Download presentation
Presentation is loading. Please wait.

1
Defaulting in OTP: a programme and research perspective Based on Lusaka CTC November 4 th, 2009 Abel Irena (M.D, MSc, DTH&M)
")
2
Presentation layout Objective of the presentation Background Implication on programme Implication on research Defaulter tracing

3
Objective To share problem of defaulting in Lusaka CTC To highlight the most common reasons for defaulting To discuss the implication of high defaulting in OTP – A programmatic perspective & – A research perspective

4
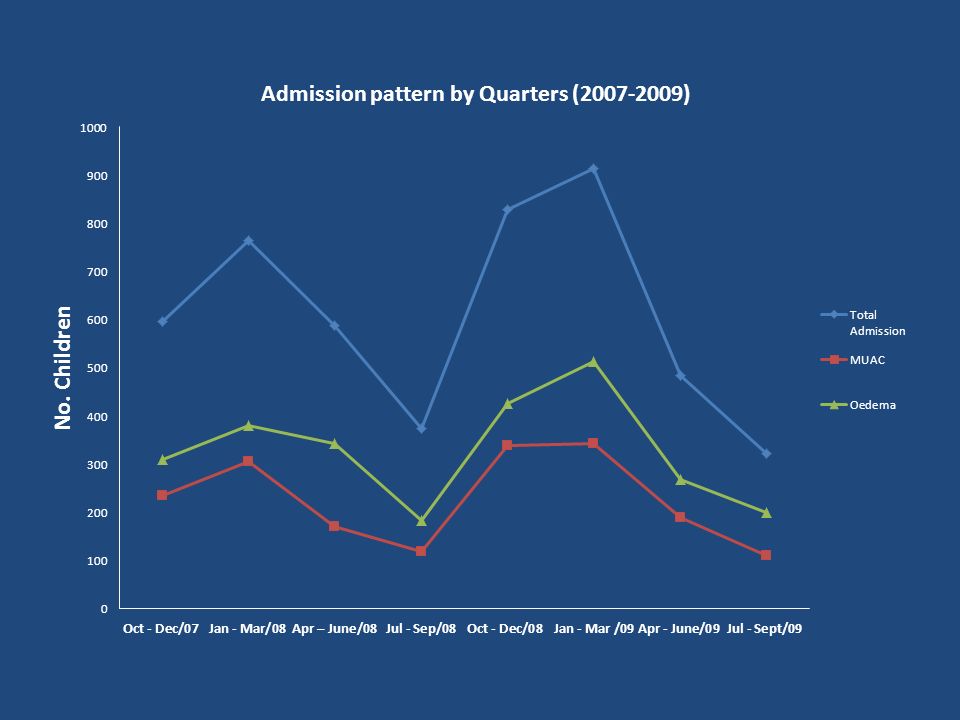
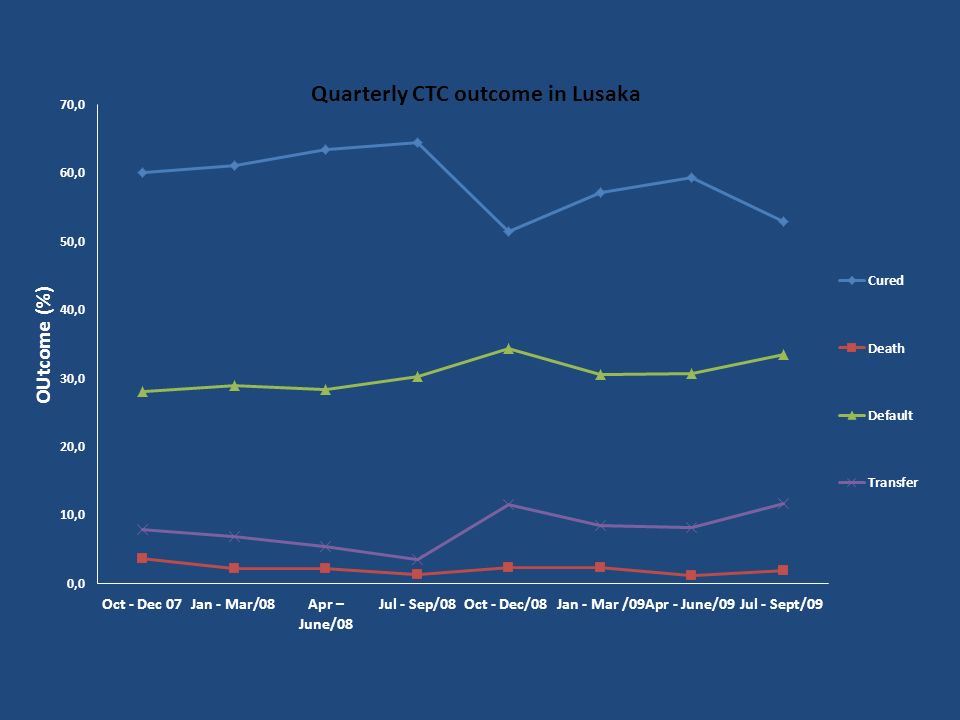
Oct - Dec 2007 Jan - Mar 2008 Apr – June 2008 Jul - Sep 2008 Oct - Dec 2008 Jan - Mar 2009 Apr - June 2009 Jul - Sept 2009 Total #%#%#%#%#%#%#%#% TOTAL ADMISSIONS 597 765 588 374 829 914 485 323 4875 Cured 276(60.1)548(61.4)433(63.0)384(64.4)385(51.6)605(57.2)429(59.3)217(52.9) 3277 Death 17(3.7)19(2.1)15(2.0)8(1.3)17(2.3)24(2.3)8(1.1)8(2.0) 116 Default 129(28.1)259(29.0)194(28.0)180(30.2)257(34.5)323(30.6)222(30.7)137(33.4) 1701 Transfer 367.8%616.8%375.0%213.5%8611.5%898.4%598.2%4811.7% 437 Non-cured 10.2%91.0%4 30.5%30.4%161.5%50.7%00.0% 41 TOTAL EXITS 459 892 683 596 746 1,057 723 410 5566 Return Default 4 22 24 29 25 27 36 194
548(61.4)433(63.0)384(64.4)385(51.6)605(57.2)429(59.3)217(52.9) 3277 Death 17(3.7)19(2.1)15(2.0)8(1.3)17(2.3)24(2.3)8(1.1)8(2.0) 116 Default 129(28.1)259(29.0)194(28.0)180(30.2)257(34.5)323(30.6)222(30.7)137(33.4) 1701 Transfer 367.8%616.8%375.0%213.5%8611.5%898.4%598.2%4811.7% 437 Non-cured 10.2%91.0%4 30.5%30.4%161.5%50.7%00.0% 41 TOTAL EXITS , Return Default")
7
Technical support & investigation on defaulting 20052006200720082009 JuneJune/JulyJulyApril + October Feb Based on different studies: Qualitative Quantitative

