Download presentation
Presentation is loading. Please wait.

1
Lynn M. Keenan, MD, FACP, FCCP Lynn M. Keenan, MD, FACP, FCCP Pulmonary/Critical Care Medicine Northwest Hospital and Medical Center WAPA January 2013 Lynn M. Keenan, MD, FACP, FCCP Lynn M. Keenan, MD, FACP, FCCP Pulmonary/Critical Care Medicine Northwest Hospital and Medical Center WAPA January 2013 Overview of COPD

2
Disclosures Speakers Bureau Boehringer Ingelheim Speakers Bureau Boehringer Ingelheim I hate tobacco abuse I hate tobacco abuse I am a old SNL and Seinfeld Fan I am a old SNL and Seinfeld Fan If you were here last year, I updated my jokes If you were here last year, I updated my jokes I miss “The Closer”, doesn’t everyone? I miss “The Closer”, doesn’t everyone? Speakers Bureau Boehringer Ingelheim Speakers Bureau Boehringer Ingelheim I hate tobacco abuse I hate tobacco abuse I am a old SNL and Seinfeld Fan I am a old SNL and Seinfeld Fan If you were here last year, I updated my jokes If you were here last year, I updated my jokes I miss “The Closer”, doesn’t everyone? I miss “The Closer”, doesn’t everyone?

3
Clinical Course of COPD Air Trapping Expiratory Flow Limitation Breathlessness Inactivity Poor Health-Related Quality of Life Hyperinflation Deconditioning COPD DisabilityDisease progressionDeath Reduced Exercise Capacity COPD Exacerbations Adapted from Decramer M. Eur Respir Rev. 2006;15:51-57.

4
COPD Definition and Epidemiology GOLD: Global Initiative for Chronic Obstructive Lung Disease GOLD: Global Initiative for Chronic Obstructive Lung Disease Goals: awareness, decrease mortality and morbidity Goals: awareness, decrease mortality and morbidity Improve prevention and management Improve prevention and management Systemic consequences: persistent systemic inflammatory state leads to: Systemic consequences: persistent systemic inflammatory state leads to: Decreased fat-free mass, impaired systemic muscle function, anemia, osteoporosis, depression, pulmonary hypertension, cor pulmonale Decreased fat-free mass, impaired systemic muscle function, anemia, osteoporosis, depression, pulmonary hypertension, cor pulmonale GOLD: Global Initiative for Chronic Obstructive Lung Disease GOLD: Global Initiative for Chronic Obstructive Lung Disease Goals: awareness, decrease mortality and morbidity Goals: awareness, decrease mortality and morbidity Improve prevention and management Improve prevention and management Systemic consequences: persistent systemic inflammatory state leads to: Systemic consequences: persistent systemic inflammatory state leads to: Decreased fat-free mass, impaired systemic muscle function, anemia, osteoporosis, depression, pulmonary hypertension, cor pulmonale Decreased fat-free mass, impaired systemic muscle function, anemia, osteoporosis, depression, pulmonary hypertension, cor pulmonale

5
COPD Definition and Epidemiology Largest disease burden Largest disease burden >age 40: 9-10 % adults, greater in men >age 40: 9-10 % adults, greater in men Affects 10% general population and 50% heavy smokers Affects 10% general population and 50% heavy smokers > 80% pts. Under diagnosed survey 8,215 pts. > 80% pts. Under diagnosed survey 8,215 pts. 16 million people with 110,000 deaths 2010 16 million people with 110,000 deaths 2010 3rd leading cause of death 2011 3rd leading cause of death 2011 3% mortality for hospital admission 3% mortality for hospital admission 50% mortality for ICU admission within 2 years 50% mortality for ICU admission within 2 years Largest disease burden Largest disease burden >age 40: 9-10 % adults, greater in men >age 40: 9-10 % adults, greater in men Affects 10% general population and 50% heavy smokers Affects 10% general population and 50% heavy smokers > 80% pts. Under diagnosed survey 8,215 pts. > 80% pts. Under diagnosed survey 8,215 pts. 16 million people with 110,000 deaths 2010 16 million people with 110,000 deaths 2010 3rd leading cause of death 2011 3rd leading cause of death 2011 3% mortality for hospital admission 3% mortality for hospital admission 50% mortality for ICU admission within 2 years 50% mortality for ICU admission within 2 years

6
High BODE index Multiple severe exacerbations CVD Decreased FEV 1 Dyspnea Hyperinflation (IC/TLC ≤ 25%) Pulmonary hypertension Impaired Exercise Performance Depression Low BMI Predictors of COPD Mortality
 Pulmonary hypertension Impaired Exercise Performance Depression Low BMI Predictors of COPD Mortality")
7
2 Million, Severe Disease* 10 Million 12+ Million at risk and unidentified SUBCLINICAL COPD Clinical COPD – Tip of the Iceberg Adapted from Mannino DM, et al. MMWR Morb Mortal Wkly Rep. 2002;51(SS06):1-16.
:")
8
Airflow Limitation Starts Before Symptoms are Evident

9
COPD Definition and Epidemiology Women >er mortality Women >er mortality poorer prognosis with BMI of 25 and lower BODE index poorer prognosis with BMI of 25 and lower BODE index Faster decline in FEV1 has a modest increased risk of death and time to COPD related hospitalization Faster decline in FEV1 has a modest increased risk of death and time to COPD related hospitalization Severe COPD: increased mortality with more advanced age, lower BMI, oxygen supplementation, greater hyperinflation, also patients at increased risk lung cancer, atherosclerosis, and osteoporosis Severe COPD: increased mortality with more advanced age, lower BMI, oxygen supplementation, greater hyperinflation, also patients at increased risk lung cancer, atherosclerosis, and osteoporosis Presence of chronic cough/sputum identifies a subgroup with higher risk of developing COPD, independent of smoking habits Presence of chronic cough/sputum identifies a subgroup with higher risk of developing COPD, independent of smoking habits Women >er mortality Women >er mortality poorer prognosis with BMI of 25 and lower BODE index poorer prognosis with BMI of 25 and lower BODE index Faster decline in FEV1 has a modest increased risk of death and time to COPD related hospitalization Faster decline in FEV1 has a modest increased risk of death and time to COPD related hospitalization Severe COPD: increased mortality with more advanced age, lower BMI, oxygen supplementation, greater hyperinflation, also patients at increased risk lung cancer, atherosclerosis, and osteoporosis Severe COPD: increased mortality with more advanced age, lower BMI, oxygen supplementation, greater hyperinflation, also patients at increased risk lung cancer, atherosclerosis, and osteoporosis Presence of chronic cough/sputum identifies a subgroup with higher risk of developing COPD, independent of smoking habits Presence of chronic cough/sputum identifies a subgroup with higher risk of developing COPD, independent of smoking habits

10
Question 1: Who is your average COPD patient? The Marlboro man The Marlboro man 55 year old working woman 55 year old working woman 85 yo man with ASCAD, and prostate cancer 85 yo man with ASCAD, and prostate cancer 80 yo retired Army thoracic surgeon 80 yo retired Army thoracic surgeon The Marlboro man The Marlboro man 55 year old working woman 55 year old working woman 85 yo man with ASCAD, and prostate cancer 85 yo man with ASCAD, and prostate cancer 80 yo retired Army thoracic surgeon 80 yo retired Army thoracic surgeon

11
Who does COPD Affect? Aunt Ann and my Dad.

12
Really?

13
My Aunt Carrie

14
Seriously?

15
It even looks like a fungus

16
COPD Definition and Epidemiology Risk Factors: cigarette smoking, Marijuana, alpha-1-antitrypsin deficiency, heavy occupational dusts, biomass fuels and chemical fumes, environmental tobacco smoke, lung growth (viral, fetal exposure) Risk Factors: cigarette smoking, Marijuana, alpha-1-antitrypsin deficiency, heavy occupational dusts, biomass fuels and chemical fumes, environmental tobacco smoke, lung growth (viral, fetal exposure) Caused by interaction of noxious inhaled agents and host factors increasing neutrophils and macrophages Caused by interaction of noxious inhaled agents and host factors increasing neutrophils and macrophages Toxic gases generate cytokines and chemokines control migration of inflammatory immune cells, leading to compromised repair of lung structure and function, increased apoptosis of endothelial and epithelial cells Toxic gases generate cytokines and chemokines control migration of inflammatory immune cells, leading to compromised repair of lung structure and function, increased apoptosis of endothelial and epithelial cells Risk Factors: cigarette smoking, Marijuana, alpha-1-antitrypsin deficiency, heavy occupational dusts, biomass fuels and chemical fumes, environmental tobacco smoke, lung growth (viral, fetal exposure) Risk Factors: cigarette smoking, Marijuana, alpha-1-antitrypsin deficiency, heavy occupational dusts, biomass fuels and chemical fumes, environmental tobacco smoke, lung growth (viral, fetal exposure) Caused by interaction of noxious inhaled agents and host factors increasing neutrophils and macrophages Caused by interaction of noxious inhaled agents and host factors increasing neutrophils and macrophages Toxic gases generate cytokines and chemokines control migration of inflammatory immune cells, leading to compromised repair of lung structure and function, increased apoptosis of endothelial and epithelial cells Toxic gases generate cytokines and chemokines control migration of inflammatory immune cells, leading to compromised repair of lung structure and function, increased apoptosis of endothelial and epithelial cells
 Risk Factors: cigarette smoking, Marijuana, alpha-1-antitrypsin deficiency, heavy occupational dusts, biomass fuels and chemical fumes, environmental tobacco smoke, lung growth (viral, fetal exposure) Caused by interaction of noxious inhaled agents and host factors increasing neutrophils and macrophages Caused by interaction of noxious inhaled agents and host factors increasing neutrophils and macrophages Toxic gases generate cytokines and chemokines control migration of inflammatory immune cells, leading to compromised repair of lung structure and function, increased apoptosis of endothelial and epithelial cells Toxic gases generate cytokines and chemokines control migration of inflammatory immune cells, leading to compromised repair of lung structure and function, increased apoptosis of endothelial and epithelial cells Risk Factors: cigarette smoking, Marijuana, alpha-1-antitrypsin deficiency, heavy occupational dusts, biomass fuels and chemical fumes, environmental tobacco smoke, lung growth (viral, fetal exposure) Risk Factors: cigarette smoking, Marijuana, alpha-1-antitrypsin deficiency, heavy occupational dusts, biomass fuels and chemical fumes, environmental tobacco smoke, lung growth (viral, fetal exposure) Caused by interaction of noxious inhaled agents and host factors increasing neutrophils and macrophages Caused by interaction of noxious inhaled agents and host factors increasing neutrophils and macrophages Toxic gases generate cytokines and chemokines control migration of inflammatory immune cells, leading to compromised repair of lung structure and function, increased apoptosis of endothelial and epithelial cells Toxic gases generate cytokines and chemokines control migration of inflammatory immune cells, leading to compromised repair of lung structure and function, increased apoptosis of endothelial and epithelial cells")
17
* Years after 2000 include adults aged ≥ 25y only COPD Mortality Year Annual US Deaths Mannino DM, et al. MMWR Morb Mortal Wkly Rep. 2002;51(SS-6):1-16. Brown DW, et al. MMWR Weekly. 2008;57(45):1229-1232
:1-16. Brown DW, et al. MMWR Weekly. 2008;57(45):")
18
COPD Immunology Small airways: inflammatory cell infiltrate, remodeling thickens the airway and increases resistance to flow Small airways: inflammatory cell infiltrate, remodeling thickens the airway and increases resistance to flow Prominent inflammatory infiltrates in the alveolar walls, destruction of alveoli, and enlargement of air spaces Prominent inflammatory infiltrates in the alveolar walls, destruction of alveoli, and enlargement of air spaces Inflammation mediated by T-cells persists after smoking cessation Inflammation mediated by T-cells persists after smoking cessation Cigarette use increased oxidative stress Cigarette use increased oxidative stress Small airways: inflammatory cell infiltrate, remodeling thickens the airway and increases resistance to flow Small airways: inflammatory cell infiltrate, remodeling thickens the airway and increases resistance to flow Prominent inflammatory infiltrates in the alveolar walls, destruction of alveoli, and enlargement of air spaces Prominent inflammatory infiltrates in the alveolar walls, destruction of alveoli, and enlargement of air spaces Inflammation mediated by T-cells persists after smoking cessation Inflammation mediated by T-cells persists after smoking cessation Cigarette use increased oxidative stress Cigarette use increased oxidative stress

24
24 Tamagawa E et al. Chest. 2006;130:1631-1633. Lung Inflammation and Vascular Disease Effects of Lung Inflammation on Blood Vessels

26
Normal Lungs and Lungs With COPD

27
Manifestations of COPD Emphysema: pathologic diagnosis Hyperinflation Mucus hypersecretion (chronic bronchitis) Frequent exacerbations Severe hypoxemia Low BMI Skeletal muscle dysfunction Papaioannou AI, et al. Respir Med. 2009;103:650-660. Celli BR. Proc Am Thorac Soc. 2006;3:461-465.

28
Increased Risk for Cardiovascular Disease in COPD MI = myocardial infarction, CHF = congestive heart failure, CVD = cardiovascular disease; All between-group differences P < 0.05 – adjusted for CV risk Curkendall SM, et al. Ann Epidemiol. 2006;16:63-70. 21.1 11.2 5.6 31.3 9.6 70.4 22.8 11.7 6.4 3.2 9 7.9 54 11.2 0 10 20 30 40 50 60 70 80 ArrhythmiaAnginaAcute MICHFStrokeOther CVDCVD Hospitalization Percent of Subjects COPD (N = 11,493) Controls (N = 22,986) Retrospective study of Canadian databases Subjects age ≥ 40 years Diagnosed with COPD during 1997–2000 Received ≥ 2 Rx for dilators w/i 6 months
 Controls (N = 22,986) Retrospective study of Canadian databases Subjects age ≥ 40 years Diagnosed with COPD during 1997–2000 Received ≥ 2 Rx for dilators w/i 6 months.")
29
The Risk of Osteoporosis in Caucasians With Obstructive Airways Disease Sin DD, et al. Am J Med. 2003;114:10-14. P = 0.005 for trends 1.9 3.9 6.8 11 7.6 10.3 20.9 33 0 5 10 15 20 25 30 35 NoneMildModerateSevere Severity of Airflow Obstruction Percent of Subjects with Osteoporosis Men Women

30
Severe Obstructive Airway Disease Is Associated With Greater Risk of Fracture de Vries F, et al. Eur Respir J. 2005;25:879-884. 0.20.512.05.0 Hip fracture Osteoporotic fracture Vertebral fracture *Adjusted in patients with severe COPD for general risk factors, smoking status, duration of enrollment, and exposure to bronchodilators ICS - No ICS - Yes ICS - No ICS - Yes ICS - No ICS - Yes Odds Ratio*

31
Skeletal Muscle Dysfunction in COPD Low muscle mass Poor capillarity Low muscle oxidative enzyme activity Low fraction of type I fibers Muscle inflammation Corticosteroid myopathy Low levels of anabolic hormones Vasoregulatory abnormalities Low muscle mass Poor capillarity Low muscle oxidative enzyme activity Low fraction of type I fibers Muscle inflammation Corticosteroid myopathy Low levels of anabolic hormones Vasoregulatory abnormalities Lactate Increase During Exercise Maltais F, et al. Am J Respir Crit Care Med. 1996;153:288-293. VO 2 (L/min)
.")
32
Testosterone IGF-1 Insulin resistance Negative energy balance Hypoxemia Steroid treatment Muscle protein breakdown Muscle wasting and cachexia Inflammation Mechanisms of Muscle Wasting and Cachexia in COPD Balasubramanian VP, Varkey B. Curr Opin Pulm Med. 2006;12:106-112.

