Download presentation
Presentation is loading. Please wait.

1
Kevin S. Hughes, MD, FACS Co-Director, Avon Comprehensive Breast Evaluation Center Massachusetts General Hospital Associate Professor of Surgery Harvard Medical School Surgeon The Newton-Wellesley Hospital Breast Center Is Post-Lumpectomy Radiation Necessary in Older Patients?

2
1.9 cm, ER+, clinical N0 Cancer Lumpectomy Plus Radiation/Boost Tamoxifen Sentinel Node Chemotherapy BRCA testing

3
1.9 cm, ER+, clinical N0 Cancer Lumpectomy Plus Radiation/Boost Tamoxifen Sentinel Node Chemotherapy BRCA testing Lumpectomy Plus Radiation/Boost Tamoxifen/AI Sentinel Node Chemotherapy BRCA testing

4
CALGB 9343 Comparison of Lumpectomy Plus Tamoxifen With and Without Irradiation in Women 70 or Older with Clinical Stage I, ER+ Breast Carcinoma Kevin S. Hughes, Lauren A. Schnaper, Constance Cirrincione, Donald Berry, Beryl McCormick, Hyman B. Muss, Clifford Hudis, Eric Winer, Barbara L. Smith Cancer and Leukemia Group B Radiation Therapy Oncology Group Eastern Cooperative Oncology Group

5
CALGB 9343 ELIGIBILITY Age 70 ELIGIBILITY Age 70Clinically Node Negative Lumpectomy, Negative Margin Tumor size 2 cm Node Negative Lumpectomy, Negative Margin Tumor size 2 cm ER Positive or Indeterminate STRATIFICATION Age < 75 75 Axillary Dissection Yes No RadiationTamoxifen Tamoxifen RANDOMIZERANDOMIZERANDOMIZERANDOMIZE

6
CALGB 9343 Opened July 15, 1994 Closed February 26, 1999 647 patients –Eligible 631 –Ineligible 5 –Canceled/Never treated 11 Median follow-up 12 years

7
Patient characteristics RT+Tam Tam Total treated 317 319 Age >75 176 (56%)172 (54%) ER Positive308 (97%)310 (97%) Size < 2cm295 (93%)296 (93%) No Ax dissection 200 (63%)203 (64%)
172 (54%) ER Positive308 (97%)310 (97%) Size < 2cm295 (93%)296 (93%) No Ax dissection 200 (63%)203 (64%)")
8
IBTR (Ipsilateral Breast Tumor Recurrence) 91% 98%
 91% 98%")
9
Ipsilateral cancer risk 40 and under RT 70 above no RT LCIS

