Download presentation
Presentation is loading. Please wait.

1
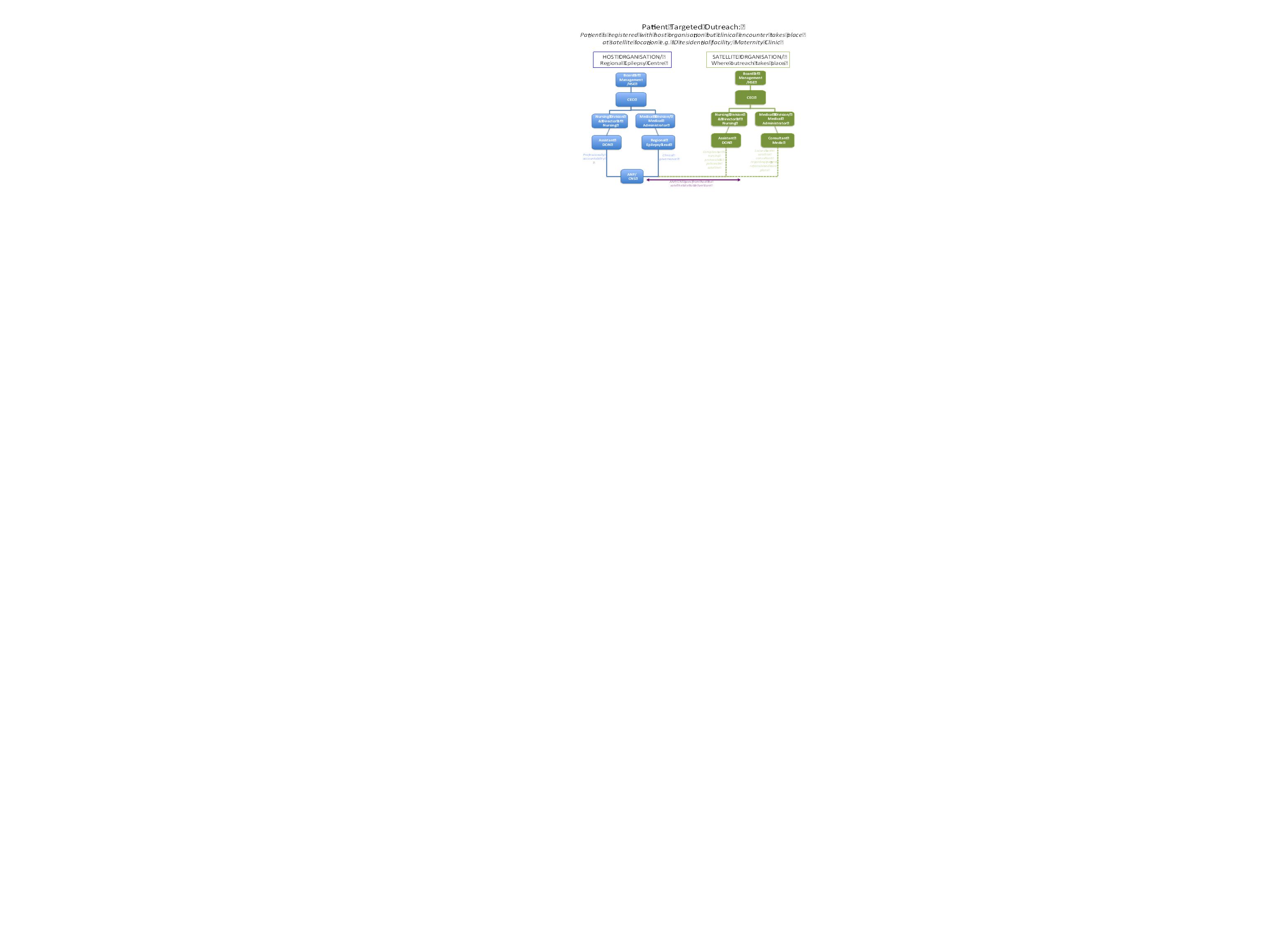
Changing the way epilepsy care is delivered - audit of a multidisciplinary epilepsy outreach clinic to an intellectual disability facility supported by an electronic patient record White M. 1, Fitzsimons M. 1, Banguiran J. 2, O Connor J. 2, Ambikapathy A. 2, Lane J. 2, Delanty N. 1 1 Beaumont Hospital, Department of Neurology, Dublin, Ireland, 2 Daughters of Charity Disability Support Services, Dublin, Ireland BACKGROUND Epilepsy is a neurological condition that affects approximately 40,000 people in Ireland 1. 25-30% of people with intellectual difficulties have epilepsy 2. People with an intellectual disability (ID) referred to hospital-based specialist epilepsy clinics, face lengthy delays from time of referral, and may experience frustrating delays on the day of clinic, leaving them stressed and uncooperative. The delays experienced reduce the numbers of people with severe behavioural problems being referred and the frequent unavailability of key nursing staff attending hospital appointments, impacts upon the quality of information available at specialist epilepsy clinics. AIM To deliver specialist epilepsy care where and when it was needed and to increase the sharing of clinical information. METHOD This study outlines the process used to set up and audit the multidisciplinary epilepsy outreach clinic in one ID residential centre over a 2 year period which was facilitated by the availability of a web based electronic patient record (EPR). Waiting times, attendance rates and the views of accompanying key members of staff attending with patients and clinical staff were sought to ascertain the benefits or otherwise of the clinic. RESULTS Fourteen clinics took place in the ID centre over 2 years One hundred appointments for 40 individual patients were scheduled 20 new patients (previously not referred) were seen (whilst this number seems small, the usual number of new referrals from this residential ID centre prior to outreach was 2-3 per year). All patients were accompanied by a key member of the nursing staff from the ID centre and all new patients had a detailed referral template completed. Outreach ClinicHospital Clinic Waiting Time for 1 st appointment ( NON URGENT) < 3 Months 12 Months Did not attend Rate3%27% Average waiting time on day of clinic Range 0-35 minutes Average 17 minutes Range 0 -120 minutes Average 75 minutes Table 1 – Waiting times in outreach clinics versus outreach clinics At the Outreach clinic staff report that…… n=15 Clients are less stressed75% There is improved continuity of care80% There are increased educational opportunities80% They are satisfied with the care between appointments 65% Table 2 – Views of key nursing staff accompanying patients to outreach clinic HOW THE CLINIC WORKS A detailed referral template for new patients was established and refined. Key nursing personnel complete the referral template in conjunction with a standard referral letter from the patient’s consultant. The referral documentation is received and triaged for outreach and an appointment scheduled. The patient’s EPR is populated prior to the appointment with the information received in the referral documents. Patients and families have the choice of attending the outreach clinic or the hospital clinic or a combination of both. The review at the ID residential centre is multidisciplinary with medical, psychiatric and key nursing personnel attending, along with the hospital based registered advanced nurse