33
Proportion Surviving Months of Follow-up BMI (kg/m 2 ) ■ > 29 ● 24-29 ✴ 20-24 ▼ < 20 Low BMI Predicts Increased Mortality Cox proportional hazards model Low BMI was an independent predictor of increased mortality (P < 0.001) After stratification into BMI quintiles, the mortality risk was clearly increased below 25 kg/m 2 Schols AM, et al. Am J Respir Crit Care Med. 1998;157(6 Pt 1):1791-1797.
:")
34
Prevalence of Depression in COPD Overlap between symptoms of depression and COPD (fatigue, sleep, appetite) 1 Prevalence: 20%–60% 1,2 Impact 3 – Decreased functional performance – Lower QOL scores Inadequate recognition and treatment 1 Overlap between symptoms of depression and COPD (fatigue, sleep, appetite) 1 Prevalence: 20%–60% 1,2 Impact 3 – Decreased functional performance – Lower QOL scores Inadequate recognition and treatment 1 1.Kunik ME, et al. Chest. 2005;127:1205-1211. 2.Norwood R. Curr Opin Pulm Med. 2006;12:113-117. 3.Felker B, et al. Gen Hosp Psych. 2001;23:56-61.

35
Prognostic Impact of Pulmonary Hypertension Oswald-Mammosser M, et al. Chest. 1995;107:1193-1198. – – – mean PAP ≥ 25 mmHg –––– mean PAP < 25 mmHg mean PAP > 18 mmHg mean PAP 18 mmHg PAP: pulmonary artery pressure Years w/o Hospitalization for Exacerbation Kaplan-Meier Estimates Survival time, months Survival Rate

36
The Majority of Patients with COPD Are Among Working Age Population

37
Employees With COPD Incurred >4 Times Higher Total Mean Healthcare Costs

38
Patients with COPD often have Multiple Comorbid Conditions

39
Comorbid Conditions in Patients with COPD Are More Likely to be Treated Than COPD

40
Mortality Associated With COPD

41
COPD Management Prevent disease and progression Prevent disease and progression Relieve symptoms Relieve symptoms Improve exercise tolerance Improve exercise tolerance Improve health status Improve health status Prevent and treat complications Prevent and treat complications Treat exacerbations Treat exacerbations Reduce mortality Reduce mortality Prevent disease and progression Prevent disease and progression Relieve symptoms Relieve symptoms Improve exercise tolerance Improve exercise tolerance Improve health status Improve health status Prevent and treat complications Prevent and treat complications Treat exacerbations Treat exacerbations Reduce mortality Reduce mortality

42
The COPD Population Screener (COPD-PS) 1. During the past 4 weeks, how much of the time did you feel short of breath? 2. Do you ever cough up any “stuff”, such as mucus or phlegm? 4. Have you smoked at least 100 cigarettes in your ENTIRE LIFE? Yes A little of the time Some of the time Most of the time All of the time None of the time 0 1 220 Only with occasional colds or chest infections Yes, a few days a month Yes, most days a week No, never Yes, every day 0 1 1 2 0 DisagreeUnsure AgreeStrongly agree Strongly disagree 0 0 1 0 2 5. How old are you? Don’t know No 0 2 0 Age 35 to 49Age 50 to 59 Age 60 to 69Age 70 + 1 22 0 Martinez FJ, et al. COPD. 2008;5:85-95. 3. Please select the answer that best describes you in the past 12 months, I do less than I used to because of my breathing problems.

43
Screening for COPD with Spirometry? Lin K, et al. Ann Intern Med. 2008;148(7):535-543. Current status Underrecognized Spirometry screening Overdiagnosis (other causes of symptoms) Symptom screening Overdiagnosis (asymptomatic healthy) 1.Symptoms 2.Spirometry Appropriate diagnosis
: Current status Underrecognized Spirometry screening Overdiagnosis (other causes of symptoms) Symptom screening Overdiagnosis (asymptomatic healthy) 1.Symptoms 2.Spirometry Appropriate diagnosis.")
44
Global Strategy for Diagnosis, Management and Prevention of COPD Diagnosis and Assessment: Key Points A clinical diagnosis of COPD should be considered in any patient who has dyspnea, chronic cough or sputum production, and/or a history of exposure to risk factors for the disease. A clinical diagnosis of COPD should be considered in any patient who has dyspnea, chronic cough or sputum production, and/or a history of exposure to risk factors for the disease. Spirometry is required to make the diagnosis; the presence of a post-bronchodilator FEV 1 /FVC < 0.70 confirms the presence of persistent airflow limitation and thus of COPD. Spirometry is required to make the diagnosis; the presence of a post-bronchodilator FEV 1 /FVC < 0.70 confirms the presence of persistent airflow limitation and thus of COPD. A clinical diagnosis of COPD should be considered in any patient who has dyspnea, chronic cough or sputum production, and/or a history of exposure to risk factors for the disease. A clinical diagnosis of COPD should be considered in any patient who has dyspnea, chronic cough or sputum production, and/or a history of exposure to risk factors for the disease. Spirometry is required to make the diagnosis; the presence of a post-bronchodilator FEV 1 /FVC < 0.70 confirms the presence of persistent airflow limitation and thus of COPD. Spirometry is required to make the diagnosis; the presence of a post-bronchodilator FEV 1 /FVC < 0.70 confirms the presence of persistent airflow limitation and thus of COPD.

45
Need a Quality Test

46
Spirometry: Obstructive Disease Volume, liters Time, seconds 5 4 3 2 1 123456 FEV 1 = 1.8L FVC = 3.2L FEV 1 /FVC = 0.56 Normal Obstructive

47
Spirograms and Flow Volume Curves A- Restrictive B- Normal C- Obstructive

48
Flow volume loops: Normal vs. COPD

49
: Normal Flow volume loop vs. COPD

50
MILD COPD

51
Severe COPD

52
Global Strategy for Diagnosis, Management and Prevention of COPD Classification of Severity of Airflow Limitation in COPD* In patients with FEV 1 /FVC < 0.70: GOLD 1: Mild FEV 1 > 80% predicted GOLD 2: Moderate 50% < FEV 1 < 80% predicted GOLD 3: Severe 30% < FEV 1 < 50% predicted GOLD 4: Very Severe FEV 1 < 30% predicted *Based on Post-Bronchodilator FEV 1

53
Assess symptoms Assess degree of airflow limitation using spirometry Assess risk of exacerbations Assess comorbidities Assess symptoms Assess degree of airflow limitation using spirometry Assess risk of exacerbations Assess comorbidities Use history of exacerbations and spirometry. Two exacerbations or more within the last year or an FEV 1 < 50 % of predicted value are indicators of high risk Global Strategy for Diagnosis, Management and Prevention of COPD Assessment of COPD

54
Global Strategy for Diagnosis, Management and Prevention of COPD Assess Risk of Exacerbations To assess risk of exacerbations use history of exacerbations and spirometry: Two or more exacerbations within the last year or an FEV 1 < 50 % of predicted value are indicators of high risk. To assess risk of exacerbations use history of exacerbations and spirometry: Two or more exacerbations within the last year or an FEV 1 < 50 % of predicted value are indicators of high risk.

55
Global Strategy for Diagnosis, Management and Prevention of COPD Combined Assessment of COPD Assess symptoms Assess degree of airflow limitation using spirometry Assess risk of exacerbations Combine these assessments for the purpose of improving management of COPD Assess symptoms Assess degree of airflow limitation using spirometry Assess risk of exacerbations Combine these assessments for the purpose of improving management of COPD

56
Global Strategy for Diagnosis, Management and Prevention of COPD Combined Assessment of COPD Risk (GOLD Classification of Airflow Limitation) Risk (Exacerbation history) > 2 1 0 (C) (D) (A) (B) mMRC 0-1 CAT < 10 4 3 2 1 mMRC > 2 CAT > 10 Symptoms (mMRC or CAT score)
 Risk (Exacerbation history) > (C) (D) (A) (B) mMRC 0-1 CAT < mMRC > 2 CAT > 10 Symptoms (mMRC or CAT score)")
57
Global Strategy for Diagnosis, Management and Prevention of COPD Combined Assessment of COPD (C)(D) (A)(B) mMRC 0-1 CAT < 10 mMRC > 2 CAT > 10 Symptoms (mMRC or CAT score) If mMRC 0-1 or CAT < 10: Less Symptoms (A or C) If mMRC > 2 or CAT > 10: More Symptoms (B or D) Assess symptoms first
(D) (A)(B) mMRC 0-1 CAT < 10 mMRC > 2 CAT > 10 Symptoms (mMRC or CAT score) If mMRC 0-1 or CAT < 10: Less Symptoms (A or C) If mMRC > 2 or CAT > 10: More Symptoms (B or D) Assess symptoms first")
58
Global Strategy for Diagnosis, Management and Prevention of COPD Combined Assessment of COPD Risk (GOLD Classification of Airflow Limitation) Risk (Exacerbation history) > 2 1 0 (C)(D) (A)(B) mMRC 0-1 CAT < 10 4 3 2 1 mMRC > 2 CAT > 10 Symptoms (mMRC or CAT score) If GOLD 1 or 2 and only 0 or 1 exacerbations per year: Low Risk (A or B) If GOLD 3 or 4 or two or more exacerbations per year: High Risk (C or D) Assess risk of exacerbations next
 Risk (Exacerbation history) > (C)(D) (A)(B) mMRC 0-1 CAT < mMRC > 2 CAT > 10 Symptoms (mMRC or CAT score) If GOLD 1 or 2 and only 0 or 1 exacerbations per year: Low Risk (A or B) If GOLD 3 or 4 or two or more exacerbations per year: High Risk (C or D) Assess risk of exacerbations next")
59
Global Strategy for Diagnosis, Management and Prevention of COPD Combined Assessment of COPD Risk (GOLD Classification of Airflow Limitation) Risk (Exacerbation history) > 2 1 0 (C)(D) (A)(B) mMRC 0-1 CAT < 10 4 3 2 1 mMRC > 2 CAT > 10 Symptoms (mMRC or CAT score) Patient is now in one of four categories: A: Les symptoms, low risk B: More symtoms, low risk C: Less symptoms, high risk D: More Symtoms, high risk Use combined assessment
 Risk (Exacerbation history) > (C)(D) (A)(B) mMRC 0-1 CAT < mMRC > 2 CAT > 10 Symptoms (mMRC or CAT score) Patient is now in one of four categories: A: Les symptoms, low risk B: More symtoms, low risk C: Less symptoms, high risk D: More Symtoms, high risk Use combined assessment")
60
Patien t CharacteristicSpirometric Classification Exacerbations per year mMRCCAT A Low Risk Less Symptoms GOLD 1-2≤ 10-1< 10 B Low Risk More Symptoms GOLD 1-2≤ 1> 2> 2≥ 10 C High Risk Less Symptoms GOLD 3-4> 2> 20-1< 10 D High Risk More Symptoms GOLD 3-4> 2> 2> 2> 2 ≥ 10 Global Strategy for Diagnosis, Management and Prevention of COPD Combined Assessment of COPD When assessing risk, choose the highest risk according to GOLD grade or exacerbation history

61
COPD Risk: exacerbations, hospitalization, death

63
CAT Scores: impact and management < 10: low impact: smoking cessation, annual influenza vaccination, reduce exacerbation risk, therapy by clinical assessment < 10: low impact: smoking cessation, annual influenza vaccination, reduce exacerbation risk, therapy by clinical assessment 10-20: medium impact: add review maintenance therapy, refer pulmonary rehab, minimize exacerbation, review aggravating factors: smoking 10-20: medium impact: add review maintenance therapy, refer pulmonary rehab, minimize exacerbation, review aggravating factors: smoking < 10: low impact: smoking cessation, annual influenza vaccination, reduce exacerbation risk, therapy by clinical assessment < 10: low impact: smoking cessation, annual influenza vaccination, reduce exacerbation risk, therapy by clinical assessment 10-20: medium impact: add review maintenance therapy, refer pulmonary rehab, minimize exacerbation, review aggravating factors: smoking 10-20: medium impact: add review maintenance therapy, refer pulmonary rehab, minimize exacerbation, review aggravating factors: smoking

64
CAT Scores: impact and management 21-30:high impact: pt has significant room for improvement, consider referral to specialist, additional pharmacologic treatments 21-30:high impact: pt has significant room for improvement, consider referral to specialist, additional pharmacologic treatments >30: very high impact: same as high impact >30: very high impact: same as high impact 21-30:high impact: pt has significant room for improvement, consider referral to specialist, additional pharmacologic treatments 21-30:high impact: pt has significant room for improvement, consider referral to specialist, additional pharmacologic treatments >30: very high impact: same as high impact >30: very high impact: same as high impact

67
Exacerbations Can Increase Healthcare Burden Associated With COPD Exacerbations of COPD can have negative impacts on patient lung function, health-related quality of life, and socioeconomic costs Exacerbations of COPD can have negative impacts on patient lung function, health-related quality of life, and socioeconomic costs Lung function declined more rapidly in patients with frequent exacerbations Lung function declined more rapidly in patients with frequent exacerbations Direct medical costs for exacerbations associated with COPD remain at approximately $18 billion per year Direct medical costs for exacerbations associated with COPD remain at approximately $18 billion per year Exacerbations of COPD can have negative impacts on patient lung function, health-related quality of life, and socioeconomic costs Exacerbations of COPD can have negative impacts on patient lung function, health-related quality of life, and socioeconomic costs Lung function declined more rapidly in patients with frequent exacerbations Lung function declined more rapidly in patients with frequent exacerbations Direct medical costs for exacerbations associated with COPD remain at approximately $18 billion per year Direct medical costs for exacerbations associated with COPD remain at approximately $18 billion per year 1) The Global Initiative for Chronic Obstructive Lung Disease. GOLD Report—Global Strategy for the Diagnosis, Management, and Prevention of Chronic Obstructive Pulmonary Disease. Updated 2009.; 2) Donaldson GC, Seemungal TA, Bhowmik A, Wedzicha JA. Relationship between exacerbation frequency and lung function decline in chronic obstructive pulmonary disease. Thorax. 2002;57(10):847-852. ; 3)Anzueto A, Sethi S, Martinez FJ. Exacerbations of chronic obstructive pulmonary disease. Proc Am Thorac Soc. 2007;4(7):554-564.
 Donaldson GC, Seemungal TA, Bhowmik A, Wedzicha JA. Relationship between exacerbation frequency and lung function decline in chronic obstructive pulmonary disease. Thorax. 2002;57(10): ; 3)Anzueto A, Sethi S, Martinez FJ. Exacerbations of chronic obstructive pulmonary disease. Proc Am Thorac Soc. 2007;4(7):")
69
Communication Is Essential to Monitoring Exacerbations

70
Management of Exacerbations Associated With COPD The Global Initiative for Chronic Obstructive Lung Disease. GOLD Report—Global Strategy for the Diagnosis, Management, and Prevention of Chronic Obstructive Pulmonary Disease. Updated 2009.

