Download presentation
Presentation is loading. Please wait.

1
October 2, 2015 2015 Annual Tennessee STEMI Meeting

2
Financial Disclosure: none Unlabeled/Unapproved Disclosure: none Kevin Maquiling, M.D., FACC Cathy Malone, MMHC, BSN Middle Tennessee Regional Showcase

3
Largest hospital between Nashville, TN and Huntsville, AL 275 bed facility with a medical staff of more than 200 physicians and 2,000 employees Serves a region of more than a quarter of a million people in southern middle Tennessee Maury Regional Medical Center

4
Service Area

5
Maury Regional Medical Center MRMC is proud to have been recognized for its quality of care and operations Services include: Cancer Center Emergency Services Heart Center Neonatal Intensive Care Neurology and Neurosurgery Orthopedic Services Surgical Services Women’s Center

6
Recent recipient of the TNCPE 2014 Excellence Award 2015 - Formally recognized as a “Planetree Designated®” Patient-Centered Hospital It’s one of 28 hospitals in the U.S. and the first in Tennessee. Quality of Care

7
Disease-Specific Care for Inpatient Diabetes Disease Specific Care for Joint Replacement - Hips Disease Specific Care for Joint Replacement – Knees Disease Specific Care for Sepsis Disease Specific Congestive Heart Failure The Joint Commission

9
MRMC’s Team

11
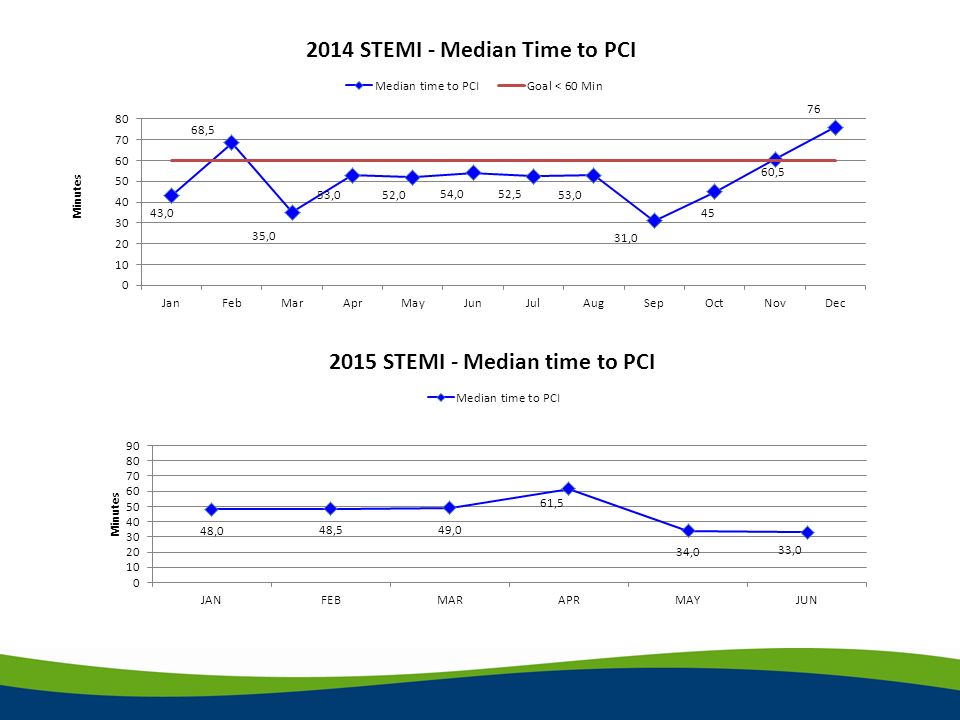
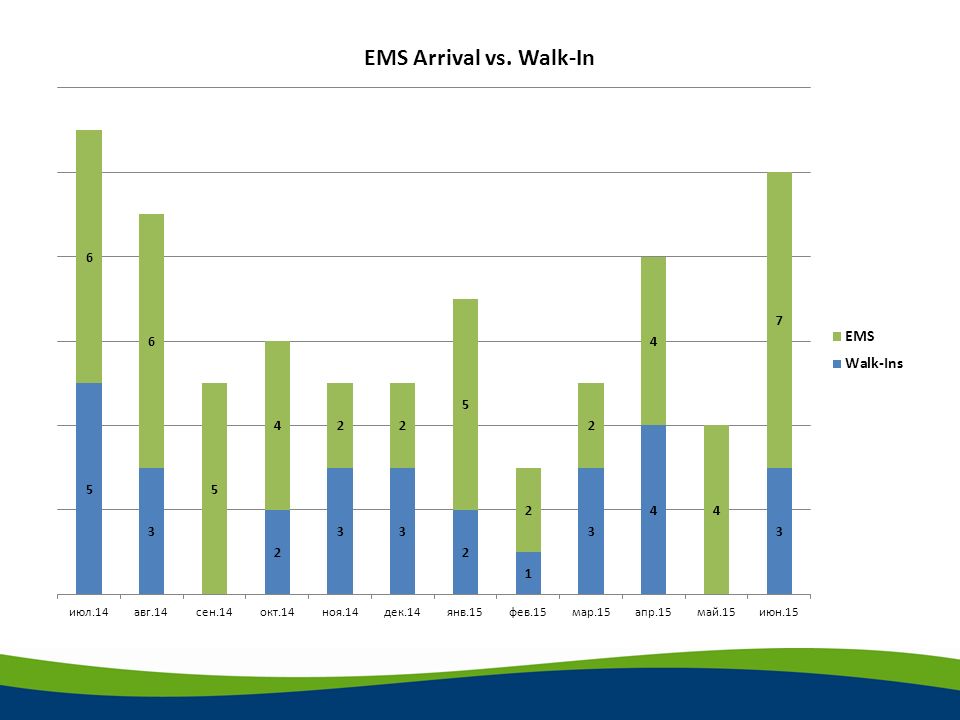
Success # 1 Community Wide Education on calling 911 …………and a personal story