10
Radiation decreases local recurrence by ~7% Does it do anything else?

12
No RT Mastectomy Lumpectomy IBTR 27 RT IBTR 6 4 18 10

17
Actuarial survival for given ages at entry D. Berry 8/28/11

18
Ultimate Outcome

19
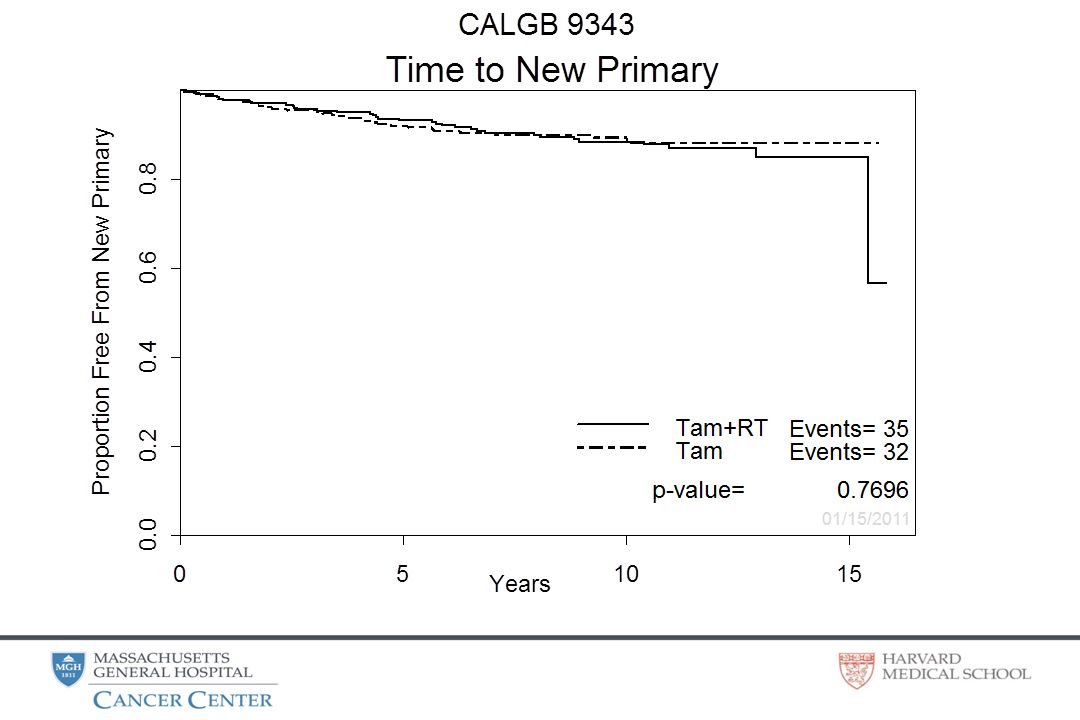
Breast Recurrence Less Ultimate Mastectomy Same Second primary cancer Same Distant metastasis Same Death Same Death Other CausesSame Death from breast cancerSame 22 women With modern margins and AI’s, RT will likely have even less benefit CONCLUSION: In older women, the benefits of radiation after lumpectomy are small

21
1.9 cm, ER+, clinical N0 Cancer Lumpectomy Plus Radiation/Boost Tamoxifen Sentinel Node Chemotherapy BRCA testing Lumpectomy Plus Radiation/Boost Tamoxifen/AI Sentinel Node Chemotherapy BRCA testing

22
1.9 cm, ER+, clinical N0 Cancer Lumpectomy Plus Radiation + Boost Tamoxifen Sentinel Node Chemotherapy Lumpectomy Tam/AI

23
When does this woman…become this woman?

24
Breast Recurrence Less Ultimate Mastectomy Same Second primary cancer Same Distant metastasis Same Death Same Death Other CausesSame Death from breast cancerSame 22 women Study is mature: 12 years Median, Half of patients dead With modern margins and AI’s, RT will likely have even less benefit CONCLUSION: In older women, the benefits of radiation after lumpectomy are small

25
1.9 cm, ER+, clinical N0 Cancer Lumpectomy Plus RT/Boost Tamoxifen Sentinel Node Chemotherapy BRCA testing Agreement: Elderly women need less treatment Lumpectomy OR Tam/AI OR Tam/AI/RT

26
1.9 cm, ER+, clinical N0 Cancer Lumpectomy Plus Radiation + Boost Tamoxifen Sentinel Node Chemotherapy BRCA testing Agreement: Elderly women need less treatment Lumpectomy OR Tam/AI OR Tam/AI/RT Continued discussion: Who are the elderly?

