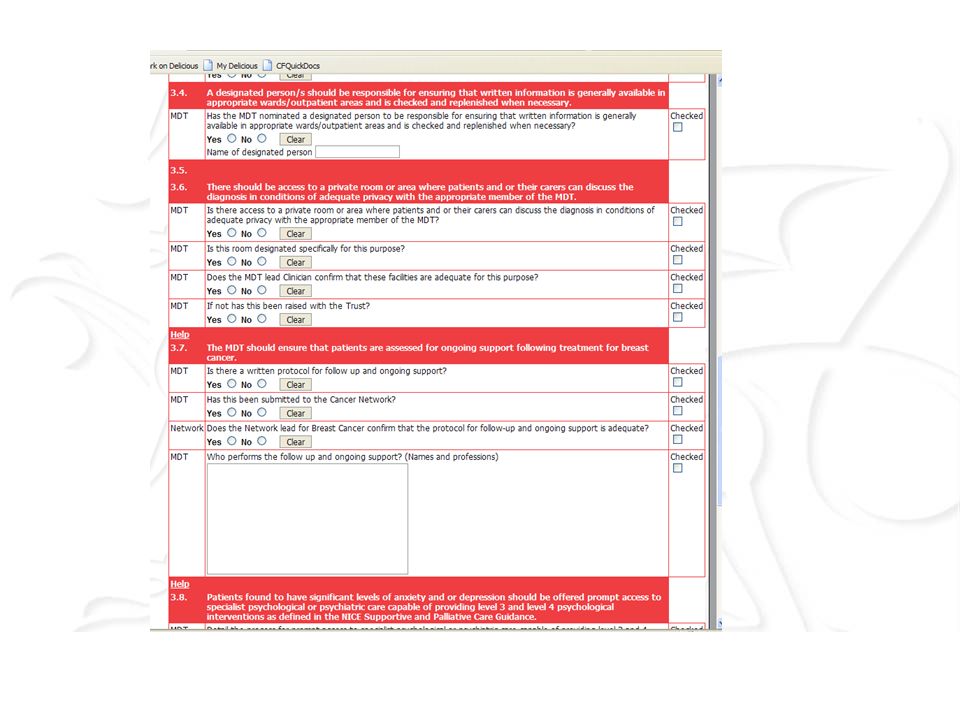
Top tips for data entry Classic exam technique tips: –Read the questions –Enter the data in enough detail CSCG central team External validation team Don’t assume knowledge but don’t overwhelm –Check your answers follow logically? Identical in different parts of the database –Validate the data (71387 lung cancers) Press “submit” frequently to prevent data loss
 Press submit frequently to prevent data loss.")
24
If the answer is 0, put 0, don’t leave blank. Whole year data or sample data This year or minimum three year cycle Answer all parts of the question don’t just give the numbers Activity data, audits and other numbers asked for All, most, some, zero, fifty, 50-60, roughly half, c.99%, n/a, not known, we don’t have the resources to find this…..

25
Am I a core/non-core/associate member of the MDT? different scoring rules apply to core and non- core members of the MDT. MDT assigns those who are core and those who aren’t Must have the required number of core individuals from each profession in the list Core individuals must attend more than 50% of MDTMs Looking at the number of MDTMs running without a specialty present or postponed/cancelled because a specialty wasn’t present.

26
Additional MDT professions Additional professions that are not in the standards list Essential/occasional Won’t be scored against the standards Markers of quality (research nurses etc) Best practice
 Best practice")
27
Changes Summary of all substantive changes on website –The MDT membership –New NHS Wales structure –Help buttons –MDT summary/pathway pages –Audit timings –All Wales dataset completion –Surgical standards –SPC standards –Skin standards –Specialist pathologists and radiologists –Sign-off mechanism

28
Specialist pathologists and radiologists Not those listed as MDT members in section 4. second opinion, May be extremely rare For UK and International-level specialists, the person/s to whom they refer for a second opinion, may be no more specialist than themselves, and be called upon very infrequently.

29
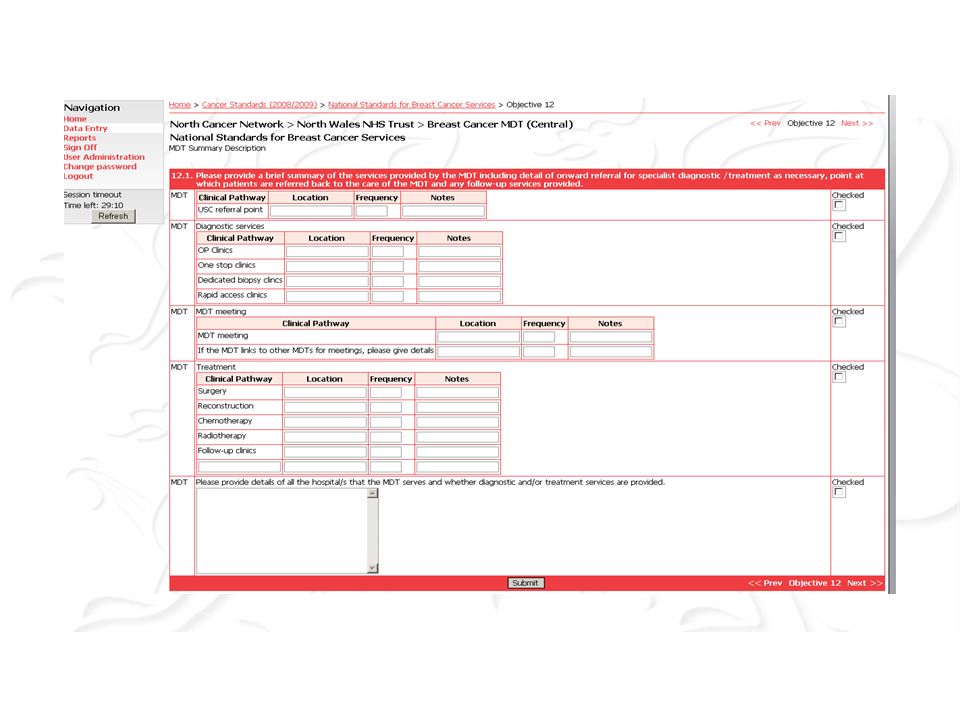
MDT summary page

31
Sign off

32
Reporting

33
Data, data, everywhere Agreed in outline with the Minister, tight deadline for reporting. Current plan: no central validation prior to reporting to the Assembly accepting all data at face value Won’t be using any occult knowledge to enhance/interpret your answers Presenting pass-fail situation to the assembly Assembly final decision

34
HSW (technical) RFW-Web@HSW.Wales.NHS.UK RFW-Web@HSW.Wales.NHS.UK Network advisors CSCG website http://howis.wales.nhs.uk/sites3/page.cfm?orgid=322&pid=14275 http://howis.wales.nhs.uk/sites3/page.cfm?orgid=322&pid=14275 Workshops CSCG Louise.Carrington@cscg.wales.nhs.uk, 02920196163 Louise.Carrington@cscg.wales.nhs.uk Query log Help files FAQs Changes document Top tips etc Clinical advisory structure Assembly Networks
 Network advisors CSCG website orgid=322&pid= orgid=322&pid=14275 Workshops CSCG Query log Help files FAQs Changes document Top tips etc Clinical advisory structure Assembly Networks")
35
Summary Use the help resources Read the questions Enter as much detail as asked for in the correct format Assume nothing Check the data Obtain clinical and managerial sign-off If in doubt ask And finally…….

36
Feedback from users

Similar presentations
 process.>")


>")

>")

>")











