Download presentation
Presentation is loading. Please wait.

1
Dr. Moneer K. Faraj Consultant Neurosurgeon College of Medicine, Baghdad Uni.

2
Lumbar spinal canal stenosis :Reduction in the diameter of the spinal canal which results from either congenital stenosis & / or degenerative changes.

3
Degenerative changes may result in: Lumbar disc protrusion Facet joint osteoarthritis Ligamentum flavum hypertrophy End plate changes ( modic changes)
")
5
Neurogenic Claudication ◦ Dermatomal: pain/sensory changes/weakness of buttock, hip, thigh, or leg initiated by standing or walking ◦ slow relief with postural changes (sitting >30 min), NOT simply exertion cessation ◦ elicited with lumbar extension, but may not have any other neurological findings, no signs of vascular compromise (e.g. ulcers, poor capillary refill, etc.)
.")
6
Facet Joint Syndrome comprises clinical symptoms related to the facet joints such as dysfunction and osteoarthritis. The cardinal symptoms of facet joint pain are: predominant low-back pain osteoarthritis pain type (improvement during motion) However, in late stages of OA this alleviation will disappear pain aggravation in extension and rotation (standing, walking downhill) The pain is often located in the buttocks and groin and infrequently radiates into the posterior thigh. However, it is non-radicular in origin. Patients often feel stiff in the morning sometimes of such intensity that they have difficulty to get out of bed.
 However, in late stages of OA this alleviation will disappear pain aggravation in extension and rotation (standing, walking downhill) The pain is often located in the buttocks and groin and infrequently radiates into the posterior thigh. However, it is non-radicular in origin. Patients often feel stiff in the morning sometimes of such intensity that they have difficulty to get out of bed..")
7
Instability Syndrome The cardinal symptom of a segmental instability is: mechanical low-back pain Instability pain worsens during motion and improves during rest Vibration (e.g. driving a car, riding in a train) may aggravate the pain. Pain is also felt when sudden movements are made. The resulting muscle spasm can be so severe that the patients experience a lumbar catch (“blockade”). Pain usually does not radiate below the buttocks. Some patients benefit from wearing a brace.
 may aggravate the pain. Pain is also felt when sudden movements are made. The resulting muscle spasm can be so severe that the patients experience a lumbar catch ( blockade ). Pain usually does not radiate below the buttocks. Some patients benefit from wearing a brace..")
8
In patients with facet syndrome, physical findings are: pain provocation on repetitive backward bending pain provocation on repetitive side rotation hyperextension in the prone position In patients with instability syndrome, physical findings are: abnormal spinal rhythm (when straightening from a forward bent position). The patient needs the support with hands on thighs when straightening out of the forward bent position by supporting the back.

9
Standard radiographs are rarely diagnostic disc space narrowing with endplate sclerosis severe facet joint osteoarthritis Flexion/Extension Films Functional views : excessive segmental motion (>4mm) or subluxation of the facet joint that is rare in asymptomatic individuals
 or subluxation of the facet joint that is rare in asymptomatic individuals")
11
Computed Tomography The current role of CT is for patients with contraindications for MRI (e.g. pacemaker). In the latter case, CT is often combined with myelography (myelo-CT) to provide conclusions on potential neural compression. in the evaluation of patients postoperatively to assess lumbar fusion status.
. In the latter case, CT is often combined with myelography (myelo-CT) to provide conclusions on potential neural compression. in the evaluation of patients postoperatively to assess lumbar fusion status..")
13
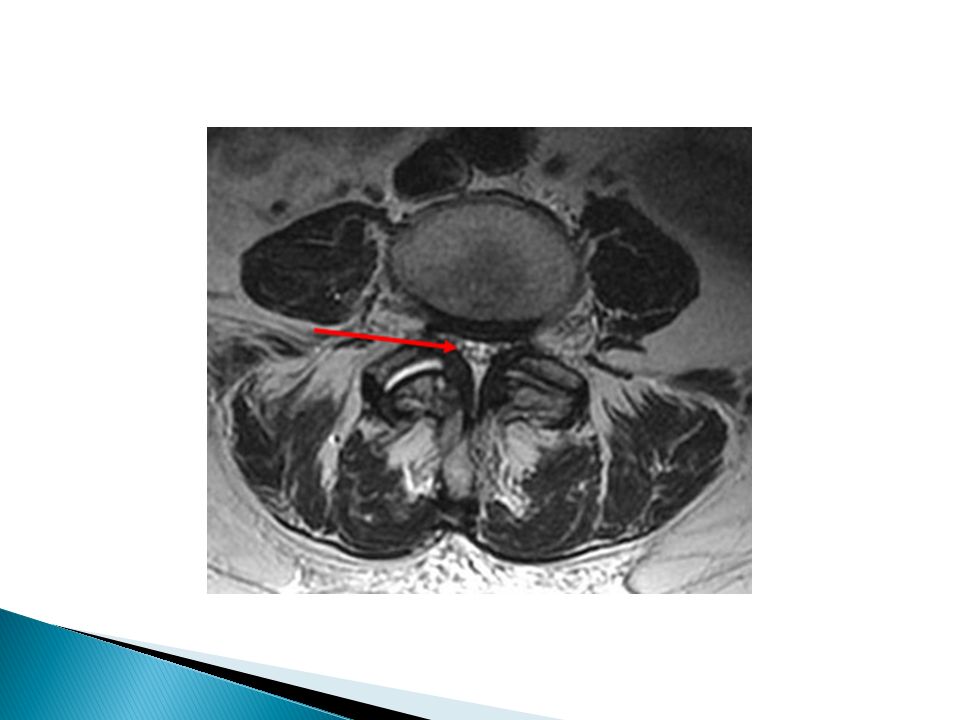
MRI It is superior to computed tomography (CT) because of its tissue contrast and multi planar capabilities.
 because of its tissue contrast and multi planar capabilities.")
17
General objectives of treatment pain relief improvement of health-related quality of life improvement of work capacity

