Download presentation
Presentation is loading. Please wait.

1
ED Evaluation of Abdominal Pain Kathleen Jobe, MD Division of Emergency Medicine University of Washington

2
“It’s the damned belly that gives man his worst troubles” -Homer

3
Epidemiology One of the most common presenting complaints: 4-8% of adult ED visits. One of the most common presenting complaints: 4-8% of adult ED visits. Admission rates of 18-42% in adults, much higher rates in the elderly Admission rates of 18-42% in adults, much higher rates in the elderly In 42% of patients etiology is unknown. In 42% of patients etiology is unknown.

4
Diagnosis “Abdominal pain of unknown etiology” “Abdominal pain of unknown etiology”

5
“Beauty cannot disguise nor music melt, A pain undiagnosable but felt” - AM Lindbergh

6
Immediate Life Threat Abdominal aortic aneurysms Abdominal aortic aneurysms Splenic rupture Splenic rupture Ectopic pregnancy Ectopic pregnancy Myocardial infarction Myocardial infarction

7
Extra Abdominal Causes of Abdominal Pain Systemic Systemic DKA AKA Uremia Sickle cell disease SLE Vasculitis Glaucoma Hyperthyroidism Toxic Methanol Heavy metals Scorpion bites Lactrodectus bite Thoracic Acute coronary syn Pneumonia PE Thoracic disc disease

8
Extra Abdominal Causes of Abdominal Pain Genitourinary Genitourinary Testicular torsion Renal colic Infectious Infectious Strep pharyngitis Rocky Mtn. Spotted Fever Mononucleosis Abdominal Wall Pain Herpes zoster Muscle hematoma Muscle spasm

9
Disease Spectrum by Age Diagnosis Age 50 Diagnosis Age 50 Cholecystitis6%21% Cholecystitis6%21% Nonspecific40%16% Nonspecific40%16% Appendicitis32%15% Appendicitis32%15% Bowel obst2%12% Bowel obst2%12% Pancreatitis2%7% Pancreatitis2%7% Diverticular disease<0.1%6% Diverticular disease<0.1%6% Cancer<0.1%4% Cancer<0.1%4% Hernia<0.1%3% Hernia<0.1%3% Vascular<0.1%2% Vascular<0.1%2%

10
History Quality of Pain Quality of Pain Onset Onset Severity Severity Associated symptoms Associated symptoms

11
History (continued) Gyn history-Sexual activity, LMP, contraception, gravida/para status. Gyn history-Sexual activity, LMP, contraception, gravida/para status. Recurrence of symptoms Recurrence of symptoms PMH-Surgeries, Chronic illnesses, Risk factors PMH-Surgeries, Chronic illnesses, Risk factors Medications Medications

12
The importance of positioning

13
Physical Exam Location of Tenderness Location of Tenderness Original study of McBurney’s point tenderness had n=10 80% of patients with appendicitis have tenderness to palpation in the RLQ Guarding Guarding Involuntary guarding (rigidity) greatly increases the likelihood of surgical disease Voluntary guarding not predictive
 greatly increases the likelihood of surgical disease Voluntary guarding not predictive")
14
Physical Exam Vitals signs Vitals signs Temperature variable sens. and spec. for intra-abdominal infection Majority of elderly patients with acute cholecystitis and appendicitis are afebrile.

15
Physical Exam General appearance General appearance ‘You can observe a lot just by watching’ -Yogi Berra

16
Physical Exam Peritoneal Signs Peritoneal Signs Cough test is 80-95% sensitive for surgically proven peritonitis ‘Heel drop’ was 93% sensitive for appendicitis Less sensitive in the elderly

17
Physical Exam Specific PE signs Specific PE signs Murphy’s- Useful in diagnosing cholecystitis and biliary colicUseful in diagnosing cholecystitis and biliary colic Sensitivity of 97% and negative predictive value of 93% for cholecystitis.Sensitivity of 97% and negative predictive value of 93% for cholecystitis. Specificity of <50% for cholecystitisSpecificity of <50% for cholecystitis Psoas Sensitive and specific for psoas muscle abcessSensitive and specific for psoas muscle abcess Appendicitis -95% spec, 16% sens in one small studyAppendicitis -95% spec, 16% sens in one small study

19
Physical Exam Rosving’s Rosving’s Obturator Obturator Boas sign Boas sign

20
Carnett’s sign Carnett’s Carnett’s 95% accuracy in distinguishing abdominal wall pain from visceral pain

21
Pelvic Examination Valuable in all women with abdominal pain Valuable in all women with abdominal pain Fitz-Hugh-Curtis PID vs. appendicitis Appendicitis may cause CMT (30% of cases) Appendicitis may cause hematuria (20-30% of cases) >95% of women with PID will have pus at the cervical os.
 Appendicitis may cause hematuria (20-30% of cases) >95% of women with PID will have pus at the cervical os..")
22
Rectal Examination Greatest value is in detection of heme + stools Greatest value is in detection of heme + stools Routine use in the evaluation of abdominal pain is unsupported in the literature Routine use in the evaluation of abdominal pain is unsupported in the literature Literature is scant Rectal provided no additional information in the patient with appendicitis Useful in diagnosis of prostatis, perirectal abcess, stool impactions, foreign body and GI bleed.