27
Conclusions Every elderly woman does not need –lumpectomy,sentinel node,RT+Boost,Tam/AI,Chemo Breast irradiation provides less benefit with age Breast irradiation plus Tam/AI is often excessive Question: Who are the elderly? Elderly women need individualized treatment

29
Axillary recurrence TamRTTam 317319 No ax dissection200203 Ax Recurrence0 6 (3%)
")
30
Breast Recurrence Less Ultimate Mastectomy Same Second primary cancer Same Distant metastasis Same Death Same Death Other CausesSame Death from breast cancerSame Benefits of RT are small N (% at 10 yeas) N (% at 10 years) 22 women Study is mature: 12 years Median, Half of patients dead With modern margins and AI’s, RT will likely have even less benefit
 N (% at 10 years) 22 women Study is mature: 12 years Median, Half of patients dead With modern margins and AI’s, RT will likely have even less benefit")
31
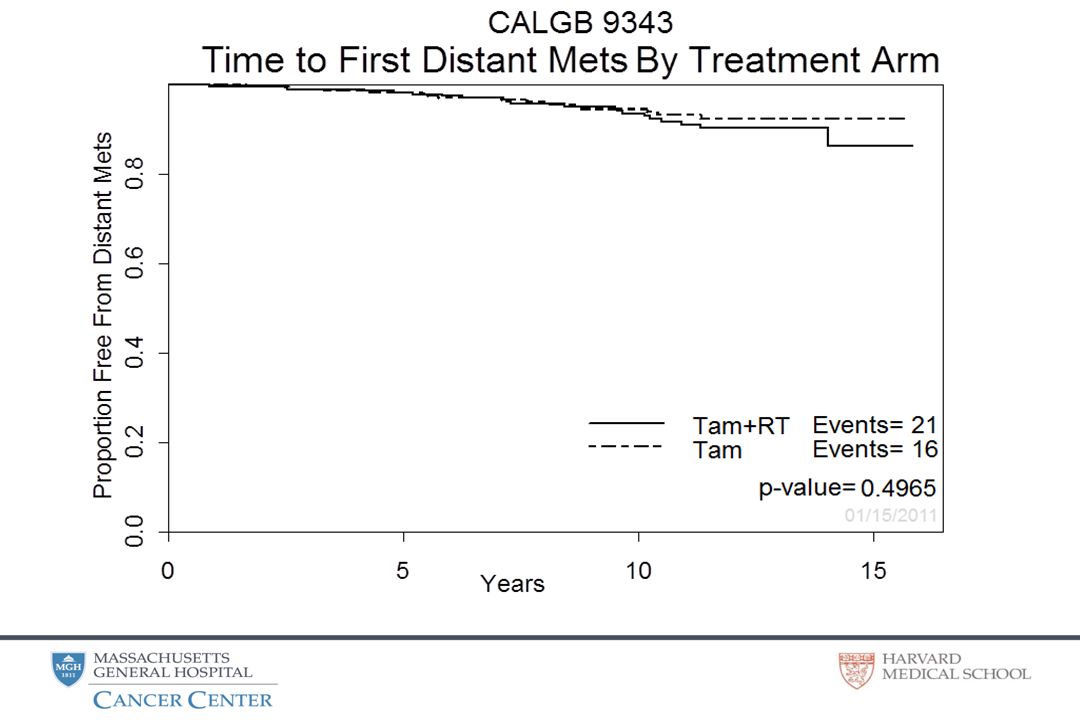
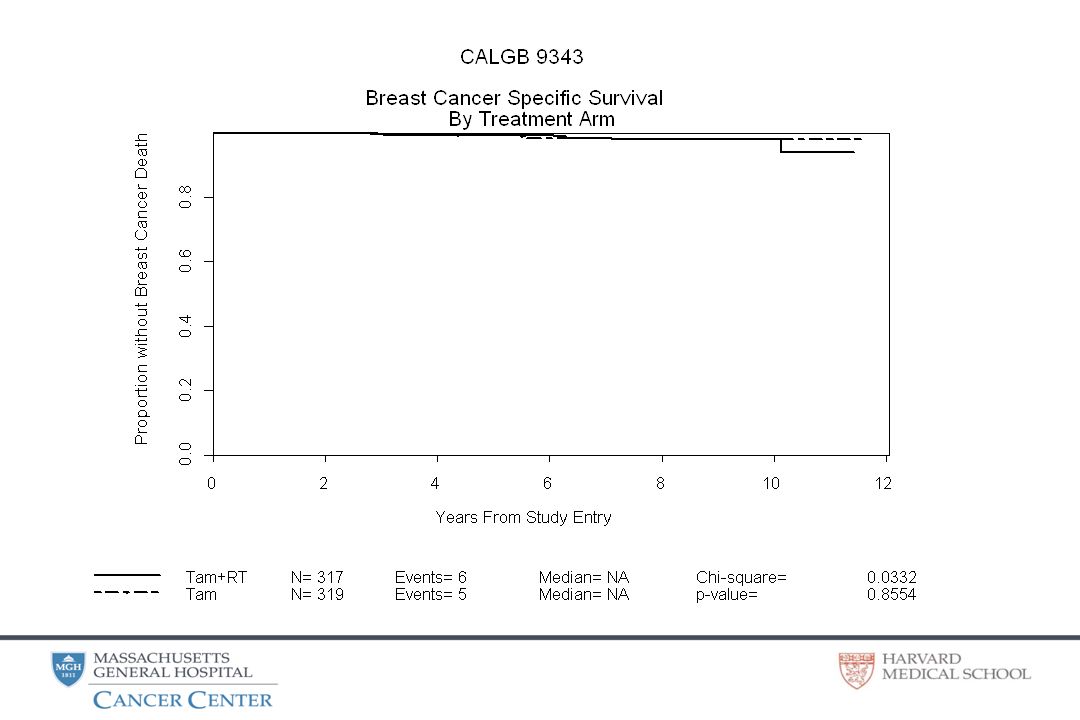
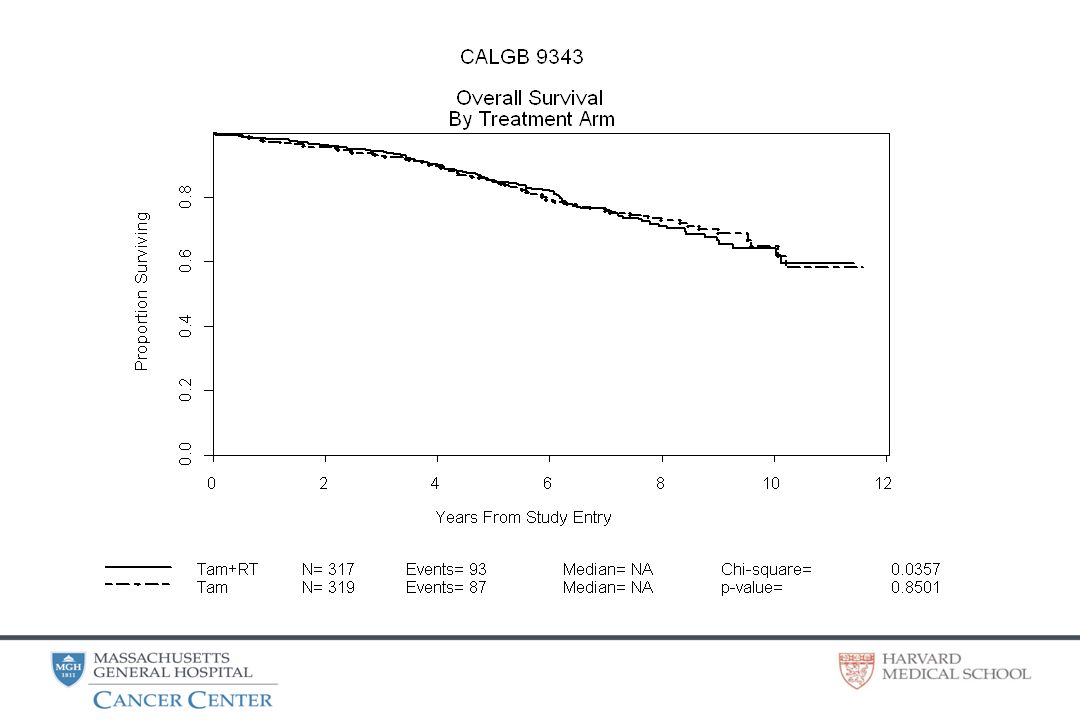
In older women, the benefits of radiation after lumpectomy are small Breast recurrence ~7% Radiate 319 women to avoid 21 in breast recurrences Ultimate breast preservationNS Second primary cancerNS Distant metastasesNS Death breast cancerNS Death from any causeNS 21 women Omitting Radiation in women 70 and above with Clinical Stage I breast cancer is a reasonable alternative for our patients