practitioner (RANP). Family members frequently attend. A neurologist personally reviews all newly referred patients at 2 outreach clinics yearly and is available to discuss return patients by phone when clinically indicated or when requested by the RANP. Follow up care between scheduled appointments is provided by the hospital-based epilepsy nurse telephone service supported by the EPR. The EPR allows services to be provided to patients in a location which is familiar to them rather than bring them to a hospital which they may perceive as a hostile environment. SETTING UP THE CLINIC A structured co-ordinated approach was used to establish and implement the clinic. A formal ‘kick off’ meeting took place between stakeholders which included management, administration, medical, nursing and IT staff. Specific governance arrangements were put in place to enable staff to deliver care off-site (see fig 1). A memorandum of understanding was agreed between the 2 organisations. Management operation procedures and standard operation procedures were developed for referral to, transfer to and from and discharge from the clinic. CONCLUSION Changing from a hospital-based epilepsy outpatient clinic to a multidisciplinary epilepsy outreach clinic supported by an EPR enhances the outpatient encounter for patients and staff from both services. REFERENCES 1. Linehan C, Kerr M.P., Walsh P.N., Brady G., Kelleher C., Delanty N., Dawson F. and Glynn M. (2010) Examining the prevalence of epilepsy and delivery of epilepsy care in Ireland, Epilepsia, 51(5):845–852. 2. Catherine W. McGrother,, Sabyasachi Bhaumik, Catherine F. Thorp, Agnes Hauck, David Branford, Joanna M. Watson (2006) Epilepsy in adults with intellectual disabilities: Prevalence, associations and service implications, Seizure, 15 (6) 376-386 Figure 1 – Governance arrangements for outreach clinic
 referred to hospital-based specialist epilepsy clinics, face lengthy delays from time of referral, and may experience frustrating delays on the day of clinic, leaving them stressed and uncooperative. The delays experienced reduce the numbers of people with severe behavioural problems being referred and the frequent unavailability of key nursing staff attending hospital appointments, impacts upon the quality of information available at specialist epilepsy clinics. AIM To deliver specialist epilepsy care where and when it was needed and to increase the sharing of clinical information. METHOD This study outlines the process used to set up and audit the multidisciplinary epilepsy outreach clinic in one ID residential centre over a 2 year period which was facilitated by the availability of a web based electronic patient record (EPR). Waiting times, attendance rates and the views of accompanying key members of staff attending with patients and clinical staff were sought to ascertain the benefits or otherwise of the clinic. RESULTS Fourteen clinics took place in the ID centre over 2 years One hundred appointments for 40 individual patients were scheduled 20 new patients (previously not referred) were seen (whilst this number seems small, the usual number of new referrals from this residential ID centre prior to outreach was 2-3 per year). All patients were accompanied by a key member of the nursing staff from the ID centre and all new patients had a detailed referral template completed. Outreach ClinicHospital Clinic Waiting Time for 1 st appointment ( NON URGENT) < 3 Months 12 Months Did not attend Rate3%27% Average waiting time on day of clinic Range 0-35 minutes Average 17 minutes