18
Patient Selection for Treatment Various domains must be considered, medical factors psychological factors sociological factors work-related factors

19
Favorable indications for non-operative treatment minor to moderate structural alterations short duration of persistent symptoms <6months Pain of variable intensity and location absence of risk factor ( early neurological deficit) intermittent symptoms
 intermittent symptoms")
20
The non-operative management composed of : pain management (medication) functional restoration (physical exercises) cognitive-behavioral therapy (psychological intervention)
 functional restoration (physical exercises) cognitive-behavioral therapy (psychological intervention)")
21
Favorable indications for operative treatment severe structural alterations and instability failure to relief the pain more than 6 months of medical therapy. Progressive neurological deficit Psychologically stable patient.

22
Decompression Laminectomy Non instrumented spinal fusion Instrumented spinal fusion Spinal fusion with fixation A combination of previous surgeries

28
Etiology Tear in the annulus with herniation of the nucleus outside either laterally compressing nerve root, or centrally causing cauda equina or lumbar stenosis (neurogenic claudication)
")
29
leg pain > back pain limited back movement (especially forward flexion) due to pain dermatomal sensory changes, motor weakness, reflex changes exacerbation with coughing, sneezing or straining. Patients often report that sitting is the worst position (caused by disc compression). Relief with flexing the knee or thigh nerve root tension signs ◦ straight leg raise (SLR test) or crossed SLR (pain should occur at less than 60 degrees) suggest LS, Sl root involvement ◦ femoral stretch suggest L2, L3 or L4 root involvement
. Relief with flexing the knee or thigh nerve root tension signs ◦ straight leg raise (SLR test) or crossed SLR (pain should occur at less than 60 degrees) suggest LS, Sl root involvement ◦ femoral stretch suggest L2, L3 or L4 root involvement.")
30
Central, sub articular, foramenal, extreme lateral