71
Impact of COPD

72
The BODE Index 0 1 2 3 FEV 1 (% predicted) 65 50-6436-49 35 Distance walked in 6 min. (M) 350 250-349150-249 149 MMRC dyspnea scale0-1234 BMI> 21 21 Variable Points on BODE Index Celli BR, et al. N Engl J Med. 2004;350:1005-1012. BODE = body mass index, obstruction, dyspnea, and exercise capacity; MMRC = Modified Medical Research Council
 149 MMRC dyspnea scale BMI> 21 21 Variable Points on BODE Index Celli BR, et al. N Engl J Med. 2004;350: BODE = body mass index, obstruction, dyspnea, and exercise capacity; MMRC = Modified Medical Research Council.")
73
Survival in COPD FEV 1 StageBODE Months 1.0 0.8 0.6 0.4 0.2 0.0 04812162024283236404448520481216202428323640444852 Stage I (> 50%) predicted Stage II (36-50%) predicted Stage III ( 35%) predicted Quartile 1 (BODE 0-2) Quartile 2 (BODE 3-4) Quartile 3 (BODE 5-6) Quartile 4 (BODE 7-10) Probability of Survival P < 0.001 Celli BR, et al. N Engl J Med. 2004;350:1005-1012.

74
COPD DIFFERENTIAL Asthma Asthma Congestive heart failure Congestive heart failure Bronchiectasis Bronchiectasis Verklempt Verklempt Asthma Asthma Congestive heart failure Congestive heart failure Bronchiectasis Bronchiectasis Verklempt Verklempt

75
More Than 50% of Patients With COPD Were Misdiagnosed With Asthma Tinkelman DG, Price DB, Nordyke RJ, Halbert RJ. Misdiagnosis of COPD and asthma in primary care patients 40 years of age and over. J Asthma. 2006;43(1):75-80.
:")
76
Differential Diagnosis: COPD and Asthma

77
COPD Management Ongoing monitoring and assessment Ongoing monitoring and assessment Progressive disease Progressive disease Follow up spirometry Follow up spirometry Monitor pharmacotherapy: therapeutics, adherence, technique, effectiveness of controlling symptoms Monitor pharmacotherapy: therapeutics, adherence, technique, effectiveness of controlling symptoms Monitor exacerbation: frequency and severity Monitor exacerbation: frequency and severity Ongoing monitoring and assessment Ongoing monitoring and assessment Progressive disease Progressive disease Follow up spirometry Follow up spirometry Monitor pharmacotherapy: therapeutics, adherence, technique, effectiveness of controlling symptoms Monitor pharmacotherapy: therapeutics, adherence, technique, effectiveness of controlling symptoms Monitor exacerbation: frequency and severity Monitor exacerbation: frequency and severity

78
Question 2: If a patient stops smoking the lung function improves True True False False Maybe a little Maybe a little True True False False Maybe a little Maybe a little

79
Smoking Cessation Can Slow COPD Onset and Progression

80
Question 3: What 4 interventions improve survival in severe COPD? 1. Exercise, oxygen, beta agonists, nutrition 2. Exercise, oxygen, anticholinergics, nutrition 3. Exercise, oxygen, quitting smoking, inhalers 4. Exercise, oxygen, quitting smoking, nutrition 1. Exercise, oxygen, beta agonists, nutrition 2. Exercise, oxygen, anticholinergics, nutrition 3. Exercise, oxygen, quitting smoking, inhalers 4. Exercise, oxygen, quitting smoking, nutrition

81
Comprehensive Approach for COPD Management

82
Counseling Nicotine replacement – Gum – Inhaler – Nasal spray – Transdermal patch – Sublingual tablet – Lozenge Acidic Beverages (coffee) Bupropion Varenicline First Line Smoking Cessation Treatments GOLD Guidelines 2008. http://www.goldcopd.com/Guidelineitem.asp?l1=2&l2=1&intId=2003. Accessed September 2010.

83
Carbon Monoxide-Confirmed 4-Week Continuous Quit Rates Weeks 9–12 OR = 3.85 * OR = 1.93 * OR = 3.85 * OR = 1.90 * 100 44.0 43.9 29.8 29.5 17.617.7 0 20 40 60 Study IStudy II Response Rate (%) VareniclineBupropionPlacebo N = 352N = 329N = 344 N = 342N = 341 OR = odds ratio * P < 0.001 Gonzales D, et al. JAMA. 2006;296:47-55. Jorenby DE, et al. JAMA. 2006;296:56-63.

84
Smoking Cessation with Varenicline Tx Period Tashkin DP, et al. Chest. 2010 Sep 23. [Epub ahead of print] 1 o Endpoint

85
Adverse EventVarenicline 0.5 mg BID n = 129 Varenicline 1 mg BID n = 821 Placebo n = 805 Nausea16%30%10% Insomnia*19%18%13% Abnormal Dreams 9%13%5% Constipation5%8%3% Flatulence9%6%3% Vomiting1%5%2% Varenicline: Most Common Adverse Events From 12-week Fixed-Dose, Placebo-Controlled Studies * Includes Preferred Terms: Insomnia/Initial insomnia/Middle insomnia/Early morning awakening* Varenicline package insert. Available at: www.pfizer.com/files/products/uspi_chantix.pdf. Accessed September 2010.

86
Psychiatric symptoms – Changes in behavior – Agitation – Depressed mood – Suicidal ideation – Suicidal behavior “Advise patients and caregivers that the patient should stop taking CHANTIX (varenicline) and contact a health care provider immediately if agitation, depressed mood, or changes in behavior that are not typical for the patient are observed, or if the patient develops suicidal ideation or suicidal behavior.” Varenicline Warning Varenicline package insert. http://www.pfizer.com/files/products/uspi_chantix.pdf. Accessed September 2010.

87
Nicotine Nasal Spray with Nicotine Patch for Smoking Cessation Percentage (number) of participants abstinent from smoking at follow up 237 smokers followed for 6 years Combination of a 5 month nicotine patch + nicotine nasal spray is more effective for smoking cessation than the patch alone Blondal T, et al. BMJ. 1999;318:285-288.

88
At every encounter, ask patient if he/she is still smoking, and chart response At every encounter, give strong advice to quit smoking Measure expired CO (> 10 ppm) Perform/order spirometry, use spirometry results and ‘lung age’ as leverage to advise smoking cessation Ask patient if they are ready to quit and their history of attempts Negotiate/impose a target ‘Quit Day’, have staff follow up that day –Schedule follow-up appointments Refer patient to a behavioral support program or telephone quit line Prescribe pharmacological support as appropriate –NRT, bupropion SR, varenicline Tips to Help Patients Quit Smoking Adapted from Tashkin DP, and Murray RP. Respir Med. 2009;103:963-974.

89
Short acting bronchodilators: Short acting bronchodilators: B2 adrenergic agonist: albuterol, levalbuterol B2 adrenergic agonist: albuterol, levalbuterol Anticholinergic agent: ipratropium Anticholinergic agent: ipratropium Combination: albuterol/ipratropium Combination: albuterol/ipratropium Long acting bronchodilators B2 adrenergic agonists: salmeterol, formoterol, B2 adrenergic agonists: salmeterol, formoterol, aformoterol, Indacaterol Anticholinergic: tiotropium bromide, Aclidinium Inhaled corticosteroids: fluticasone, budesonide, beclomethasone, mometasone Combinations: fluticasone-salmeterol, budesonide- formoterol, mometasone-fomoterol Methylxanthines: theophylline PDE4 Inhibitor: Roflumilast Antibiotics: Azithromycin

90
Rescue vs Maintenance Medication in Moderate COPD

91
COPD Management: Pharmacologic Theophylline Theophylline: Thoracic Park Theophylline: Thoracic Park Smooth muscle relaxation Smooth muscle relaxation Fall in trapped gas volume Fall in trapped gas volume Pulmonary vascular dilator Pulmonary vascular dilator Level 6-10 Level 6-10 Studies: 110 patients 100mg bid over 1 year, favorable, decreased exacerbations, decreased clinic visits, increased FEV1 Studies: 110 patients 100mg bid over 1 year, favorable, decreased exacerbations, decreased clinic visits, increased FEV1 42 Theophylline and 43 placebo 42 Theophylline and 43 placebo Theophylline: Thoracic Park Theophylline: Thoracic Park Smooth muscle relaxation Smooth muscle relaxation Fall in trapped gas volume Fall in trapped gas volume Pulmonary vascular dilator Pulmonary vascular dilator Level 6-10 Level 6-10 Studies: 110 patients 100mg bid over 1 year, favorable, decreased exacerbations, decreased clinic visits, increased FEV1 Studies: 110 patients 100mg bid over 1 year, favorable, decreased exacerbations, decreased clinic visits, increased FEV1 42 Theophylline and 43 placebo 42 Theophylline and 43 placebo

92
COPD Management:Pharmacologic Theophylline May act as nonselective phosphodiesterase inhibitors May act as nonselective phosphodiesterase inhibitors Significance is disputed Significance is disputed Clearance of the drug decreases with age Clearance of the drug decreases with age All studies were performed with slow release preparations All studies were performed with slow release preparations There is evidence to show greater improvement in FEV1 when added to salmeterol than salmeterol alone There is evidence to show greater improvement in FEV1 when added to salmeterol than salmeterol alone Toxicity: arrythmias, nausea, vomiting, seizure, GERD, plus multiple drug interactions Toxicity: arrythmias, nausea, vomiting, seizure, GERD, plus multiple drug interactions May act as nonselective phosphodiesterase inhibitors May act as nonselective phosphodiesterase inhibitors Significance is disputed Significance is disputed Clearance of the drug decreases with age Clearance of the drug decreases with age All studies were performed with slow release preparations All studies were performed with slow release preparations There is evidence to show greater improvement in FEV1 when added to salmeterol than salmeterol alone There is evidence to show greater improvement in FEV1 when added to salmeterol than salmeterol alone Toxicity: arrythmias, nausea, vomiting, seizure, GERD, plus multiple drug interactions Toxicity: arrythmias, nausea, vomiting, seizure, GERD, plus multiple drug interactions

94
PDE4 Inhibitor Roflumilast Study Design Anti-inflammatory action Previously shown to improve lung function but not exacerbations Assess exacerbations in carefully selected patients Patients: confirmed COPD Severe airflow limitation (FEV 1 /FVC ≤ 70%) Bronchitic symptoms History of exacerbations Current or former smokers (≥ 20 pack-year history) > 40 years old 2 parallel identical studies Anti-inflammatory action Previously shown to improve lung function but not exacerbations Assess exacerbations in carefully selected patients Patients: confirmed COPD Severe airflow limitation (FEV 1 /FVC ≤ 70%) Bronchitic symptoms History of exacerbations Current or former smokers (≥ 20 pack-year history) > 40 years old 2 parallel identical studies Calverley PM, et al. Lancet. 2009;374(9691):685-694.
:")
95
PDE4 Inhibitor Roflumilast 4 week run-in with placebo Randomization (Study M2-124 n = 1525; M2-125 n = 1571) Roflumilast 500 mcg qd Placebo 52 weeks of treatment Permitted co-medications LABA SABA Continuing short- or long-acting anticholinergics Forbidden co-medications Inhaled CS New long-acting anticholinergics 1 o endpoints Change in pre-bronchodilator FEV 1 Rate of COPD exacerbations NO NOT GIVE IN COMBINATION with Theophylline 4 week run-in with placebo Randomization (Study M2-124 n = 1525; M2-125 n = 1571) Roflumilast 500 mcg qd Placebo 52 weeks of treatment Permitted co-medications LABA SABA Continuing short- or long-acting anticholinergics Forbidden co-medications Inhaled CS New long-acting anticholinergics 1 o endpoints Change in pre-bronchodilator FEV 1 Rate of COPD exacerbations NO NOT GIVE IN COMBINATION with Theophylline Calverley PM, et al. Lancet. 2009;374(9691):685-694.
:")
96
PDE4 Inhibitor Roflumilast Results Calverley PM, et al. Lancet. 2009;374(9691):685-694. M2-124M2-125Pooled RofPboΔPRofPboΔPRofPboΔP Δ pre-dilator FEV 1 (mL) 468390.000333-2558< 0.000140-948< 0.0001 RR Mean exac rate (per pt*yr) 1.081.270.850.0281.211.490.820.0041.141.37 0.0003 Study confirms efficacy in selected patients with COPD No roflumilast effect on mortality or CRP levels Diarrhea, nausea, weight loss more common with roflumilast
: M2-124M2-125Pooled RofPboΔPRofPboΔPRofPboΔP Δ pre-dilator FEV 1 (mL) < < RR Mean exac rate (per pt*yr) Study confirms efficacy in selected patients with COPD No roflumilast effect on mortality or CRP levels Diarrhea, nausea, weight loss more common with roflumilast.")
97
COPD Management: Pharmacologic Beta Agonists Sympathomimetics: Albuterol, Salbutamol, Levalbuterol, Salmeterol, Formoterol, Indacaterol Sympathomimetics: Albuterol, Salbutamol, Levalbuterol, Salmeterol, Formoterol, Indacaterol B2: bronchial smooth muscle: small and medium airways, stimulate beta2 adrenergic receptors B2: bronchial smooth muscle: small and medium airways, stimulate beta2 adrenergic receptors Improve mucocilliary clearance Improve mucocilliary clearance Increased response in combination therapy Increased response in combination therapy Cardiovascular effects, hypokalemia, tachyphylaxis, lactic acidosis and respiratory failure Cardiovascular effects, hypokalemia, tachyphylaxis, lactic acidosis and respiratory failure Dose: technique, spacer Dose: technique, spacer Sympathomimetics: Albuterol, Salbutamol, Levalbuterol, Salmeterol, Formoterol, Indacaterol Sympathomimetics: Albuterol, Salbutamol, Levalbuterol, Salmeterol, Formoterol, Indacaterol B2: bronchial smooth muscle: small and medium airways, stimulate beta2 adrenergic receptors B2: bronchial smooth muscle: small and medium airways, stimulate beta2 adrenergic receptors Improve mucocilliary clearance Improve mucocilliary clearance Increased response in combination therapy Increased response in combination therapy Cardiovascular effects, hypokalemia, tachyphylaxis, lactic acidosis and respiratory failure Cardiovascular effects, hypokalemia, tachyphylaxis, lactic acidosis and respiratory failure Dose: technique, spacer Dose: technique, spacer