32
Managing the elderly If mastectomy needed –Preop chemo or endocrine possible & needed Yes=>Try No=>Do Mastectomy (With sentinel node) If breast preservation possible –Clinically positive node Lumpectomy/Axillary dissection –Tumor ER- or over 2 cm Lumpectomy/Sentinel node –If Clinical Stage I and ER+ If chemotherapy a possibility –Do sentinel node If chemotherapy NOT a possibility –Sentinel node optional (Not encouraged)
 If breast preservation possible –Clinically positive node Lumpectomy/Axillary dissection –Tumor ER- or over 2 cm Lumpectomy/Sentinel node –If Clinical Stage I and ER+ If chemotherapy a possibility –Do sentinel node If chemotherapy NOT a possibility –Sentinel node optional (Not encouraged)")
34
No RT IBTR 20 RT IBTR 4

35
No RT Mastectomy Lumpectomy IBTR 20 RT IBTR 4 4 11 9

36
In older women, the benefits of radiation after lumpectomy are small Breast recurrence ~7% Radiate 319 women to avoid 21 in breast recurrences Ultimate breast preservationNS Second primary cancerNS Distant metastasesNS Death breast cancerNS Death from any causeNS 21 women

37
CONCLUSION: In older women, the benefits of radiation after lumpectomy are small Breast recurrence ~7% Radiate 319 women to avoid 21 in breast recurrences Ultimate breast preservationNS Second primary cancerNS Distant metastasesNS Death breast cancerNS Death from any causeNS 21 women Study is mature: 12 years Median, Half of patients dead With modern margins and AI’s, RT will likely have even less benefit

38
Axillary recurrence

42
CALGB 9343: All Patients Dead Breast 2 % Dead Other 27% Alive 71%

43
Morbidity statistically inferior in RT arm Physician assessment Patient assessment 4 monthsCosmesisPain TendernessFibrosis Skin color changes Breast edema 1 year CosmesisPain TendernessFibrosisSkin color changes Breast edema Fibrosis 2 years Skin color changesSkin color changes Breast edemaCosmesis Fibrosis 4 yearsNo differencesNo differences

44
Benefit of RT LocoRegional recur5.9% Ultimate Breast Preservation0 % Distant Metastases0 % Death Breast Cancer0 % Death Any Cause0 %

45
Benefit of RT LocoRegional recur5.9% Ultimate Breast Preservation0 % Distant Metastases0 % Death Breast Cancer0 % Death Any Cause0 % 5 YR results verified at 8.2 YRS

46
Early 1990’s: Was RT always needed after conservative surgery? Possible groups –Elderly –Small tumors –Tamoxifen

47
Summary of Randomized Trials: Lumpectomy + Tam vs Lumpectomy + Tam + RT NSABPCanadianCALGBScottishAustrian B-21FylesHughesStewartPotter AgeAny50 and over70 and overAny Size<1 cm< 5 cm< 2 cm< 4 cm< 3 cm Tamoxifen2 / 3 armsyes PopulationSmall tum / younger large tum / older Small tum / older Large tum / younger Large tum / younger # of pts1,009769636585836 Median FU8 y 6 y3.5 y