23
Serial Exams Useful in a subset of patients Useful in a subset of patients May be done on an outpatient basis depending on individual patient May be done on an outpatient basis depending on individual patient

24
Diagnostic Studies Adjuncts to history and physical Adjuncts to history and physical Most overused: Most overused: CBC, electrolytes, LFT’s, radiographs Most underused Most underused bHCG, UA, EKG

25
Laboratory Evaluation Amylase Amylase Neither sensitive nor specific for pancreatitis May be elevated in alcoholics without pancreatitis May be normal in recurrent pancreatitis Lipase Lipase Most useful test for acute pancreatitis

26
Laboratory Evaluation CBC CBC Most commonly ordered test in abdominal pain 10-60% of patients with appendicitis initially had a normal WBC Rarely changes management, often does not add to information gathered from H & P

27
Laboratory Evaluation Urinalysis Urinalysis Useful, but interpret with caution 20-30% of patients with appendicitis have hematuria Up to 30% of patients with ruptured AAA have hematuria

28
Plain Films Retrospective review of 1,000 patients Retrospective review of 1,000 patients 68% non-specific 23% normal 10% abnormal Useful for: Useful for: Foreign body (90% sensitivity) Bowel obstruction (43% sensitivity) Perforated viscous
 Bowel obstruction (43% sensitivity) Perforated viscous")
29
Ultrasound RUQ pain RUQ pain Lower abdominal pain in the pregnant female Lower abdominal pain in the pregnant female Transabdominal if bHCG > 5000 Transvaginal if bHCG >2000 but 2000 but <5000 Abdominal aortic aneurysms Abdominal aortic aneurysms

30
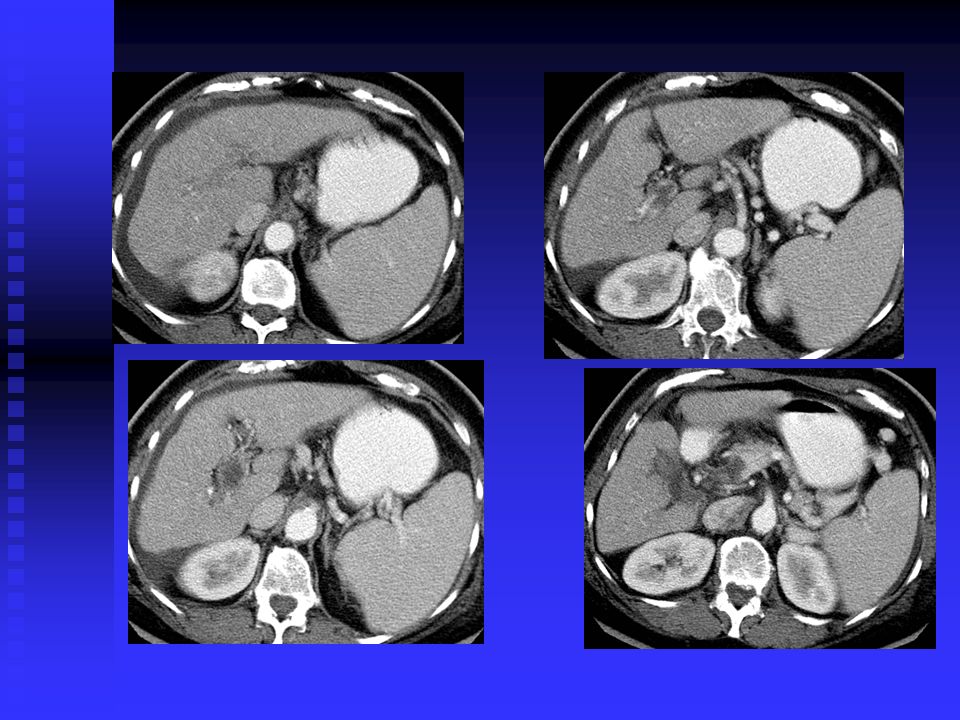
CT scanning “CT is a dark and lonely place where ED patients go to die” “CT is a dark and lonely place where ED patients go to die” Spiral CT of the abdomen provides high sens. and specificity for intra-abdominal disease Spiral CT of the abdomen provides high sens. and specificity for intra-abdominal disease Women with abdominal pain and suspected appendicitis are routinely scanned Women with abdominal pain and suspected appendicitis are routinely scanned Useful in special circumstances Useful in special circumstances Immunocompromised Altered LOC High surgical risk

31
Analgesia in Abdominal Pain OK to use analgesia in abdominal pain OK to use analgesia in abdominal pain Many studies support this Many studies support this Discuss with consultants Discuss with consultants Use in small doses, short-acting agents Use in small doses, short-acting agents Fentanyl 0.07-1.4µcg/kg with airway monitoring, low dose morphine or hydromorphone. Fentanyl 0.07-1.4µcg/kg with airway monitoring, low dose morphine or hydromorphone.