98
COPD Management: Pharmacologic Beta Agonists SABA: takes effect in 15-20 minutes and lasts 4 hours SABA: takes effect in 15-20 minutes and lasts 4 hours LABA: LABA: Salmeterol: takes effect in 4 hours and lasts 12 hours Salmeterol: takes effect in 4 hours and lasts 12 hours Fomoterol: takes effect in 1 hour and lasts 12hours Fomoterol: takes effect in 1 hour and lasts 12hours Indacaterol: takes effect in 1 hout and lasts 24 hours Indacaterol: takes effect in 1 hout and lasts 24 hours All significantly improve lung volumes, dyspnea, health related quality of life, and exacerbation rate All significantly improve lung volumes, dyspnea, health related quality of life, and exacerbation rate Aformoterol nebulized lasts 12 hours Aformoterol nebulized lasts 12 hours SABA: takes effect in 15-20 minutes and lasts 4 hours SABA: takes effect in 15-20 minutes and lasts 4 hours LABA: LABA: Salmeterol: takes effect in 4 hours and lasts 12 hours Salmeterol: takes effect in 4 hours and lasts 12 hours Fomoterol: takes effect in 1 hour and lasts 12hours Fomoterol: takes effect in 1 hour and lasts 12hours Indacaterol: takes effect in 1 hout and lasts 24 hours Indacaterol: takes effect in 1 hout and lasts 24 hours All significantly improve lung volumes, dyspnea, health related quality of life, and exacerbation rate All significantly improve lung volumes, dyspnea, health related quality of life, and exacerbation rate Aformoterol nebulized lasts 12 hours Aformoterol nebulized lasts 12 hours

99
COPD Management: Pharmacologic Anticholinergics Anticholinergics Muscarinic receptors Muscarinic receptors Airway smooth muscle: M3 Airway smooth muscle: M3 Chronic bronchitis and emphysema 2x -4x increased cholinergic tone Chronic bronchitis and emphysema 2x -4x increased cholinergic tone Atropine 1920’s, Ipratropium bromide 1980’s, Tiotropium 2004- proximal bronchiole and bronchi, Aclidinium 2012 Atropine 1920’s, Ipratropium bromide 1980’s, Tiotropium 2004- proximal bronchiole and bronchi, Aclidinium 2012 Anticholinergics Anticholinergics Muscarinic receptors Muscarinic receptors Airway smooth muscle: M3 Airway smooth muscle: M3 Chronic bronchitis and emphysema 2x -4x increased cholinergic tone Chronic bronchitis and emphysema 2x -4x increased cholinergic tone Atropine 1920’s, Ipratropium bromide 1980’s, Tiotropium 2004- proximal bronchiole and bronchi, Aclidinium 2012 Atropine 1920’s, Ipratropium bromide 1980’s, Tiotropium 2004- proximal bronchiole and bronchi, Aclidinium 2012

100
Expiratory Airflow Limitation Leads to Air Trapping

101
Airflow Limitation Leads to Air Trapping and Hyperinflation Airflow Limitation Leads to Air Trapping and Hyperinflation

102
Hyperinflation

103
COPD Management: Pharmacologic Ipratropium Dosing: 4 puffs Q6 hours Ipratropium Dosing: 4 puffs Q6 hours Combivent 1990’s: Albuterol + Ipratropium Combivent 1990’s: Albuterol + Ipratropium FEV1 increased 31-33% over baseline FEV1 increased 31-33% over baseline Fewer exacerbations Fewer exacerbations Tiotropium Bromide- once daily long acting bronchodilator Tiotropium Bromide- once daily long acting bronchodilator Long acting antimuscarinic agent, M3 receptors, effect one hour and lasts 24 hours Long acting antimuscarinic agent, M3 receptors, effect one hour and lasts 24 hours Ipratropium Dosing: 4 puffs Q6 hours Ipratropium Dosing: 4 puffs Q6 hours Combivent 1990’s: Albuterol + Ipratropium Combivent 1990’s: Albuterol + Ipratropium FEV1 increased 31-33% over baseline FEV1 increased 31-33% over baseline Fewer exacerbations Fewer exacerbations Tiotropium Bromide- once daily long acting bronchodilator Tiotropium Bromide- once daily long acting bronchodilator Long acting antimuscarinic agent, M3 receptors, effect one hour and lasts 24 hours Long acting antimuscarinic agent, M3 receptors, effect one hour and lasts 24 hours

104
COPD Management: Pharmacologic Minimal side effects: dry mouth, exacerbation glaucoma and constipation Minimal side effects: dry mouth, exacerbation glaucoma and constipation Very safe Very safe Poorly absorbed Poorly absorbed Minimal side effects: dry mouth, exacerbation glaucoma and constipation Minimal side effects: dry mouth, exacerbation glaucoma and constipation Very safe Very safe Poorly absorbed Poorly absorbed

105
Donahue et al: Indacaterol vs. Tiotropium Evaluated Indacaterol vs. placebo and placebo and Tiotropium over 26 weeks Evaluated Indacaterol vs. placebo and placebo and Tiotropium over 26 weeks 1,683 patients, Moderate to severe COPD, Indacaterol 150 mcg or 300 mcg 1,683 patients, Moderate to severe COPD, Indacaterol 150 mcg or 300 mcg SGRQ, FEV1, and exacerbations SGRQ, FEV1, and exacerbations post dose trough FEV1 increased 180 ml with Indacaterol and 140 ml with Tiotropium post dose trough FEV1 increased 180 ml with Indacaterol and 140 ml with Tiotropium SGRQ improved but not statistically significant, no improvement in decreased exacerbations SGRQ improved but not statistically significant, no improvement in decreased exacerbations Evaluated Indacaterol vs. placebo and placebo and Tiotropium over 26 weeks Evaluated Indacaterol vs. placebo and placebo and Tiotropium over 26 weeks 1,683 patients, Moderate to severe COPD, Indacaterol 150 mcg or 300 mcg 1,683 patients, Moderate to severe COPD, Indacaterol 150 mcg or 300 mcg SGRQ, FEV1, and exacerbations SGRQ, FEV1, and exacerbations post dose trough FEV1 increased 180 ml with Indacaterol and 140 ml with Tiotropium post dose trough FEV1 increased 180 ml with Indacaterol and 140 ml with Tiotropium SGRQ improved but not statistically significant, no improvement in decreased exacerbations SGRQ improved but not statistically significant, no improvement in decreased exacerbations

106
UPLIFT Trial Time to first exacerbation: Tiotropium 16.5 months vs placebo 12.5 months 14% reduction in # exacerbations Tiotropium Mortality not statically significant 14.4% vs 16.3% Time to first exacerbation: Tiotropium 16.5 months vs placebo 12.5 months 14% reduction in # exacerbations Tiotropium Mortality not statically significant 14.4% vs 16.3%

107
Clinical Course of COPD Air Trapping Expiratory Flow Limitation Breathlessness Inactivity Poor Health-Related Quality of Life Hyperinflation Deconditioning COPD DisabilityDisease progressionDeath Reduced Exercise Capacity COPD Exacerbations Adapted from Decramer M. Eur Respir Rev. 2006;15:51-57.

108
Question 5: what happens to your end expiratory lung volume with exercise? A- increases B- decreases

109
Totallungcapacity Tidal volume Inspiratory reserve volume Expiratory reserve volume Residual volume Inspiratory Inspiratorycapacity Vital Vitalcapacity Functional residual capacity Lung Volume Terminology

110
FRC TV IC RV Normal Rest Static and Dynamic Lung Volumes in COPDExercise RestCOPDExercise

111
Lung Volume Response to Exercise

112
Lung volume (L) Exercise time (minutes) EELV TLC VTVT IRV Placebo IC (1.92 L) Operating Lung Volumes & Exercise Endurance Maltais et al EELV TLC VTVT IRV IC (1.78 L) Tiotropium
 Exercise time (minutes) EELV TLC VTVT IRV Placebo IC (1.92 L) Operating Lung Volumes & Exercise Endurance Maltais et al EELV TLC VTVT IRV IC (1.78 L) Tiotropium")
113
Management: Aclidinium bromide Long term management of COPD, chronic bronchitis, emphysema LAMA, twice a day, muscarinic receptor M3 receptors Long term management of COPD, chronic bronchitis, emphysema LAMA, twice a day, muscarinic receptor M3 receptors

114
Management: Aclidinium Bromide Potential side effects: narrow angle glaucoma, urinary retention, cough, hypersensitivity to milk protein Peak FEV1 improvements: 200mcg 235 ml and 400mcg 264ml Trough FEV1 improvements: 200 mg 44 ml and 400mcg 109 ml Sustained over 52 weeks Potential side effects: narrow angle glaucoma, urinary retention, cough, hypersensitivity to milk protein Peak FEV1 improvements: 200mcg 235 ml and 400mcg 264ml Trough FEV1 improvements: 200 mg 44 ml and 400mcg 109 ml Sustained over 52 weeks

115
COPD Management: Pharmacologic Steroids: acute exacerbation of COPD favorable results and substantial benefits Improvement in wheezing, air flow Improvement in abnormal mucus Trial for 2-3 weeks Demonstrate 20-30% improvement FEV1 Response to oral steroids poor predictor respond to inhaled steroids Steroids: acute exacerbation of COPD favorable results and substantial benefits Improvement in wheezing, air flow Improvement in abnormal mucus Trial for 2-3 weeks Demonstrate 20-30% improvement FEV1 Response to oral steroids poor predictor respond to inhaled steroids

116
COPD Management: Pharmacologic Four large studies regular treatment with inhaled glucocorticosteroids appropriate for symptomatic COPD patients FEV1< 50% predicted Treatment reduce frequency of exacerbations and improve health status Benefit 25-50% of patients: improvement 6 minute walk Four large studies regular treatment with inhaled glucocorticosteroids appropriate for symptomatic COPD patients FEV1< 50% predicted Treatment reduce frequency of exacerbations and improve health status Benefit 25-50% of patients: improvement 6 minute walk

117
TRIPLE THERAPY Welte et al.:Efficacy and Tolerability of Budesonide/Formoterol Added to Tiotropium in Patients with Chronic Obstructive Pulmonary Disease To assess the efficacy and tolerability of budesonide/formoterol added to tiotropium in patients eligible for inhaled corticosteroid/long-acting β2-agonist combination therapy. Welte et al.:Efficacy and Tolerability of Budesonide/Formoterol Added to Tiotropium in Patients with Chronic Obstructive Pulmonary Disease To assess the efficacy and tolerability of budesonide/formoterol added to tiotropium in patients eligible for inhaled corticosteroid/long-acting β2-agonist combination therapy.

118
Triple Therapy Over the treatment period, budesonide/formoterol plus tiotropium significantly increased predose FEV1 by 6% (65 ml) and postdose by 11% (123 and 131 ml at 5 and 60 min postdose, respectively) versus tiotropium alone (both P < 0.001). The number of severe exacerbations decreased by 62%. Both treatments were well tolerated.