48
Summary of Randomized Trials: Lumpectomy + Tam vs Lumpectomy + Tam + RT NSABPCanadianCALGBScottishAustrian B-21FylesHughesStewartPotter Tam16.5%11.5%7%25%3.1% Tam + RT2.8%3.8%1%3%0.2%

49
Summary of Randomized Trials: Older Women NSABP B-21 Canadian Fyles CALGB Hughes Age>70>60> 70 Size< 1cm < 2cm # of pts100193636 Tam7%4.8%7% Tam + RT0 %4.2%1%

50
Can we Vs should we?

52
Managing the elderly Lumpectomy ≤ 2 cm & ER+ Adjuvant treatment RT plus Tam/AI Tam/AI RT Sentinel node IF chemo being considered > 2 cm &/or ER- Sentinel node plus RT Mastectomy

53
Treating breast cancer in the elderly differently makes medical sense Or is discrimination

55
I can’t define elderly, but I know it when I see it. Paraphrase of Supreme Court Decision Potter Stewart Miller VS California, 1973 Miller VS California, 1973

56
2004: Median 5 Yr Hughes NEJM, 2004

57
Mastectomy Lumpectomy IBTR Lumpectomy + RT Local recurrence does not preclude breast preservation

58
GOALS Prevent Breast Recurrence Prevent Axillary Recurrence Prevent Systemic Recurrence Preserve the Breast Minimize Treatment

59
Mission of the American Academy of Pediatrics change the custom of treating children as miniature adults

60
Mission of the American Academy of Pediatrics change the custom of treating children as miniature adults The mission of Geriatric Oncology should be similarly described.

61
CALGB 9343: All Patients Dead Breast 2 % Dead Other 27% Alive 71%

62
CALGB 9343: Deceased Dead Breast 6 % Dead Other 94%

63
For older women… these hazards would exceed the estimated benefits Breast Cancer Trialists’ Collaborative Group Lancet 2000; 355: 1757–70 …if …radiotherapy regimens … can … yield most of the benefit while avoiding most of the hazard, 20- year survival could be moderately improved …

64
NEJM 2004: Median 5 Yr Hughes NEJM, 2004 Criticism FU too short Curves will separate Need longer FU!

65
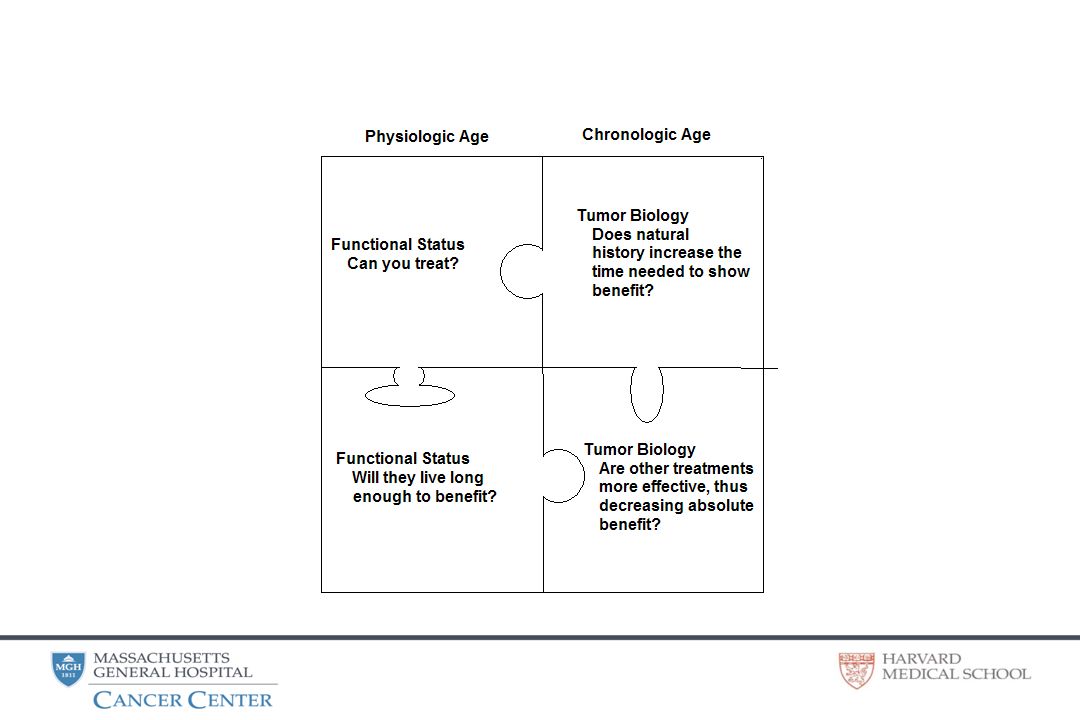
Can we? Should we? Patient factors are dependent on physiologic age Tumor factors are dependent on chronologic age

