Download presentation
Presentation is loading. Please wait.

1
Using QOF and Service Specifications to meet HI Needs Rachel Foskett-Tharby

2
Key Points Know your population Know your gap Know QOF and actively manage the process Get the most from QOF Plugging the gaps

3
Know your population To do this successfully requires: –Close collaboration between commissioning and public health –Use of the outputs of the JSNA –Understanding of current service provision

4
Know your gap Consider in terms of: –Life years –Access to services –Proportion of patients receiving optimal treatment –Distribution – inequalities across the patch or concentrated in pockets?

5
Know QOF Strengths Weaknesses Management of process Used effectively can impact on health inequalities

6
Get the best from QOF

7
Where should we be looking? Four body systems Heart disease StrokeDiabetes Kidney disease One main mechanism Disordered blood chemistry Atheroma in blood vessels Multiple organs affected One increases risk of others Common risk factors Poor diet (fat, sugar, salt) Lack of physical activity Smoking High blood pressure Death and disability 6.2m people affected 200k deaths pa (38% of total) 17% hospital admissions 50%+ of mortality gaps
 Lack of physical activity Smoking High blood pressure Death and disability 6.2m people affected 200k deaths pa (38% of total) 17% hospital admissions 50%+ of mortality gaps.")
8
individual risk management Indicators for Individual Vascular Risk Assessment Existing guidance and tools (eg SIGN) NICE Guidelines (in current programme) Unified risk assessment support system Low Risk Individual maintenance plan Med Risk Management plan Review 1-5 yrs High Risk Intervention Eg statin Review yearly Disease Existing clinical pathways
 NICE Guidelines (in current programme) Unified risk assessment support system Low Risk Individual maintenance plan Med Risk Management plan Review 1-5 yrs High Risk Intervention Eg statin Review yearly Disease Existing clinical pathways")
13
How to add value to QOF CHD (with thanks to NST) Calculate an ‘expected’ prevalence of CVD by practice and compare with numbers on registers Have strict criteria for exceptions and exclusions from registers for QOF purposes Audit records of excepted and excluded patients Ensure excepted patients have a care plan