119
FEV 1 With Triple Combination Therapy 1. Aaron SD, et al. Ann Intern Med. 2007;146(8):545-555. 2. Welte T, et al. Am J Respir Crit Care Med. 2009;180(8):741-750. ● BUD/FORM + TIO ■ PBO + TIO Tio +/- Fluc/Sal 1 Tio +/- Bud/Form 2
: Welte T, et al. Am J Respir Crit Care Med. 2009;180(8): ● BUD/FORM + TIO ■ PBO + TIO Tio +/- Fluc/Sal 1 Tio +/- Bud/Form 2.")
120
Exacerbations With Triple Combination Therapy Tiotropium (n = 156) Tiotropium + Salmeterol (n = 148) Tiotropium + Salmeterol + Fluticasone (n = 145) % Pts with ≥ 1 exacerbations 62.8 %64.8%60.0% Total Exacerbations222226188 Exacerbations with Hospitalization Incidence rate ratio compared with tiotropium + placebo (95% CI) 4938 0.83 (0.54 to 1.27) 26 0.53 (0.33 to 0.86) Aaron SD, et al. Ann Int Med. 2007;146(8):545-555.
:")
121
COPD Management: Pharmacologic Side effects : well recognized with steroids Inhaled steroids: oral thrush, hoarseness, bruising Increased pneumonia with fluticasone/salmeterol (TORCH trial) Triamcinolone increased risk of bone fracture Budesonide least absorbed, no effect on bone mineral density Fluticosone/salmeterol; mometasone/formoterol; budesonide/formoterol Side effects : well recognized with steroids Inhaled steroids: oral thrush, hoarseness, bruising Increased pneumonia with fluticasone/salmeterol (TORCH trial) Triamcinolone increased risk of bone fracture Budesonide least absorbed, no effect on bone mineral density Fluticosone/salmeterol; mometasone/formoterol; budesonide/formoterol
 Triamcinolone increased risk of bone fracture Budesonide least absorbed, no effect on bone mineral density Fluticosone/salmeterol; mometasone/formoterol; budesonide/formoterol Side effects : well recognized with steroids Inhaled steroids: oral thrush, hoarseness, bruising Increased pneumonia with fluticasone/salmeterol (TORCH trial) Triamcinolone increased risk of bone fracture Budesonide least absorbed, no effect on bone mineral density Fluticosone/salmeterol; mometasone/formoterol; budesonide/formoterol")
122
COPD Management: Pharmacologic Vaccines: influenza reduce the serious illness and death in COPD by 50% Pneumococcal vaccine: 65 and older, younger patients with COPD FEV1< 40%, reduction pneumonia Alpha-1-antitrypsin augmentation therapy Smoking cessation: Varenicline, nicotine acetycholine receptor agonist Mucolytics: controvertial, some evidence in pts not on inhaled steroids N-acetylcyseine or carbocysteine may reduce exacerbations Vaccines: influenza reduce the serious illness and death in COPD by 50% Pneumococcal vaccine: 65 and older, younger patients with COPD FEV1< 40%, reduction pneumonia Alpha-1-antitrypsin augmentation therapy Smoking cessation: Varenicline, nicotine acetycholine receptor agonist Mucolytics: controvertial, some evidence in pts not on inhaled steroids N-acetylcyseine or carbocysteine may reduce exacerbations

123
Management Azithromycin: macrolide antibiotics have immunomodulatory and anti-bacterial properties 1142 COPD patients: randomized placebo to Azithromycin 250 mg daily Azithromycin increased time to first exacerbation from 174 days to 266 days 37% decrease exacerbation rate Azithromycin: macrolide antibiotics have immunomodulatory and anti-bacterial properties 1142 COPD patients: randomized placebo to Azithromycin 250 mg daily Azithromycin increased time to first exacerbation from 174 days to 266 days 37% decrease exacerbation rate

124
Effects best in patients with more moderate GOLD II disease and former smokers Increased hearing decrement 25% vs 20% 1 yr, no guidance for long term efficacy or potential adverse effects of resistance Patients with tachycardia and prolonged QT excluded Management: Azithromycin

125
COPD mortality is increasing Exacerbations are an important risk factor for mortality Treatment with current drugs and combinations can reduce exacerbations Currently available drugs alone and in combination have been shown to have beneficial impacts on lung function and patient-centered outcomes in COPD and are useful in managing COPD. No pharmacologic agent has thus far been shown to modify the persistence or progression of the underlying inflammatory/profibrotic/elastolytic pathology in COPD COPD mortality is increasing Exacerbations are an important risk factor for mortality Treatment with current drugs and combinations can reduce exacerbations Currently available drugs alone and in combination have been shown to have beneficial impacts on lung function and patient-centered outcomes in COPD and are useful in managing COPD. No pharmacologic agent has thus far been shown to modify the persistence or progression of the underlying inflammatory/profibrotic/elastolytic pathology in COPD Implications of Recent Trial Results

126
COPD Management: Oxygen 1895: commercially produced liquid air 1920: hypoxia and right heart failure 1956: improves exercise capacity 1967: low flow O2 1968: improvement function in patients receiving ambulatory O2 1970: long term home O2 increase survival 1980: O2 conserving device 1895: commercially produced liquid air 1920: hypoxia and right heart failure 1956: improves exercise capacity 1967: low flow O2 1968: improvement function in patients receiving ambulatory O2 1970: long term home O2 increase survival 1980: O2 conserving device

127
COPD Management: Oxygen Mortality reduced in patients with RA PaO2 < 56 mmHg or O2 saturation < 88% RA PaO2 < 60 mmHg with erythrocytosis, mental dysfunction, CHF, or cor pulmonale Need therapy for 18-24 hours Mortality reduced in patients with RA PaO2 < 56 mmHg or O2 saturation < 88% RA PaO2 < 60 mmHg with erythrocytosis, mental dysfunction, CHF, or cor pulmonale Need therapy for 18-24 hours

128
COPD Management: Oxygen Improves quality of life, decreased hospitalization, improved psychomotor performance Improves quality of life, decreased hospitalization, improved psychomotor performance Decreases pulmonary artery pressure Decreases pulmonary artery pressure Improves quality of life, decreased hospitalization, improved psychomotor performance Improves quality of life, decreased hospitalization, improved psychomotor performance Decreases pulmonary artery pressure Decreases pulmonary artery pressure

129
Improved COPD Survival on LTOT Güell Rous R. Int J Chron Obstruct Pulmon Dis. 2008;3(2):231-237. Nocturnal Oxygen Therapy Trial Group. Ann Intern Med. 1980;93:391-398. Medical Research Council Working Party. Lancet 1981;1:681-686.
: Nocturnal Oxygen Therapy Trial Group. Ann Intern Med. 1980;93: Medical Research Council Working Party. Lancet 1981;1:")
130
COPD Management: Pulmonary Rehab Reduces symptoms, improve quality of life, increased physical and emotional participation in life activities Covers non pulmonary issues Respiratory muscles abnormal: inactivity, systemic inflammation, malnutrition, increased work of breathing, impaired oxygen delivery, co morbid states, electrolyte imbalance, and drugs Reduces symptoms, improve quality of life, increased physical and emotional participation in life activities Covers non pulmonary issues Respiratory muscles abnormal: inactivity, systemic inflammation, malnutrition, increased work of breathing, impaired oxygen delivery, co morbid states, electrolyte imbalance, and drugs

131
COPD Management: Pulmonary Rehab Involve several health professionals Comprehensive exercise training Nutrition counseling Education Involve several health professionals Comprehensive exercise training Nutrition counseling Education

132
Efficacy of Pulmonary Rehabilitation Griffiths TL, et al. Lancet. 2000;355:362-368. Walking Distance Dyspnea Patients participated in 3 half day sessions per week for 6 weeks in a multidisciplinary rehabilitation program including smoking cessation, occupational, physical, breathing, and diet sessions Physical therapy included 30 min sessions in-office as well as home sessions –Treadmills, cycling, circuit training P = 0.000 P = 0.017 P = 0.000 P = 0.002

133
COPD Management: Pulmonary Rehab 80 patients at LLUMC reduction from 19 to 6 days of hospitalization Less time in hospital, fewer ER and office visits, return to work, increased ADL’s, more self care, decreased extended care and home care Improved dyspnea and cough 80 patients at LLUMC reduction from 19 to 6 days of hospitalization Less time in hospital, fewer ER and office visits, return to work, increased ADL’s, more self care, decreased extended care and home care Improved dyspnea and cough

134
COPD Management: Nutrition

135
Nutritional Supplements Have Not Increased Weight of Patients Study DeLetter 1991 Knowles 1988 Otte 1989 Rogers 1992 Schols 1995 Schols 1995a Steiner 2003 Weekes 2004 18 13 15 39 33 25 30 N 17 12 15 12 25 38 35 25 N Nutritional supplementation versus placebo or usual diet Adapted from Ferreira IM, et al. Cochrane Database Syst Rev. 2009;(2):CD000998. Standardized Mean Difference (Random) 9.2 7.2 8.1 7.8 12.9 13.9 12.6 11.9 Weight % 95% CI Total 214205100.0 Test for overall effect Z = 1.25 P = 0.21 -4.0-2.04.02.00 Control betterSupplement better
:CD Standardized Mean Difference (Random) Weight % 95% CI Total Test for overall effect Z = 1.25 P = Control betterSupplement better.")
136
LVRS: resection of functionless areas of emphysematous lung to improve mechanics FEV1< 20% and either homogenous emphysema or DLCO < 20% high risk for death or unlikely to benefit Increases exercise capacity not confer survival advantage LVRS: resection of functionless areas of emphysematous lung to improve mechanics FEV1< 20% and either homogenous emphysema or DLCO < 20% high risk for death or unlikely to benefit Increases exercise capacity not confer survival advantage COPD Management: Surgery

137
Yield advantage for patients both predominantly upper lobe emphysema and low baseline exercise capacity Range of FEV1 improvement 250-350 ml Improved 6 minute walk $140,000 per quality-adjusted life year Resection of large bullae > 1/3 hemithorax Lung transplant Yield advantage for patients both predominantly upper lobe emphysema and low baseline exercise capacity Range of FEV1 improvement 250-350 ml Improved 6 minute walk $140,000 per quality-adjusted life year Resection of large bullae > 1/3 hemithorax Lung transplant COPD Management: Surgery

138
Global Strategy for Diagnosis, Management and Prevention of COPD Manage Stable COPD: Non-pharmacologic PatientEssentialRecommendedDepending on local guidelines A Smoking cessation (can include pharmacologic treatment) Physical activity Flu vaccination Pneumococcal vaccination B, C, D Smoking cessation (can include pharmacologic treatment) Pulmonary rehabilitation Physical activity Flu vaccination Pneumococcal vaccination
 Physical activity Flu vaccination Pneumococcal vaccination B, C, D Smoking cessation (can include pharmacologic treatment) Pulmonary rehabilitation Physical activity Flu vaccination Pneumococcal vaccination")
139
Global Strategy for Diagnosis, Management and Prevention of COPD Manage Stable COPD: Pharmacologic Therapy ( Medications in each box are mentioned in alphabetical order, and therefore not necessarily in order of preference.) PatientFirst choiceSecond choiceAlternative Choices A SAMA prn or SABA prn LAMA or LABA or SABA and SAMA Theophylline B LAMA or LABA LAMA and LABA SABA and/or SAMA Theophylline C ICS + LABA or LAMA LAMA and LABA PDE4-inh. SABA and/or SAMA Theophylline D ICS + LABA or LAMA ICS and LAMA or ICS + LABA and LAMA or ICS+LABA and PDE4-inh. or LAMA and LABA or LAMA and PDE4-inh. Carbocysteine SABA and/or SAMA Theophylline

140
Exacerbations per year > 2 1 0 mMRC 0-1 CAT < 10 GOLD 4 mMRC > 2 CAT > 10 GOLD 3 GOLD 2 GOLD 1 SAMA prn or SABA prn LABA or LAMA ICS + LABA or LAMA Global Strategy for Diagnosis, Management and Prevention of COPD Manage Stable COPD: Pharmacologic Therapy FIRST CHOICE AB DC ICS + LABA or LAMA

141
> 2 1 0 mMRC 0-1 CAT < 10 GOLD 4 mMRC > 2 CAT > 10 GOLD 3 GOLD 2 GOLD 1 LAMA or LABA or SABA and SAMA LAMA and LABA ICS and LAMA or ICS + LABA and LAMA or ICS + LABA and PDE4-inh or LAMA and LABA or LAMA and PDE4-inh. LAMA and LABA Global Strategy for Diagnosis, Management and Prevention of COPD Manage Stable COPD: Pharmacologic Therapy SECOND CHOICE A DC B Exacerbations per year

142
> 2 1 0 mMRC 0-1 CAT < 10 GOLD 4 mMRC > 2 CAT > 10 GOLD 3 GOLD 2 GOLD 1 Theophylline PDE4-inh. SABA and/or SAMA Theophylline Carbocysteine SABA and/or SAMA Theophylline SABA and/or SAMA Theophylline Global Strategy for Diagnosis, Management and Prevention of COPD Manage Stable COPD: Pharmacologic Therapy ALTERNATIVE CHOICES A D C B Exacerbations per year

144
Bibliography Celi et al. The body mass-index, airflow obstruction, dyspnea, and exercise capacity in chronic obstructive pulmonary disease. N Engl J Med;350:1005-1012. Celi et al. The body mass-index, airflow obstruction, dyspnea, and exercise capacity in chronic obstructive pulmonary disease. N Engl J Med;350:1005-1012. Taskin et al. A 4-year trial of tiotropium in chronic obstructive pulmonary disease. N Engl J Med;359:1543-1554. Taskin et al. A 4-year trial of tiotropium in chronic obstructive pulmonary disease. N Engl J Med;359:1543-1554. Mannino DM et al. MMWR Surval Summary 2002;5. Mannino DM et al. MMWR Surval Summary 2002;5. Lethbridge and Cejku. Vital Health Stat 2006;232:1-153. Lethbridge and Cejku. Vital Health Stat 2006;232:1-153. Barr RG et al, Am J Med 2009;6:348-355. Barr RG et al, Am J Med 2009;6:348-355. Jemal A et al. JAMA 2005;294:1255-1259 Jemal A et al. JAMA 2005;294:1255-1259 Doherty et al. J Fam Prac 2006;55, supp S1-S8 Doherty et al. J Fam Prac 2006;55, supp S1-S8 Barnes PJ. N Eng J Med 2000;343:296-280 Barnes PJ. N Eng J Med 2000;343:296-280 Fletcher G et al. Br Med J 1977;1:1645-1648 Fletcher G et al. Br Med J 1977;1:1645-1648 Martinez FJ et al COPD 2008;5:85-95 Martinez FJ et al COPD 2008;5:85-95 Tinkelman et al, J Asthma 2006;43:75-80. Tinkelman et al, J Asthma 2006;43:75-80. Mosenifar A. Postgrad Med 2009;121:1-8. Mosenifar A. Postgrad Med 2009;121:1-8. Celi et al. The body mass-index, airflow obstruction, dyspnea, and exercise capacity in chronic obstructive pulmonary disease. N Engl J Med;350:1005-1012. Celi et al. The body mass-index, airflow obstruction, dyspnea, and exercise capacity in chronic obstructive pulmonary disease. N Engl J Med;350:1005-1012. Taskin et al. A 4-year trial of tiotropium in chronic obstructive pulmonary disease. N Engl J Med;359:1543-1554. Taskin et al. A 4-year trial of tiotropium in chronic obstructive pulmonary disease. N Engl J Med;359:1543-1554. Mannino DM et al. MMWR Surval Summary 2002;5. Mannino DM et al. MMWR Surval Summary 2002;5. Lethbridge and Cejku. Vital Health Stat 2006;232:1-153. Lethbridge and Cejku. Vital Health Stat 2006;232:1-153. Barr RG et al, Am J Med 2009;6:348-355. Barr RG et al, Am J Med 2009;6:348-355. Jemal A et al. JAMA 2005;294:1255-1259 Jemal A et al. JAMA 2005;294:1255-1259 Doherty et al. J Fam Prac 2006;55, supp S1-S8 Doherty et al. J Fam Prac 2006;55, supp S1-S8 Barnes PJ. N Eng J Med 2000;343:296-280 Barnes PJ. N Eng J Med 2000;343:296-280 Fletcher G et al. Br Med J 1977;1:1645-1648 Fletcher G et al. Br Med J 1977;1:1645-1648 Martinez FJ et al COPD 2008;5:85-95 Martinez FJ et al COPD 2008;5:85-95 Tinkelman et al, J Asthma 2006;43:75-80. Tinkelman et al, J Asthma 2006;43:75-80. Mosenifar A. Postgrad Med 2009;121:1-8. Mosenifar A. Postgrad Med 2009;121:1-8.