13
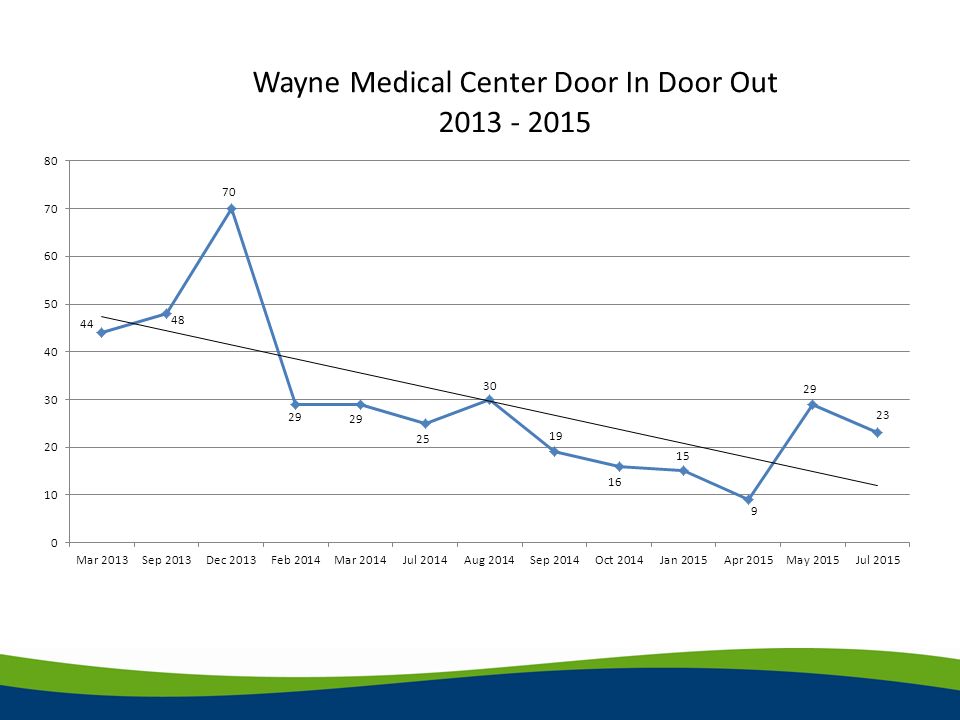
Success # 2 Lean Project: Improving Door In to Door Out (DIDO) Wayne Medical Center
 Wayne Medical Center")
14
Issue and Background Issue: When a STEMI is diagnosed at Wayne Medical Center (WMC), there is a delay in the transfer to Maury Regional Medical Center (MRMC). Background: Once a STEMI is diagnosed, the time it takes to get the medications from pharmacy, call for transport, wait for an accepting physician, finish the paperwork and get the patient out the door is greater than 50 minutes.