32
Electrocardiogram Useful in patients who are: Useful in patients who are: Over 40 years of age Unexplained epigastric pain Non-tender abdomen

33
The Elderly Patient Likelihood of mortality increase with age Likelihood of mortality increase with age Age > 80 mortality is 7% In patients > age 70 10% of those with abd. pain have a underlying vascular event (mesenteric ischemia, MI, AAA) Accuracy of diagnosis decreases with age Accuracy of diagnosis decreases with age Age > 80 diagnostic accuracy in ED 80 diagnostic accuracy in ED < 30% Most geriatric patients with abd. pain should have surgical evaluation in the ED
 Accuracy of diagnosis decreases with age Accuracy of diagnosis decreases with age Age > 80 diagnostic accuracy in ED 80 diagnostic accuracy in ED < 30% Most geriatric patients with abd. pain should have surgical evaluation in the ED.")
34
The Patient with HIV High incidence of drug induced pancreatitis, AIDS related cholangiopathy, enterocolitis. High incidence of drug induced pancreatitis, AIDS related cholangiopathy, enterocolitis. Drug induced pancreatitis in the HIV patient is fulminant in 10% of case Abdominal pain related to immunocompromise in 65% of cases in one study Consider CMV, lymphoma, atypical mycobacterium enteritis, crypto, sclerosing cholangitis

35
Women of Childbearing Age 1/3 of women of childbearing age with appendicitis are initially misdiagnosed 1/3 of women of childbearing age with appendicitis are initially misdiagnosed 13% of female patients presenting with lower abd. pain are pregnant 13% of female patients presenting with lower abd. pain are pregnant Tubal ligation does not exclude pregnancy Tubal ligation does not exclude pregnancy Patients in their second trimester may have tenderness in RUQ with appendicitis Patients in their second trimester may have tenderness in RUQ with appendicitis

36
Case #1 A 37 yo male with a history of recurrent abdominal pain… A 37 yo male with a history of recurrent abdominal pain…

38
Case #2 A 26 yo male without significant PMH presents complaining of ‘not feeling right’… A 26 yo male without significant PMH presents complaining of ‘not feeling right’…

39
Dieulafoy lesions

40
Case #3 A 23 yo male presents to the ED after a syncopal episode and states that he has had days of LLQ pain… A 23 yo male presents to the ED after a syncopal episode and states that he has had days of LLQ pain…

44
Case #4 You are asked to ‘medically clear’ a patient for admission to the psych floor. He is complaining of abdominal pain… You are asked to ‘medically clear’ a patient for admission to the psych floor. He is complaining of abdominal pain…

45
Acute Intermittent Porphyria

46
Things you don’t want to say in court ‘They were only constipated’ (bowel ishemia, volvulus, infection) ‘They were only constipated’ (bowel ishemia, volvulus, infection) ‘Wish I’d thought of that’ (mesenteric ischemia, AAA, MI) ‘Wish I’d thought of that’ (mesenteric ischemia, AAA, MI) ‘Looked like a kidney stone to me’ (AAA) ‘Looked like a kidney stone to me’ (AAA) ‘I wished I’d called the surgeon’ (40% of geriatric patients presenting to ED with abdominal pain require surgery) ‘I wished I’d called the surgeon’ (40% of geriatric patients presenting to ED with abdominal pain require surgery)
 ‘They were only constipated’ (bowel ishemia, volvulus, infection) ‘Wish I’d thought of that’ (mesenteric ischemia, AAA, MI) ‘Wish I’d thought of that’ (mesenteric ischemia, AAA, MI) ‘Looked like a kidney stone to me’ (AAA) ‘Looked like a kidney stone to me’ (AAA) ‘I wished I’d called the surgeon’ (40% of geriatric patients presenting to ED with abdominal pain require surgery) ‘I wished I’d called the surgeon’ (40% of geriatric patients presenting to ED with abdominal pain require surgery)")
47
Things you don’t want to say in court ‘She said there was no way she could be pregnant’ ‘She said there was no way she could be pregnant’ ‘It sure looked like PID’ (1/3 of women with appendicitis are initially misdiagnosed as PID or UTI) ‘It sure looked like PID’ (1/3 of women with appendicitis are initially misdiagnosed as PID or UTI) ‘I thought it was gastroenteritis’ ‘I thought it was gastroenteritis’ ‘The CBC was normal’ ‘The CBC was normal’
 ‘It sure looked like PID’ (1/3 of women with appendicitis are initially misdiagnosed as PID or UTI) ‘I thought it was gastroenteritis’ ‘I thought it was gastroenteritis’ ‘The CBC was normal’ ‘The CBC was normal’")
Similar presentations