145
Bibliogrpahy Weitzenblum et al. Pulmonary hemodynamics in patients with chronic obstructive pulmonary disease before and during an episode of peripheral edema. Chest 1994; 105: 1377-82. Weitzenblum et al. Pulmonary hemodynamics in patients with chronic obstructive pulmonary disease before and during an episode of peripheral edema. Chest 1994; 105: 1377-82. ACCP / AACVPR. Pulmonary Rehabilitation Guidelines Panel. Panel. Pulmonary rehabilitation. Chest 1997; 112:1363-1396 ACCP / AACVPR. Pulmonary Rehabilitation Guidelines Panel. Panel. Pulmonary rehabilitation. Chest 1997; 112:1363-1396 Anthonisen NR et al. Effects of smoking intervention and the use of an inhaled Anticholinergic bronchodilator on the rate of decline of FEV1. JAMA 1994; 272:1497-1505. Anthonisen NR et al. Effects of smoking intervention and the use of an inhaled Anticholinergic bronchodilator on the rate of decline of FEV1. JAMA 1994; 272:1497-1505. ATS Statement. Standards for the diagnosis and care of patients with chronic obstructive pulmonary disease. Am J Respir Crit Care Med 1995; 152:S77-S120 ATS Statement. Standards for the diagnosis and care of patients with chronic obstructive pulmonary disease. Am J Respir Crit Care Med 1995; 152:S77-S120 Etnier J et al. The relationships among pulmonary function, aerobic fitness, and cognitive functioning in older COPD patients. Chest 1999; 116:953-960. Etnier J et al. The relationships among pulmonary function, aerobic fitness, and cognitive functioning in older COPD patients. Chest 1999; 116:953-960. Snow V et al. Evidence base management of acute exacerbations of chronic obstructive pulmonary disease. Ann Intern Med. 2001; 134:595- 599. Friedman M et al. Pharmacoeconomic evaluation of a combination of Ipratropium plus Albuterol compared with Ipratropium alone and Albuterol alone in COPD. Chest 1999; 115:635-641 Snow V et al. Evidence base management of acute exacerbations of chronic obstructive pulmonary disease. Ann Intern Med. 2001; 134:595- 599. Friedman M et al. Pharmacoeconomic evaluation of a combination of Ipratropium plus Albuterol compared with Ipratropium alone and Albuterol alone in COPD. Chest 1999; 115:635-641 The National Emphysema Treatment Trial Research Group. Rationale and design of the national emphysema treatment trial Chest 1999; 116:1750-1761. The National Emphysema Treatment Trial Research Group. Rationale and design of the national emphysema treatment trial Chest 1999; 116:1750-1761. Paggiaro et al. Multicenter randomized placebo-controlled trial of inhaled Fluticasone propionate in patients with chronic obstructive pulmonary disease. Lancet 1998; 351:773-80. Paggiaro et al. Multicenter randomized placebo-controlled trial of inhaled Fluticasone propionate in patients with chronic obstructive pulmonary disease. Lancet 1998; 351:773-80. Celli B. Pulmonary rehabilitation in patients with COPD Am J Respir Crit Care Med; 152:861-864Gray-Donald L et al. Nutritional status and mortality in chronic obstructive pulmonary disease. Am J Respir Crit Care Med 1996; 153:961-6. Celli B. Pulmonary rehabilitation in patients with COPD Am J Respir Crit Care Med; 152:861-864Gray-Donald L et al. Nutritional status and mortality in chronic obstructive pulmonary disease. Am J Respir Crit Care Med 1996; 153:961-6. Jones P. Quality of life changes in COPD patients treated with salmeterol. Am J Respir Crit Care Med 1997; 155:1283-1289 Jones P. Quality of life changes in COPD patients treated with salmeterol. Am J Respir Crit Care Med 1997; 155:1283-1289 Ramirez-Venegas et al. Salmeterol reduces dyspnea and improves lung function in patients with COPD. Chest 1997; 112:336-40 Ramirez-Venegas et al. Salmeterol reduces dyspnea and improves lung function in patients with COPD. Chest 1997; 112:336-40 Jones et al. Quality of life changes in COPD patients treated with salmeterol. Am J Respir Crit Care Med 1997; 155:1283-1289. Jones et al. Quality of life changes in COPD patients treated with salmeterol. Am J Respir Crit Care Med 1997; 155:1283-1289. Mahler et al. Efficacy of Salmeterol Xinafoate in the treatment of COPD. Chest 1999; 115:957-965. Mahler et al. Efficacy of Salmeterol Xinafoate in the treatment of COPD. Chest 1999; 115:957-965. Llewellyn-Jones et al. Effect of Fluticasone propionate on sputum of patents with chronic bronchitis and emphysema. Am J Respir Crit Care Med 1996; 153:616-21 Llewellyn-Jones et al. Effect of Fluticasone propionate on sputum of patents with chronic bronchitis and emphysema. Am J Respir Crit Care Med 1996; 153:616-21 Mahler D et al. Efficacy of salmeterol xinafoate in the treatment of COPD. Chest 1999;115:957-965. Mahler D et al. Efficacy of salmeterol xinafoate in the treatment of COPD. Chest 1999;115:957-965. Cazzola M et al. Additive effects of salmeterol and fluticasone or theophyline in COPD. Chest 2000; 118:1576-1581. Cazzola M et al. Additive effects of salmeterol and fluticasone or theophyline in COPD. Chest 2000; 118:1576-1581. Rennard et al. Extended therapy with Ipratropium is associated with improved lung function in patients with COPD. Chest 1996; 110:62- 70Tobias Welte, Marc Miravitlles, Paul Hernandez, Göran Eriksson, Stefan Peterson, Tomasz Polanowski, and Romain Kessler Efficacy and Tolerability of Budesonide/Formoterol Added to Tiotropium in Patients with Chronic Obstructive Pulmonary Disease Am. J. Respir. Crit. Care Med., Oct 2009; 180: 741 - 750. Rennard et al. Extended therapy with Ipratropium is associated with improved lung function in patients with COPD. Chest 1996; 110:62- 70Tobias Welte, Marc Miravitlles, Paul Hernandez, Göran Eriksson, Stefan Peterson, Tomasz Polanowski, and Romain Kessler Efficacy and Tolerability of Budesonide/Formoterol Added to Tiotropium in Patients with Chronic Obstructive Pulmonary Disease Am. J. Respir. Crit. Care Med., Oct 2009; 180: 741 - 750. Weitzenblum et al. Pulmonary hemodynamics in patients with chronic obstructive pulmonary disease before and during an episode of peripheral edema. Chest 1994; 105: 1377-82. Weitzenblum et al. Pulmonary hemodynamics in patients with chronic obstructive pulmonary disease before and during an episode of peripheral edema. Chest 1994; 105: 1377-82. ACCP / AACVPR. Pulmonary Rehabilitation Guidelines Panel. Panel. Pulmonary rehabilitation. Chest 1997; 112:1363-1396 ACCP / AACVPR. Pulmonary Rehabilitation Guidelines Panel. Panel. Pulmonary rehabilitation. Chest 1997; 112:1363-1396 Anthonisen NR et al. Effects of smoking intervention and the use of an inhaled Anticholinergic bronchodilator on the rate of decline of FEV1. JAMA 1994; 272:1497-1505. Anthonisen NR et al. Effects of smoking intervention and the use of an inhaled Anticholinergic bronchodilator on the rate of decline of FEV1. JAMA 1994; 272:1497-1505. ATS Statement. Standards for the diagnosis and care of patients with chronic obstructive pulmonary disease. Am J Respir Crit Care Med 1995; 152:S77-S120 ATS Statement. Standards for the diagnosis and care of patients with chronic obstructive pulmonary disease. Am J Respir Crit Care Med 1995; 152:S77-S120 Etnier J et al. The relationships among pulmonary function, aerobic fitness, and cognitive functioning in older COPD patients. Chest 1999; 116:953-960. Etnier J et al. The relationships among pulmonary function, aerobic fitness, and cognitive functioning in older COPD patients. Chest 1999; 116:953-960. Snow V et al. Evidence base management of acute exacerbations of chronic obstructive pulmonary disease. Ann Intern Med. 2001; 134:595- 599. Friedman M et al. Pharmacoeconomic evaluation of a combination of Ipratropium plus Albuterol compared with Ipratropium alone and Albuterol alone in COPD. Chest 1999; 115:635-641 Snow V et al. Evidence base management of acute exacerbations of chronic obstructive pulmonary disease. Ann Intern Med. 2001; 134:595- 599. Friedman M et al. Pharmacoeconomic evaluation of a combination of Ipratropium plus Albuterol compared with Ipratropium alone and Albuterol alone in COPD. Chest 1999; 115:635-641 The National Emphysema Treatment Trial Research Group. Rationale and design of the national emphysema treatment trial Chest 1999; 116:1750-1761. The National Emphysema Treatment Trial Research Group. Rationale and design of the national emphysema treatment trial Chest 1999; 116:1750-1761. Paggiaro et al. Multicenter randomized placebo-controlled trial of inhaled Fluticasone propionate in patients with chronic obstructive pulmonary disease. Lancet 1998; 351:773-80. Paggiaro et al. Multicenter randomized placebo-controlled trial of inhaled Fluticasone propionate in patients with chronic obstructive pulmonary disease. Lancet 1998; 351:773-80. Celli B. Pulmonary rehabilitation in patients with COPD Am J Respir Crit Care Med; 152:861-864Gray-Donald L et al. Nutritional status and mortality in chronic obstructive pulmonary disease. Am J Respir Crit Care Med 1996; 153:961-6. Celli B. Pulmonary rehabilitation in patients with COPD Am J Respir Crit Care Med; 152:861-864Gray-Donald L et al. Nutritional status and mortality in chronic obstructive pulmonary disease. Am J Respir Crit Care Med 1996; 153:961-6. Jones P. Quality of life changes in COPD patients treated with salmeterol. Am J Respir Crit Care Med 1997; 155:1283-1289 Jones P. Quality of life changes in COPD patients treated with salmeterol. Am J Respir Crit Care Med 1997; 155:1283-1289 Ramirez-Venegas et al. Salmeterol reduces dyspnea and improves lung function in patients with COPD. Chest 1997; 112:336-40 Ramirez-Venegas et al. Salmeterol reduces dyspnea and improves lung function in patients with COPD. Chest 1997; 112:336-40 Jones et al. Quality of life changes in COPD patients treated with salmeterol. Am J Respir Crit Care Med 1997; 155:1283-1289. Jones et al. Quality of life changes in COPD patients treated with salmeterol. Am J Respir Crit Care Med 1997; 155:1283-1289. Mahler et al. Efficacy of Salmeterol Xinafoate in the treatment of COPD. Chest 1999; 115:957-965. Mahler et al. Efficacy of Salmeterol Xinafoate in the treatment of COPD. Chest 1999; 115:957-965. Llewellyn-Jones et al. Effect of Fluticasone propionate on sputum of patents with chronic bronchitis and emphysema. Am J Respir Crit Care Med 1996; 153:616-21 Llewellyn-Jones et al. Effect of Fluticasone propionate on sputum of patents with chronic bronchitis and emphysema. Am J Respir Crit Care Med 1996; 153:616-21 Mahler D et al. Efficacy of salmeterol xinafoate in the treatment of COPD. Chest 1999;115:957-965. Mahler D et al. Efficacy of salmeterol xinafoate in the treatment of COPD. Chest 1999;115:957-965. Cazzola M et al. Additive effects of salmeterol and fluticasone or theophyline in COPD. Chest 2000; 118:1576-1581. Cazzola M et al. Additive effects of salmeterol and fluticasone or theophyline in COPD. Chest 2000; 118:1576-1581. Rennard et al. Extended therapy with Ipratropium is associated with improved lung function in patients with COPD. Chest 1996; 110:62- 70Tobias Welte, Marc Miravitlles, Paul Hernandez, Göran Eriksson, Stefan Peterson, Tomasz Polanowski, and Romain Kessler Efficacy and Tolerability of Budesonide/Formoterol Added to Tiotropium in Patients with Chronic Obstructive Pulmonary Disease Am. J. Respir. Crit. Care Med., Oct 2009; 180: 741 - 750. Rennard et al. Extended therapy with Ipratropium is associated with improved lung function in patients with COPD. Chest 1996; 110:62- 70Tobias Welte, Marc Miravitlles, Paul Hernandez, Göran Eriksson, Stefan Peterson, Tomasz Polanowski, and Romain Kessler Efficacy and Tolerability of Budesonide/Formoterol Added to Tiotropium in Patients with Chronic Obstructive Pulmonary Disease Am. J. Respir. Crit. Care Med., Oct 2009; 180: 741 - 750.