15
Current Condition Everyone involved brought together STEMI transfers reviewed for areas of opportunity Each OFI broken down into manageable categories Opportunities identified: Delay: waiting on accepting physician Delay: waiting on cardiologist to give med orders Delay: using helicopter to transfer patients Delay: RN does not have medications readily accessible Delay: RN hold up transport of patient to give report Delay: RN (after hours) gives report to ED charge nurse if cath team not present yet
 gives report to ED charge nurse if cath team not present yet")
16
Problem Analysis WMC ED physician waits on cardiology to call back before starting transfer of patient. Why? Not all ED physicians aware of one call acceptance at MRMC Why? Turnover of ED physicians at WMC = new ED physicians WMC ED physicians wait to speak with cardiologist prior to initiating medications to STEMI patient. Why? Not aware of transfer protocols established by MRMC cardiologists.

17
Problem Analysis (continued) WMC ED physicians use Air EMS to transport STEMI patients. Why? They think it is faster than ground transportation Why? New ED physicians that do not live in area are not aware of time requirements of flying patients and logistics of transfer at MRMC. RN does not have easy access to protocol medications or supplies. Why? Some stocked in accudose, others in pharmacy. Why? Not enough room in accudose for rarely used medications.

18
Problem Analysis (continued) RN delays transfer of patient to give report to MRMC Why? In the past, always told had to speak to accepting RN first. Why? That was the practice. RN calls ED charge nurse after cath lab hours to give report Why? Cath lab personnel not on site yet. Why? After hours, they are on call.

19
Target Condition Eliminate delays and make it easier for WMC to transfer STEMI timely! Call is made to Wayne County EMS at the same time MRMC is called to notify of STEMI transfer. Protocols are initiated by physician – RN uses STEMI kit with all medications and supplies in accudose. Patient is transferred by ground. All paperwork is faxed after the patient leaves the facility. Upon arrival of cath team, one member calls WMC and receives report from RN.

20
Countermeasures/Implementation Plan Education to WMC staff regarding one call acceptance, MRMC transfer medication protocols, Door In/Door Out goal of less than 30 minutes and preferred use of ground transport. - implemented by Dr. McMurray by January 31 st, 2014. Establish STEMI kit in Accudose with all medications and supplies needed for transfer STEMI to MRMC. - implemented by Karen Johnson and Brenda Bishop by February 1 st, 2014. Meet with Wayne County EMS director to establish protocols for for STEMI transfers to MRMC. - implemented by Karen Johnson and Brenda Bishop by February 1 st, 2014.

21
Countermeasures/Implementation Plan Educate cath lab staff at MRMC of calling for report upon arrival. - implemented by Brenda Bishop by February 1 st, 2014. Educate House Supervisors to prompt WMC ED physicians to expedite transfer of STEMI patients: not to wait for cardiology to call them back and to fax paperwork after patient has left facility. - implemented by Brenda Bishop by February 1 st, 2014. FOLLOW UP March 1 st, 2014 – Brenda, Karen and Dr. McMurray met to discuss any other implementations or needs concerning STEMI patients.

23
Challenges/Works in Progress Community Education Reducing DIDO times at the other transferring facilities in our region.

24
“ If everyone is moving forward together, then success takes care of itself” - Henry Ford

25
Thank You!!

Similar presentations


 JCAHO Core Measure Project Loyola University Medical Center Team Members: K. McLean MD, M. Morrow MSN, J. Cochran BSN,>")
 30 hours per week for 10 months Part Time Eves – 3 eves per.>")





 patients is through our emergency room. Improvement.>")








 Intensive Analysis Wm. Todd Gray, D.O., F.A.C.C. June.>")