8
June- July 2006 Method – Qualitative Reason for defaulting – Intra-city migration – Self discharge Minimum 8 weeks – Illness – Labour responsibilities – Distance 12 health centres – Lack of understanding of RUTF, OTP Defaulter tracing Done by volunteers – Limited service availability – Wrong address No ranking

9
July 2007 Method – Qualitative Reason for defaulting – Economic reason – Misconceptions regarding the CTC – Unforeseen circumstances Illness Motivating volunteers – Not paid after being promised – Heavy workload? Relieve the role of active case finding & sensitization – Lack of recognition for their work? Refresher training – Rejection of children? No ranking

10
April 2008 DefaulterTraceddeadSAM 572876 (49.1%)(25%)(21.5%) Based on 8 clinic catchments area survey Reason for defaulting Busy Stigma Cause of child’s condition Distance (did not exceed 45 minutes) Traditional belief RUTF (shortage & belief it causes disease) Sickness Long duration of stay in programme
(25%)(21.5%) Based on 8 clinic catchments area survey Reason for defaulting Busy Stigma Cause of child’s condition Distance (did not exceed 45 minutes) Traditional belief RUTF (shortage & belief it causes disease) Sickness Long duration of stay in programme")
11
Barrier to service access Lack of knowledge about CTC57 Transfer failure4 Sick carer2 Busy carer1 Mother dead1

12
Feb 2009 criteriaMeanSDminMax Age (mo)186.77120 MUAC (cm)11.31.4815 Oedema61.0% had oedema on admission 52% had oedema upon defaulting HIV status53(60.0%) status not known at time of default 12 (34.3%) HIV positive? LOSMean (SD)=34 (17.7) days Out of 88 defaulters 54 (61%) could not be located 12 (13.6%) moved out 6 (5.7%) died 17 (19.2%) return defaulter/okay Mortality =17.1% Small sample size
=34 (17.7) days Out of 88 defaulters 54 (61%) could not be located 12 (13.6%) moved out 6 (5.7%) died 17 (19.2%) return defaulter/okay Mortality =17.1% Small sample size.")
13
Role of volunteers Over 400 volunteers Assist in anthropometry measurement Assist in active case finding – when possible (GMP) Run OTP in the absence of nurse/nutritionist – Less frequently at the moment Absent and defaulter tracing – Has not been consistent
 Run OTP in the absence of nurse/nutritionist – Less frequently at the moment Absent and defaulter tracing – Has not been consistent")
14
You need me to assist @ the clinic!

15
Pay me to leave my job!!!!!!!!!

16
Give me means & I will do it!!!!!!!!!

17
Bicycle will probably do!

18
Did we do anything? Payment per defaulter traced @ the start – Payment interrupted in late 2007 Secondment of a focal community mobilizer from LDHMT – Provide with mentoring /training Refresher training for volunteers Case finding through use of child health week Payment made during defaulter tracing – Only to few and others still expecting The seconded person too busy – 25 health centres to coordinate – Large number of absentees and defaulters to follow – Low motivation of volunteers

19
Implications on programme Won’t meet internationally agreed standards (SPHERE, CTC) Criticism on success of CTC – ? Majority die The million Kwacha Q is@ – Is this defaulter trend normal for urban area? – Is this normal for programme run by Govn’t? – Should we accept and live with it?

20
Implications on research Lost to follow-up (LTFU) – Selection bias cohort studies RCT How to manage LTFU – Outcome? – Do they have similar exposure status? Implications on publication on a peer reviewed journal

21
Scenarios for mortality among defaulters Under five mortality in Zambia 119/1000 202 children would have died? UTH mortality rate: 30-40% 152 children would have died CriteriaTotal #Hypothesis Defaulter1701=1701*119/1000202 Transfer437=437*35/100152 Death116=116+152+202471 Total Exit5566=417/5566*100 8.5%

22
UTH

Similar presentations