146
Bibliography Global Initiative Lung Disease 2009 Rabe et al. Amer J Respir Crit Care Med 2007;176:532-555. Celi BR et al, Eur Resp J.2004;23:932-946. Ramsy SD. Chest 2000;117 supplement:S335-375. Barnes PT. N Eng J Med 2000;343:269-280. Barnes PT. Am J Med 2004;117; 24s-32s. Donaldson GC. Thorax 2002;57:847-852. Cote CG. Chest 2007;13:696-704. Cooper and Taskin. BMJ 2005;330: 640-644 Global Initiative Lung Disease 2009 Rabe et al. Amer J Respir Crit Care Med 2007;176:532-555. Celi BR et al, Eur Resp J.2004;23:932-946. Ramsy SD. Chest 2000;117 supplement:S335-375. Barnes PT. N Eng J Med 2000;343:269-280. Barnes PT. Am J Med 2004;117; 24s-32s. Donaldson GC. Thorax 2002;57:847-852. Cote CG. Chest 2007;13:696-704. Cooper and Taskin. BMJ 2005;330: 640-644

147
Bibliography Decramer M. Eur Respir Rev. 2006;15:51-57. Decramer M. Eur Respir Rev. 2006;15:51-57. Mannino DM, et al. MMWR Morb Mortal Wkly Rep. 2002;51(SS06):1-16. Mannino DM, et al. MMWR Morb Mortal Wkly Rep. 2002;51(SS06):1-16. Barnes PJ. Med Princ Pract. 2010;19(5):330-338. Barnes PJ. Med Princ Pract. 2010;19(5):330-338. Brown DW, et al. MMWR Weekly. 2008;57(45):1229-1232 Brown DW, et al. MMWR Weekly. 2008;57(45):1229-1232 Celli BR. Proc Am Thorac Soc. 2006;3:461-465. Celli BR. Proc Am Thorac Soc. 2006;3:461-465. Decramer M. Eur Respir Rev. 2006;15:51-57. Decramer M. Eur Respir Rev. 2006;15:51-57. Mannino DM, et al. MMWR Morb Mortal Wkly Rep. 2002;51(SS06):1-16. Mannino DM, et al. MMWR Morb Mortal Wkly Rep. 2002;51(SS06):1-16. Barnes PJ. Med Princ Pract. 2010;19(5):330-338. Barnes PJ. Med Princ Pract. 2010;19(5):330-338. Brown DW, et al. MMWR Weekly. 2008;57(45):1229-1232 Brown DW, et al. MMWR Weekly. 2008;57(45):1229-1232 Celli BR. Proc Am Thorac Soc. 2006;3:461-465. Celli BR. Proc Am Thorac Soc. 2006;3:461-465.
:1-16. Mannino DM, et al. MMWR Morb Mortal Wkly Rep. 2002;51(SS06):1-16. Barnes PJ. Med Princ Pract. 2010;19(5): Barnes PJ. Med Princ Pract. 2010;19(5): Brown DW, et al. MMWR Weekly. 2008;57(45): Brown DW, et al. MMWR Weekly. 2008;57(45): Celli BR. Proc Am Thorac Soc. 2006;3: Celli BR. Proc Am Thorac Soc. 2006;3: Decramer M. Eur Respir Rev. 2006;15: Decramer M. Eur Respir Rev. 2006;15: Mannino DM, et al. MMWR Morb Mortal Wkly Rep. 2002;51(SS06):1-16. Mannino DM, et al. MMWR Morb Mortal Wkly Rep. 2002;51(SS06):1-16. Barnes PJ. Med Princ Pract. 2010;19(5): Barnes PJ. Med Princ Pract. 2010;19(5): Brown DW, et al. MMWR Weekly. 2008;57(45): Brown DW, et al. MMWR Weekly. 2008;57(45): Celli BR. Proc Am Thorac Soc. 2006;3: Celli BR. Proc Am Thorac Soc. 2006;3:")
148
Bibliography Tamagawa E et al. Chest. 2006;130:1631-1633. Tamagawa E et al. Chest. 2006;130:1631-1633. Curkendall SM, et al. Ann Epidemiol. 2006;16:63-70. Curkendall SM, et al. Ann Epidemiol. 2006;16:63-70. Sin DD, et al. Am J Med 2003;114:10- 14. Sin DD, et al. Am J Med 2003;114:10- 14. de Vries F, et al. Eur Respir J. 2005;25:879-884. de Vries F, et al. Eur Respir J. 2005;25:879-884. Maltais F, et al. Am J Respir Crit Care Med. 1996;153:288-293. Maltais F, et al. Am J Respir Crit Care Med. 1996;153:288-293.. Tamagawa E et al. Chest. 2006;130:1631-1633. Tamagawa E et al. Chest. 2006;130:1631-1633. Curkendall SM, et al. Ann Epidemiol. 2006;16:63-70. Curkendall SM, et al. Ann Epidemiol. 2006;16:63-70. Sin DD, et al. Am J Med 2003;114:10- 14. Sin DD, et al. Am J Med 2003;114:10- 14. de Vries F, et al. Eur Respir J. 2005;25:879-884. de Vries F, et al. Eur Respir J. 2005;25:879-884. Maltais F, et al. Am J Respir Crit Care Med. 1996;153:288-293. Maltais F, et al. Am J Respir Crit Care Med. 1996;153:288-293..

149
Bibliogrpahy Balasubramanian VP, Varkey B. Curr Opin Pulm Med. 2006;12:106-112 Balasubramanian VP, Varkey B. Curr Opin Pulm Med. 2006;12:106-112 Schols AM, et al. Am J Respir Crit Care Med. 1998;157(6 Pt 1):1791-1797. Schols AM, et al. Am J Respir Crit Care Med. 1998;157(6 Pt 1):1791-1797. Kunik ME, et al. Chest. 2005;127:1205- 1211. Norwood R. Curr Opin Pulm Med. 2006;12:113-117. Felker B, et al. Gen Hosp Psych. 2001;23:56-61. Oswald-Mammosser M, et al. Chest. 1995;107:1193-1198. Balasubramanian VP, Varkey B. Curr Opin Pulm Med. 2006;12:106-112 Balasubramanian VP, Varkey B. Curr Opin Pulm Med. 2006;12:106-112 Schols AM, et al. Am J Respir Crit Care Med. 1998;157(6 Pt 1):1791-1797. Schols AM, et al. Am J Respir Crit Care Med. 1998;157(6 Pt 1):1791-1797. Kunik ME, et al. Chest. 2005;127:1205- 1211. Norwood R. Curr Opin Pulm Med. 2006;12:113-117. Felker B, et al. Gen Hosp Psych. 2001;23:56-61. Oswald-Mammosser M, et al. Chest. 1995;107:1193-1198.
: Schols AM, et al. Am J Respir Crit Care Med. 1998;157(6 Pt 1): Kunik ME, et al. Chest. 2005;127: Norwood R. Curr Opin Pulm Med. 2006;12: Felker B, et al. Gen Hosp Psych. 2001;23: Oswald-Mammosser M, et al. Chest. 1995;107: Balasubramanian VP, Varkey B. Curr Opin Pulm Med. 2006;12: Balasubramanian VP, Varkey B. Curr Opin Pulm Med. 2006;12: Schols AM, et al. Am J Respir Crit Care Med. 1998;157(6 Pt 1): Schols AM, et al. Am J Respir Crit Care Med. 1998;157(6 Pt 1): Kunik ME, et al. Chest. 2005;127: Norwood R. Curr Opin Pulm Med. 2006;12: Felker B, et al. Gen Hosp Psych. 2001;23: Oswald-Mammosser M, et al. Chest. 1995;107:")
150
Bibliography Martinez FJ, et al. COPD. 2008;5:85-95. Martinez FJ, et al. COPD. 2008;5:85-95. Lin K, et al. Ann Intern Med. 2008;148(7):535-543. Lin K, et al. Ann Intern Med. 2008;148(7):535-543. Celli BR, et al. N Engl J Med. 2004;350:1005-1012. Celli BR, et al. N Engl J Med. 2004;350:1005-1012. Gonzales D, et al. JAMA. 2006;296:47- 55. Jorenby DE, et al. JAMA. 2006;296:56- 63. Gonzales D, et al. JAMA. 2006;296:47- 55. Jorenby DE, et al. JAMA. 2006;296:56- 63. Tashkin DP, et al. Chest. 2010 Sep 23. [Epub ahead of print] Tashkin DP, et al. Chest. 2010 Sep 23. [Epub ahead of print] Martinez FJ, et al. COPD. 2008;5:85-95. Martinez FJ, et al. COPD. 2008;5:85-95. Lin K, et al. Ann Intern Med. 2008;148(7):535-543. Lin K, et al. Ann Intern Med. 2008;148(7):535-543. Celli BR, et al. N Engl J Med. 2004;350:1005-1012. Celli BR, et al. N Engl J Med. 2004;350:1005-1012. Gonzales D, et al. JAMA. 2006;296:47- 55. Jorenby DE, et al. JAMA. 2006;296:56- 63. Gonzales D, et al. JAMA. 2006;296:47- 55. Jorenby DE, et al. JAMA. 2006;296:56- 63. Tashkin DP, et al. Chest. 2010 Sep 23. [Epub ahead of print] Tashkin DP, et al. Chest. 2010 Sep 23. [Epub ahead of print]
: Lin K, et al. Ann Intern Med. 2008;148(7): Celli BR, et al. N Engl J Med. 2004;350: Celli BR, et al. N Engl J Med. 2004;350: Gonzales D, et al. JAMA. 2006;296: Jorenby DE, et al. JAMA. 2006;296: Gonzales D, et al. JAMA. 2006;296: Jorenby DE, et al. JAMA. 2006;296: Tashkin DP, et al. Chest Sep 23. [Epub ahead of print] Tashkin DP, et al. Chest Sep 23. [Epub ahead of print] Martinez FJ, et al. COPD. 2008;5: Martinez FJ, et al. COPD. 2008;5: Lin K, et al. Ann Intern Med. 2008;148(7): Lin K, et al. Ann Intern Med. 2008;148(7): Celli BR, et al. N Engl J Med. 2004;350: Celli BR, et al. N Engl J Med. 2004;350: Gonzales D, et al. JAMA. 2006;296: Jorenby DE, et al. JAMA. 2006;296: Gonzales D, et al. JAMA. 2006;296: Jorenby DE, et al. JAMA. 2006;296: Tashkin DP, et al. Chest Sep 23. [Epub ahead of print] Tashkin DP, et al. Chest Sep 23. [Epub ahead of print].")
151
Bibliography Blondal T, et al. BMJ1999;318:285-288. Blondal T, et al. BMJ1999;318:285-288. Tashkin DP, and Murray RP. Respir Med. 2009;103:963-974. Tashkin DP, and Murray RP. Respir Med. 2009;103:963-974. Calverley PM, et al. Lancet. 2009;374(9691):685-694. Calverley PM, et al. Lancet. 2009;374(9691):685-694. Tashkin DP, et al. Drugs. 2008;68:1975- 2000. Tashkin DP, et al. Drugs. 2008;68:1975- 2000. Rennard SI, et al. Drugs. 2009;69:549- 565. Rennard SI, et al. Drugs. 2009;69:549- 565. Dahl R, et al. Thorax. 2010;65(6):473- 479. Dahl R, et al. Thorax. 2010;65(6):473- 479. Blondal T, et al. BMJ1999;318:285-288. Blondal T, et al. BMJ1999;318:285-288. Tashkin DP, and Murray RP. Respir Med. 2009;103:963-974. Tashkin DP, and Murray RP. Respir Med. 2009;103:963-974. Calverley PM, et al. Lancet. 2009;374(9691):685-694. Calverley PM, et al. Lancet. 2009;374(9691):685-694. Tashkin DP, et al. Drugs. 2008;68:1975- 2000. Tashkin DP, et al. Drugs. 2008;68:1975- 2000. Rennard SI, et al. Drugs. 2009;69:549- 565. Rennard SI, et al. Drugs. 2009;69:549- 565. Dahl R, et al. Thorax. 2010;65(6):473- 479. Dahl R, et al. Thorax. 2010;65(6):473- 479.
: Calverley PM, et al. Lancet. 2009;374(9691): Tashkin DP, et al. Drugs. 2008;68: Tashkin DP, et al. Drugs. 2008;68: Rennard SI, et al. Drugs. 2009;69: Rennard SI, et al. Drugs. 2009;69: Dahl R, et al. Thorax. 2010;65(6): Dahl R, et al. Thorax. 2010;65(6): Blondal T, et al. BMJ1999;318: Blondal T, et al. BMJ1999;318: Tashkin DP, and Murray RP. Respir Med. 2009;103: Tashkin DP, and Murray RP. Respir Med. 2009;103: Calverley PM, et al. Lancet. 2009;374(9691): Calverley PM, et al. Lancet. 2009;374(9691): Tashkin DP, et al. Drugs. 2008;68: Tashkin DP, et al. Drugs. 2008;68: Rennard SI, et al. Drugs. 2009;69: Rennard SI, et al. Drugs. 2009;69: Dahl R, et al. Thorax. 2010;65(6): Dahl R, et al. Thorax. 2010;65(6):")
152
Bibliography Decramer M. Eur Respir Rev Decramer M. Eur Respir Rev2006;15:51-57. Aaron SD, et al. Ann Intern Med. 2007;146(8):545-555. Griffiths TL, et al. Lancet. 2000;355:362- 368. Ferreira IM, et al. Cochrane Database Syst Rev. 2009;(2):CD000998. Albert et al. Azithromycin for prevention of exacerbations of COPD. N Engl J Med 2011;365:689-698. Decramer M. Eur Respir Rev Decramer M. Eur Respir Rev2006;15:51-57. Aaron SD, et al. Ann Intern Med. 2007;146(8):545-555. Griffiths TL, et al. Lancet. 2000;355:362- 368. Ferreira IM, et al. Cochrane Database Syst Rev. 2009;(2):CD000998. Albert et al. Azithromycin for prevention of exacerbations of COPD. N Engl J Med 2011;365:689-698.
: Griffiths TL, et al. Lancet. 2000;355: Ferreira IM, et al. Cochrane Database Syst Rev. 2009;(2):CD Albert et al. Azithromycin for prevention of exacerbations of COPD. N Engl J Med 2011;365: Decramer M. Eur Respir Rev Decramer M. Eur Respir Rev2006;15: Aaron SD, et al. Ann Intern Med. 2007;146(8): Griffiths TL, et al. Lancet. 2000;355: Ferreira IM, et al. Cochrane Database Syst Rev. 2009;(2):CD Albert et al. Azithromycin for prevention of exacerbations of COPD. N Engl J Med 2011;365:")
153
Bibliography D’Uzo et al. Improvements in lung function with twice-daily Aclidinium bromide: results of a long-term, phase 3 trial in patients with chronic obstructive pulmonary disease. Chest:2012;142 Meeting Abstract D’Uzo et al. Improvements in lung function with twice-daily Aclidinium bromide: results of a long-term, phase 3 trial in patients with chronic obstructive pulmonary disease. Chest:2012;142 Meeting Abstract