66
FEMALE POPULATION (in thousands) USA - November 1, 1998 Age Group 138,200 5-910-14
 USA - November 1, 1998 Age Group 138,")
67
Biologic factors in older patients Doubling Time by Xeromammography Cancer Research 46:970,1986 Spratt et al Cancer Research 46:970,1986

68
Histopathology of Breast Cancer in Relation to Age CJ Fisher, et al, Guy’s Hopital BrJCa 75:593,1997

69
Superimpose 5 + 8.2 Yrs

70
Can we…? Patient factors Dependent on physiologic age

71
New Approach to Geriatric Oncology Should we…? –Will the patient live long enough to benefit? Does less aggressive cancer increase the time needed to show benefit? –Does tumor response abrogate the need for multimodality therapy?

72
Decreased local recurrence Biologic factors

73
Decreased local recurrence Decreased time at risk

74
Decreased local recurrence Tamoxifen

75
Local recurrence does not preclude breast preservation

76
IBTR (Ipsilateral Breast Tumor Recurrence)
")
77
SECOND PRIMARY CANCER TamRTTam TOTAL36 (12%)33 (9%) Breast1210 Leukemia12 MDS01 Lymphoma43 Colorectal65 Epiglottis10 Peritoneum01 GI,NOS10 Liver02 Pancreas01 Spleen10 Bladder10 Endometrium31 Lung47 Melanoma20
33 (9%) Breast1210 Leukemia12 MDS01 Lymphoma43 Colorectal65 Epiglottis10 Peritoneum01 GI,NOS10 Liver02 Pancreas01 Spleen10 Bladder10 Endometrium31 Lung47 Melanoma20")
78
Initial Approach to Geriatric Oncology Can we…? –Can we do the same surgery? –Can we use the same drugs? –Can we radiate?

79
Women could now choose breast preservation or mastectomy

80
Can we…? Patient factors Dependent on physiologic age

81
In Breast Recurrence from another trial

82
STANDARD THERAPY

83
Cancer. 1981 May 15;47(10):2358-63. Survival following breast cancer surgery in the elderly. Herbsman H, Feldman J, Seldera J, Gardner B, Alfonso AE. Herbsman HFeldman JSeldera JGardner BAlfonso AE “there is little justification for avoiding conventional operative treatment in elderly patients with breast cancer solely on the basis of advanced age.” Early papers on cancer in the elderly evaluated the question: ‘Can we?”