32
L5-S1L4-5L3-4 SlSlL5L4 Root Involved 45%45%45%<10% Incidence Sciatic pattern Femoral patternPain LateralfootLateral leg Dorsal foot to hallux Medial legSensory Gastronemius, Soleus ( plantar flexion) Extensor hallusis longus ( hallux extension) Tibialis anterior (dorsiflexion) Motor Ankle jerk Knee jerkReflexes
 Extensor hallusis longus ( hallux extension) Tibialis anterior (dorsiflexion) Motor Ankle jerk Knee jerkReflexes")
33
x -ray spine (only to rule out other lesions) CT, CT- Myelography MRl consider EMG, nerve conduction studies if diagnosis uncertain
 CT, CT- Myelography MRl consider EMG, nerve conduction studies if diagnosis uncertain")
35
conservative ◦ bed rest ◦ activity modification, patient education (reduce sitting, lifting) ◦ physiotherapy, exercise programs ◦ analgesics may help
 ◦ physiotherapy, exercise programs ◦ analgesics may help")
36
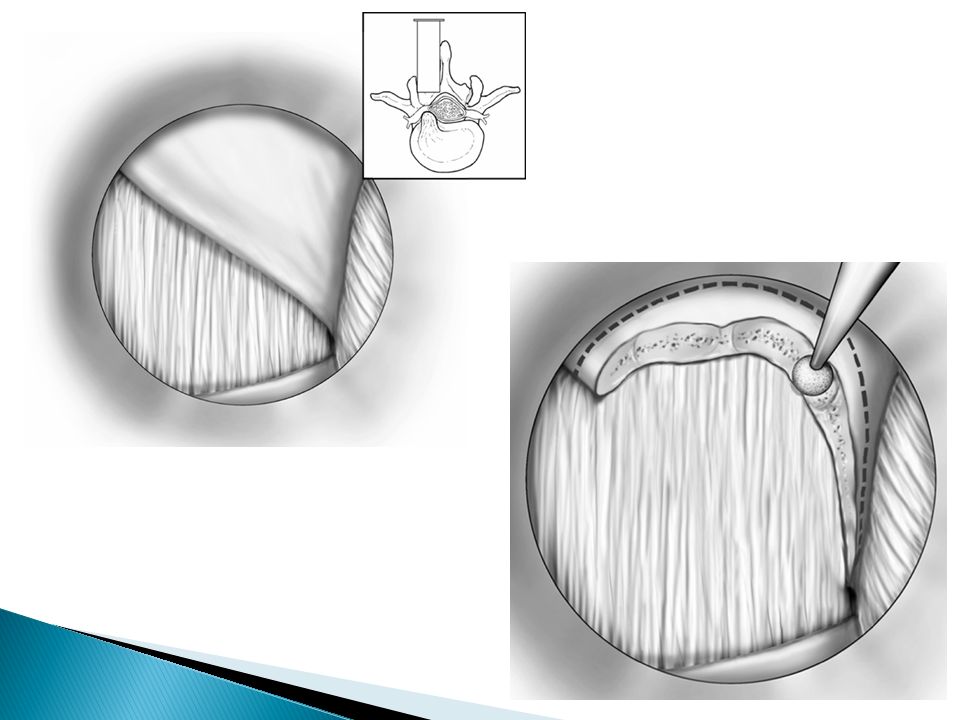
surgical indications ◦ intractable pain despite adequate conservative treatment for >3 months ◦ progressive neurological deficit Types: - open laminectomy with discectomy - micro discectomy

41
Etiology compression or irritation of lumbosacral nerve roots below conus medullaris due to decreased space in the vertebral canal below L2. Common causes include herniated disk, spinal stenosis, vertebral fracture and tumors.

42
usually acute (develops in less than 24 hours); rarely subacute or chronic motor (LMN signs) ◦ weakness/paraparesis in multiple root distribution ◦ reduced deep tendon reflexes (knee or ankle) autonomic ◦ urinary retention (or over flow incontinence) and/or fecal incontinence due to loss of anal sphincter tone sensory ◦ low back pain radiating to legs (sciatica) aggravated by Valsalva maneuver and by sitting; relieved by lying down ◦ bilateral sensory loss or pain: depends on the level of cauda equina affected ◦ saddle area (S2-S3) anesthesia (most common sensory deficit) ◦ sexual dysfunction (late finding)
; rarely subacute or chronic motor (LMN signs) ◦ weakness/paraparesis in multiple root distribution ◦ reduced deep tendon reflexes (knee or ankle) autonomic ◦ urinary retention (or over flow incontinence) and/or fecal incontinence due to loss of anal sphincter tone sensory ◦ low back pain radiating to legs (sciatica) aggravated by Valsalva maneuver and by sitting; relieved by lying down ◦ bilateral sensory loss or pain: depends on the level of cauda equina affected ◦ saddle area (S2-S3) anesthesia (most common sensory deficit) ◦ sexual dysfunction (late finding)")
43
Treatment: requires urgent investigation and decompression (<48 hrs) to preserve bowel and bladder function and/ or to prevent progression to paraplegia Prognosis: markedly improves with surgical decompression. Recovery correlates with function at the initial consult: if patient is ambulatory, likely to continue to be ambulatory; if unable to walk, unlikely to walk after surgery

Similar presentations


































 Case 3: Karen.>")


 - Lumbar>")