 Calculate an ‘expected’ prevalence of CVD by practice and compare with numbers on registers Have strict criteria for exceptions and exclusions from registers for QOF purposes Audit records of excepted and excluded patients Ensure excepted patients have a care plan")
14
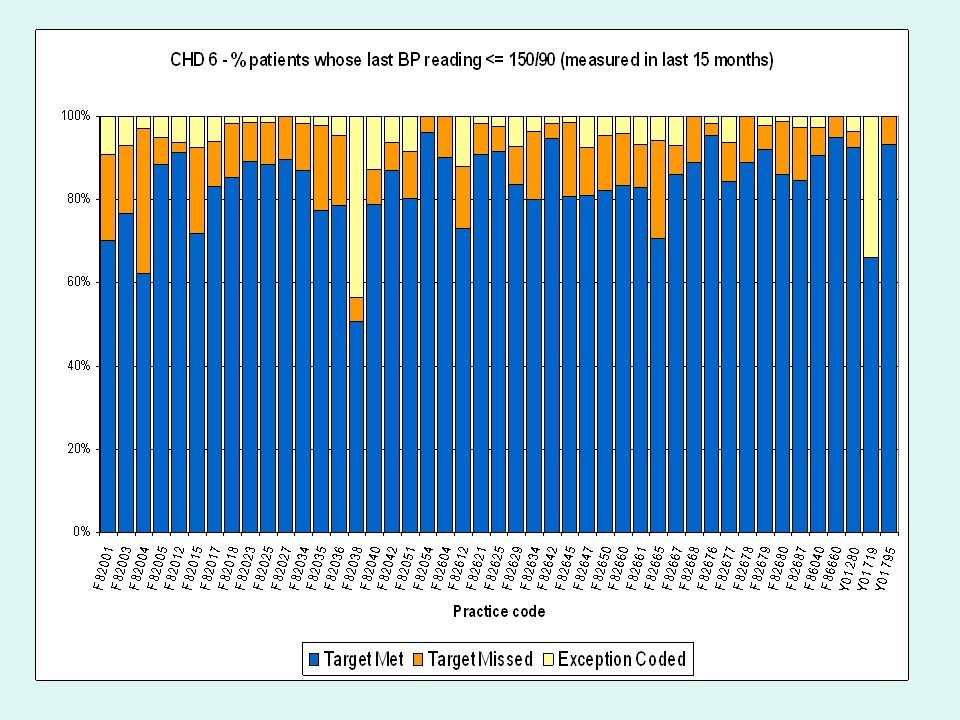
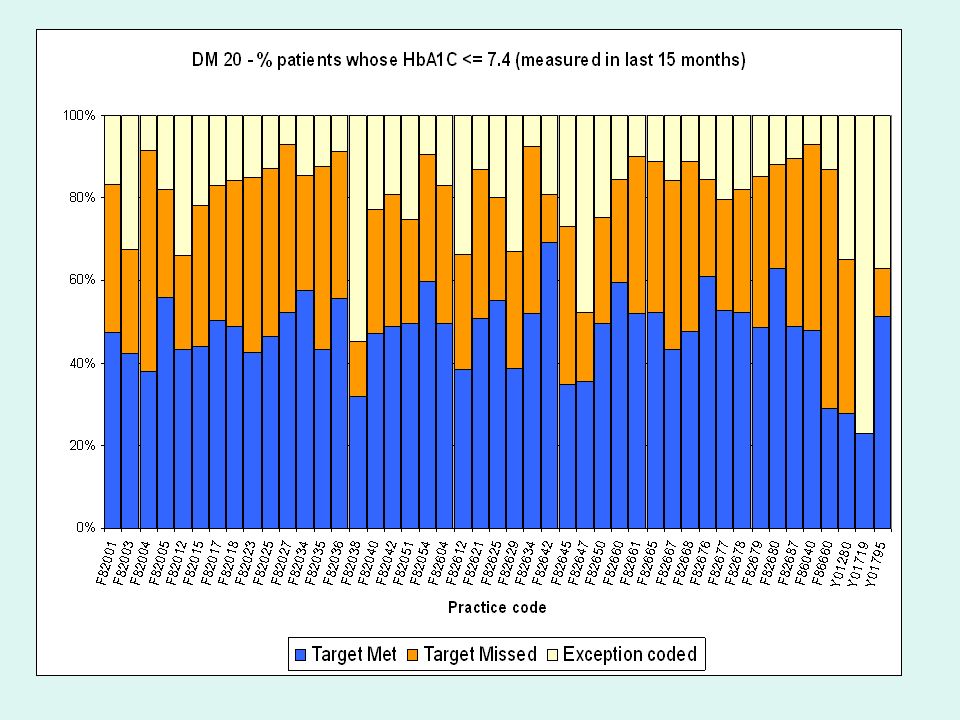
How to add value (2) Establish from QOF scores which practices are not claiming full points for CHD5, stroke 5, CHD 7 and stroke 7 Establish from QOF scores practices with scope to improve overall effectiveness of clinical practice e.g. CHD6, stroke 6, CHD8 and stroke 8 Audit practices claiming maximum points to verify outcomes

15
How to add value (3) Promote systems of medicines management and patient adherence to therapy based on active assessment and appropriate support based on cultural and language requirements Ensure referral of newly diagnosed angina patients for exercise testing and specialist assessment Consider linking to PBC plans and bonus payments
 Promote systems of medicines management and patient adherence to therapy based on active assessment and appropriate support based on cultural and language requirements Ensure referral of newly diagnosed angina patients for exercise testing and specialist assessment Consider linking to PBC plans and bonus payments")
16
QOF and APMS Contracts In groups discuss: –Strengths of using QOF in these contracts –Weaknesses of using QOF in these contracts –Risks and benefits of setting points targets as part of a contract –Strategies to manage these

17
Plug the gaps Identify areas not covered by QOF of local significance in terms of HI Identify ‘hard to reach’ populations Consider evidence based service framework Link to PBC plans

18
Service Frameworks Templates available at www.primarycarecontracting.nhs.uk www.primarycarecontracting.nhs.uk Suggested frameworks available for: –Alcohol –Obesity –Long term conditions –Support for self-care –Sexual health

19
Discussion and Questions

Similar presentations






: Can it be used for more than just paying GPs?’ Ananda Allan Senior.>")







 Helen Carter, NHS WM.>")





>")