84
Should we? Patient factors Dependent on physiologic age Tumor factors Dependent on chronologic age

85
Can we? Should we? Patient factors Dependent on physiologic age Tumor factors Dependent on chronologic age

86
NSABP B - 06 Lumpectomy + Axillary Dissection Lumpectomy + Axillary Dissection Mastectomy Mastectomy n 719 731 713 n 719 731 713 IBTR 40.9% 12.4% N/A IBTR 40.9% 12.4% N/A Survival 65% 71% 68% Survival 65% 71% 68% Lumpectomy + Axillary Dissection & RT Lumpectomy + Axillary Dissection & RT vs

87
Early 1990’s: Did any group NOT need RT after conservative surgery? –Elderly –Small tumors –Tamoxifen

88
RADIATION AFTER AGE 70 No change in survival Decreased local recurrence Biologic factors in patients over 50 Decreased time at risk Tamoxifen Local recurrence does not preclude breast preservation

89
RT: No change in survival Authorn Follow-up RT No RT Authorn Follow-up RT No RT Fisher930 10 Years 71% 65% Liljegren381 5 Years 91% 87.1% Veronesi567 4 Years No Difference Clark837 3 Years 91-96% 90-96%

90
Effects of radiotherapy and of differences in the extent of surgery for early breast cancer on local recurrence and 15-year survival: an overview of the randomised trials Early Breast Cancer Trialists’ Collaborative Group, Lancet 2005; 366: 2087–2106 By contrast, more than half the 15-year breast cancer mortality (and much more than half of any such treatment effects on breast cancer mortality) occurred after the first 5 years. Some local treatment comparisons (eg, axillary clearance vs effective axillary radiotherapy; mastectomy vs BCS plus effective radiotherapy; post-mastectomy radiotherapy in nodenegative disease) involved little (10%) absolute difference in the 5-year risk of local recurrence and, in aggregate, these comparisons also involved little difference in 15-year breast cancer mortality (figure 5, upper panel).
 involved little (10%) absolute difference in the 5-year risk of local recurrence and, in aggregate, these comparisons also involved little difference in 15-year breast cancer mortality (figure 5, upper panel)..")
91
Decreased local recurrence MILAN TRIAL III Quandrantectomy and Axillary Dissection Only Age n Local Recurrence 45 years 6311 (17.5%) 46-55104 9 (8.7%) >55 years 106 4 (3.8%)
 (8.7%) >55 years (3.8%)")
92
NEJM 351: 963, 2004 Fyles (Princess Margaret) Age at diagnosis#Local Relapse 50–59 yr1836.0 60–69 yr2613.8 ≥70 yr3253.2
 Age at diagnosis#Local Relapse 50–59 yr –69 yr ≥70 yr3253.2")
93
Decreased Time at Risk

94
NSABP B-14 53 MONTH ANALYSIS IBTR1.9% 4.3% IBTR1.9% 4.3% TamoxifenPlacebo Decreased local recurrence: Tamoxifen

95
No RT Mastectomy Lumpectomy IBTR RT IBTR

96
Concerns regarding this study Patients randomized to receive no radiation would be inappropriately under-treated

97
No RT IBTR 28 RT IBTR 6

98
Concerns regarding this study Patients randomized to receive no radiation would be inappropriately under-treated Patients randomized to receive radiation therapy would be inappropriately over-treated

99
In Breast Recurrence from another trial

100
Recurrence Rates after Treatment of Breast Cancer with Standard Radiotherapy with or without Additional Radiation Bartelink, N Engl J Med 2001; 345:1378-1387 Tam 70 and above Lumpectomy, RT/Boost 40 or younger

101
Ipsilateral breast from another study AtypiaIpsilateral 5 year riskIpsilateral 10 year risk Type ADH (n=1233)0.0273540.08439 ALH (n=851)0.053390.114086 LCIS (n=595)0.0537810.096924 Borderline (n=370)0.040020.08236
 ALH (n=851) LCIS (n=595) Borderline (n=370)")
102
LCIS AtypiaIpsilateral 5 year riskIpsilateral 10 year risk Type ADH (n=1233)0.0273540.08439 ALH (n=851)0.053390.114086 LCIS (n=595)0.0537810.096924 Borderline (n=370)0.040020.08236
 ALH (n=851) LCIS (n=595) Borderline (n=370)")
Similar presentations










: Department.>")










>")