Range minutes Average 75 minutes Table 1 – Waiting times in outreach clinics versus outreach clinics At the Outreach clinic staff report that…… n=15 Clients are less stressed75% There is improved continuity of care80% There are increased educational opportunities80% They are satisfied with the care between appointments 65% Table 2 – Views of key nursing staff accompanying patients to outreach clinic HOW THE CLINIC WORKS A detailed referral template for new patients was established and refined. Key nursing personnel complete the referral template in conjunction with a standard referral letter from the patient’s consultant. The referral documentation is received and triaged for outreach and an appointment scheduled. The patient’s EPR is populated prior to the appointment with the information received in the referral documents. Patients and families have the choice of attending the outreach clinic or the hospital clinic or a combination of both. The review at the ID residential centre is multidisciplinary with medical, psychiatric and key nursing personnel attending, along with the hospital based registered advanced nurse practitioner (RANP). Family members frequently attend. A neurologist personally reviews all newly referred patients at 2 outreach clinics yearly and is available to discuss return patients by phone when clinically indicated or when requested by the RANP. Follow up care between scheduled appointments is provided by the hospital-based epilepsy nurse telephone service supported by the EPR. The EPR allows services to be provided to patients in a location which is familiar to them rather than bring them to a hospital which they may perceive as a hostile environment. SETTING UP THE CLINIC A structured co-ordinated approach was used to establish and implement the clinic. A formal ‘kick off’ meeting took place between stakeholders which included management, administration, medical, nursing and IT staff. Specific governance arrangements were put in place to enable staff to deliver care off-site (see fig 1). A memorandum of understanding was agreed between the 2 organisations. Management operation procedures and standard operation procedures were developed for referral to, transfer to and from and discharge from the clinic. CONCLUSION Changing from a hospital-based epilepsy outpatient clinic to a multidisciplinary epilepsy outreach clinic supported by an EPR enhances the outpatient encounter for patients and staff from both services. REFERENCES 1. Linehan C, Kerr M.P., Walsh P.N., Brady G., Kelleher C., Delanty N., Dawson F. and Glynn M. (2010) Examining the prevalence of epilepsy and delivery of epilepsy care in Ireland, Epilepsia, 51(5):845– Catherine W. McGrother,, Sabyasachi Bhaumik, Catherine F. Thorp, Agnes Hauck, David Branford, Joanna M. Watson (2006) Epilepsy in adults with intellectual disabilities: Prevalence, associations and service implications, Seizure, 15 (6) Figure 1 – Governance arrangements for outreach clinic.")
Similar presentations

 has been commissioned by Ipswich and East Suffolk CCG to establish and run.>")


![Presented by [Insert name of presenter] [Insert title] [Insert LHD/SHN name] Month 2014 PD2014_030 Using Resuscitation Plans in End of Life Decisions.](/12/3498778/big_thumb.jpg "Presented by [Insert name of presenter] [Insert title] [Insert LHD/SHN name] Month 2014 PD2014_030 Using Resuscitation Plans in End of Life Decisions.>")


 & determining eligible patients for PPS PPS Data Collector Training April 2012 Presentation 2.>")




 Chesterfield Primary Care Trust.>")