Similar presentations
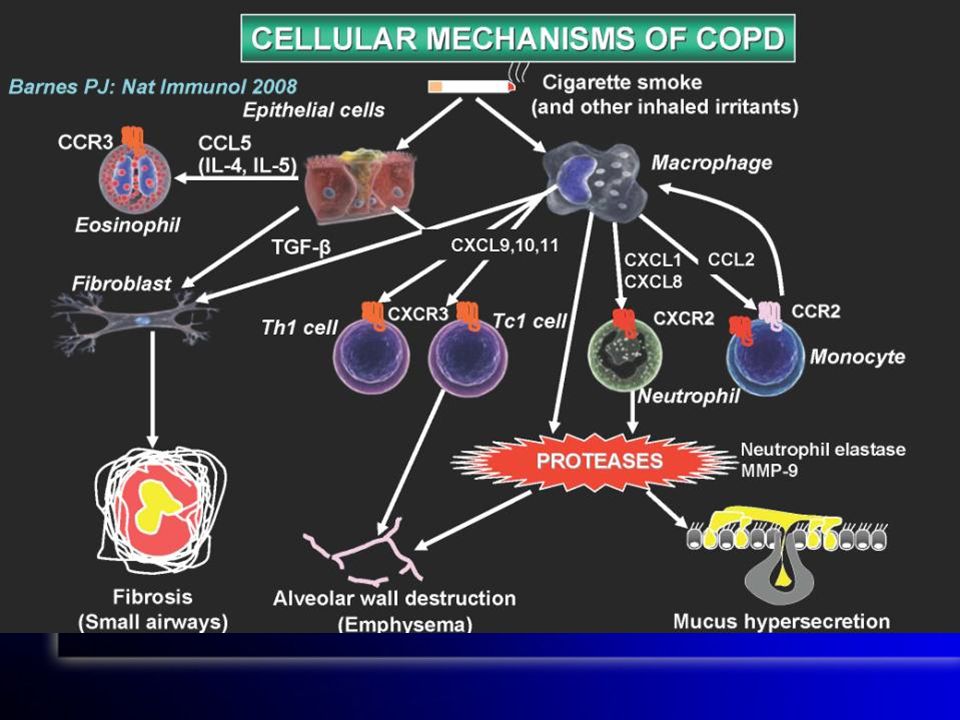
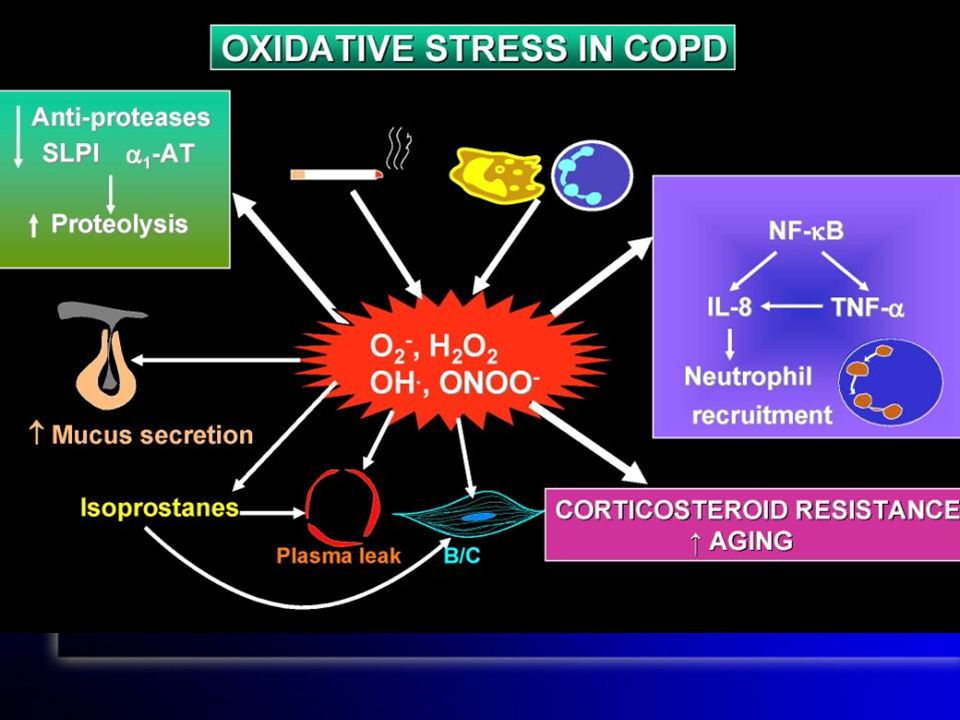
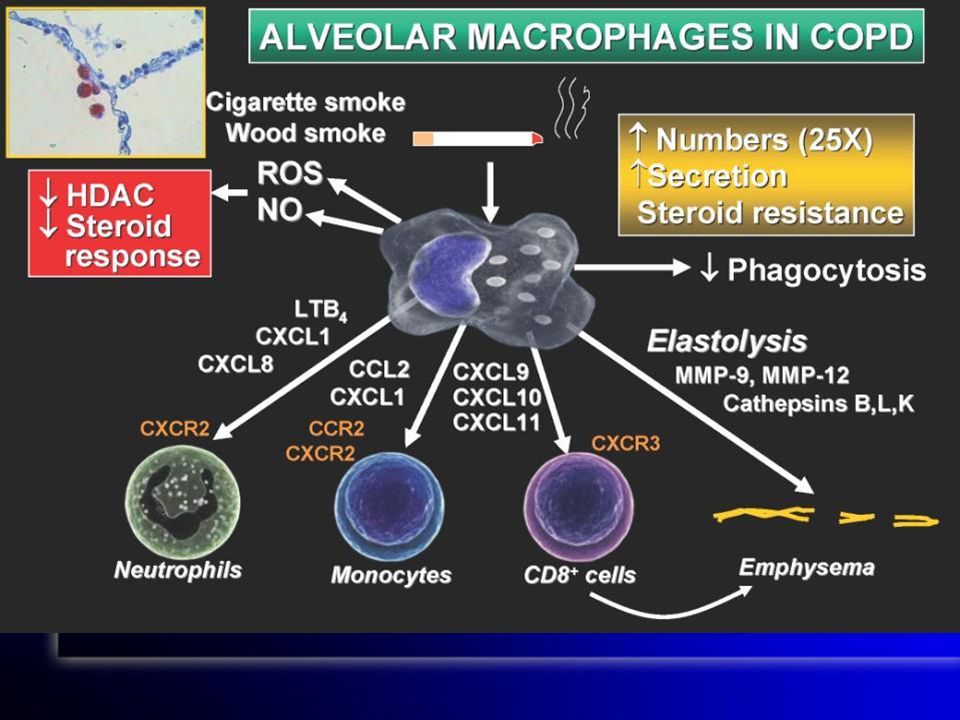
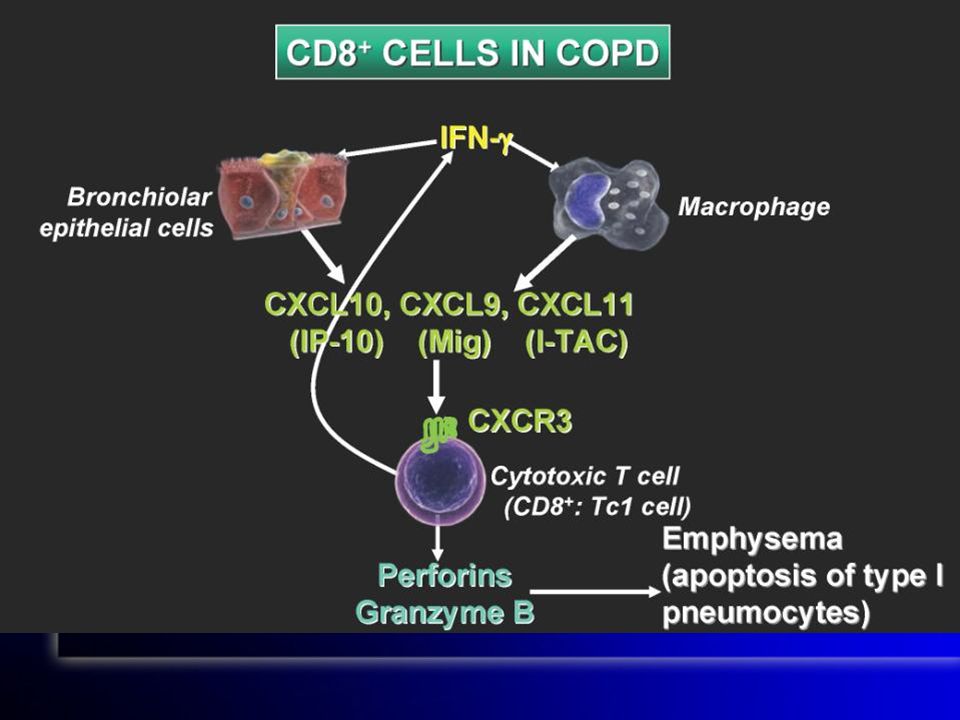
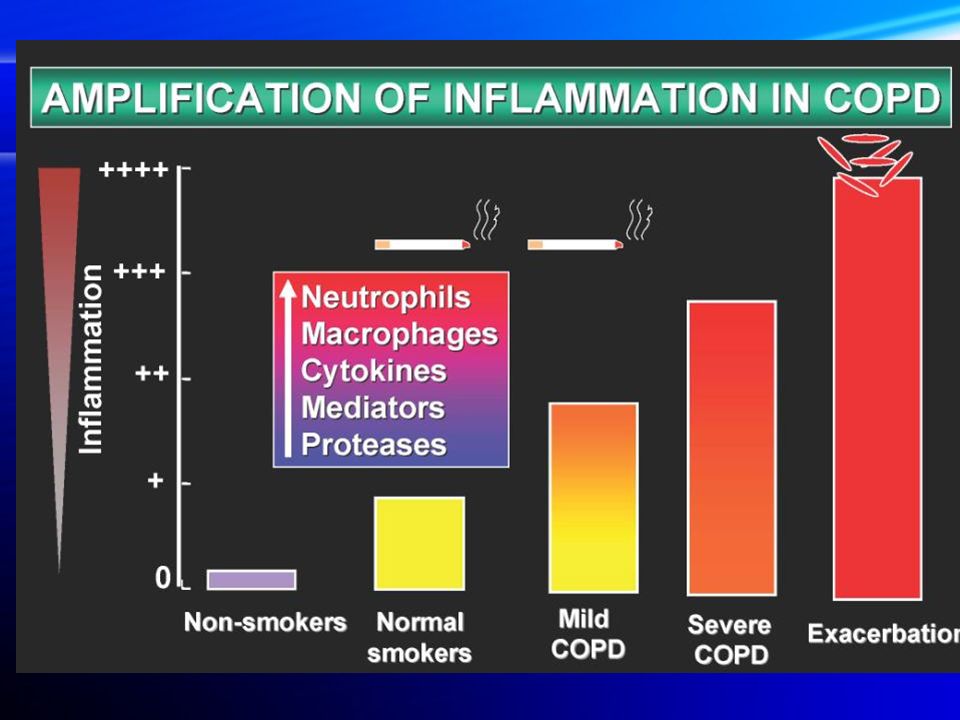
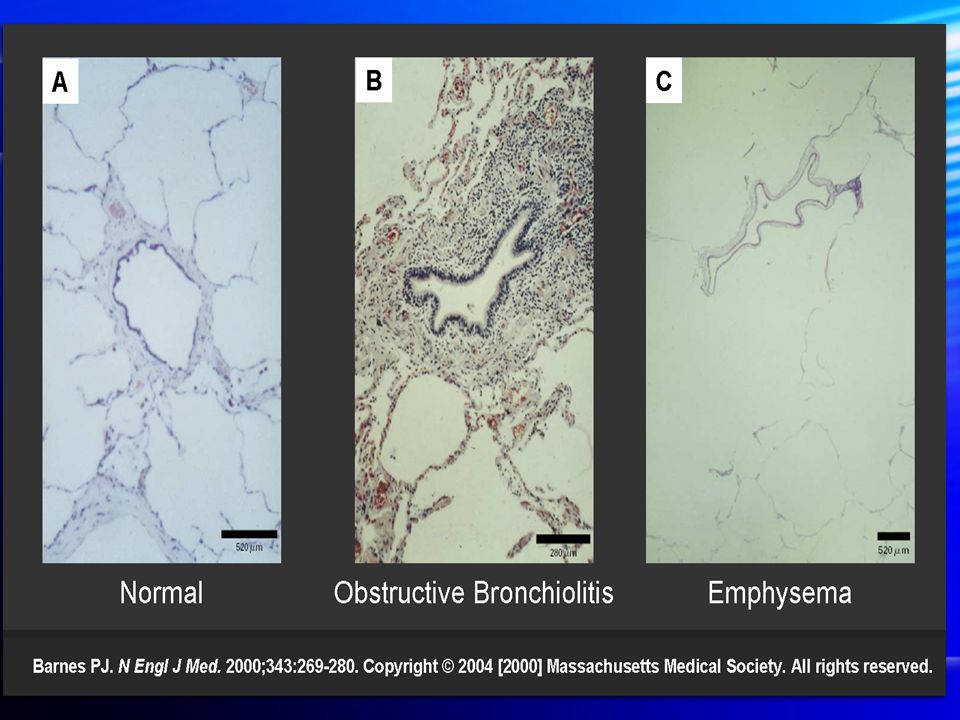
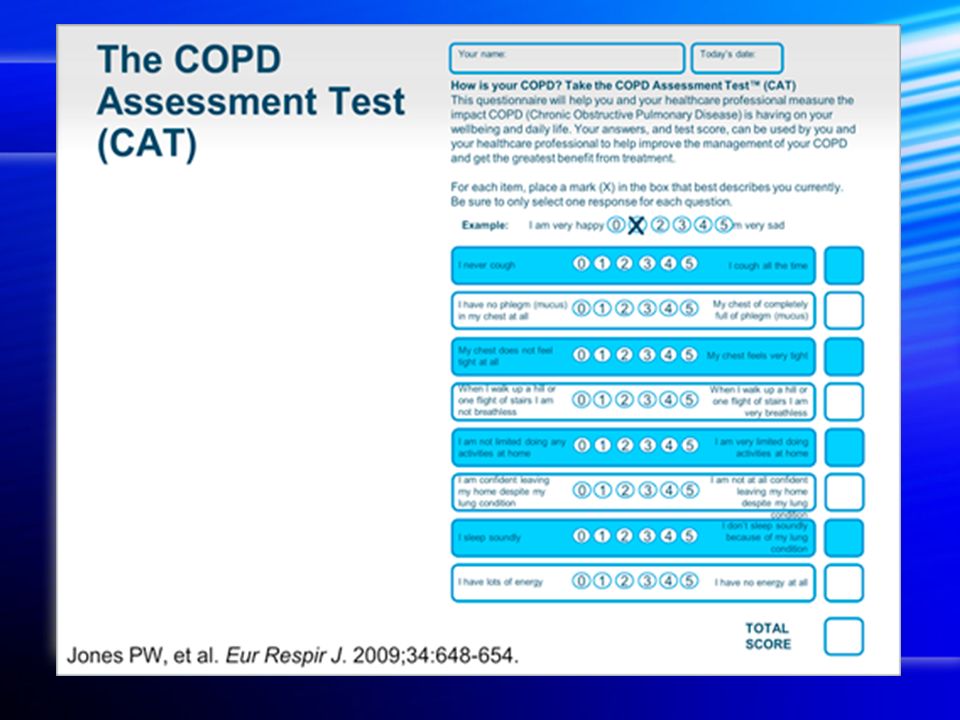

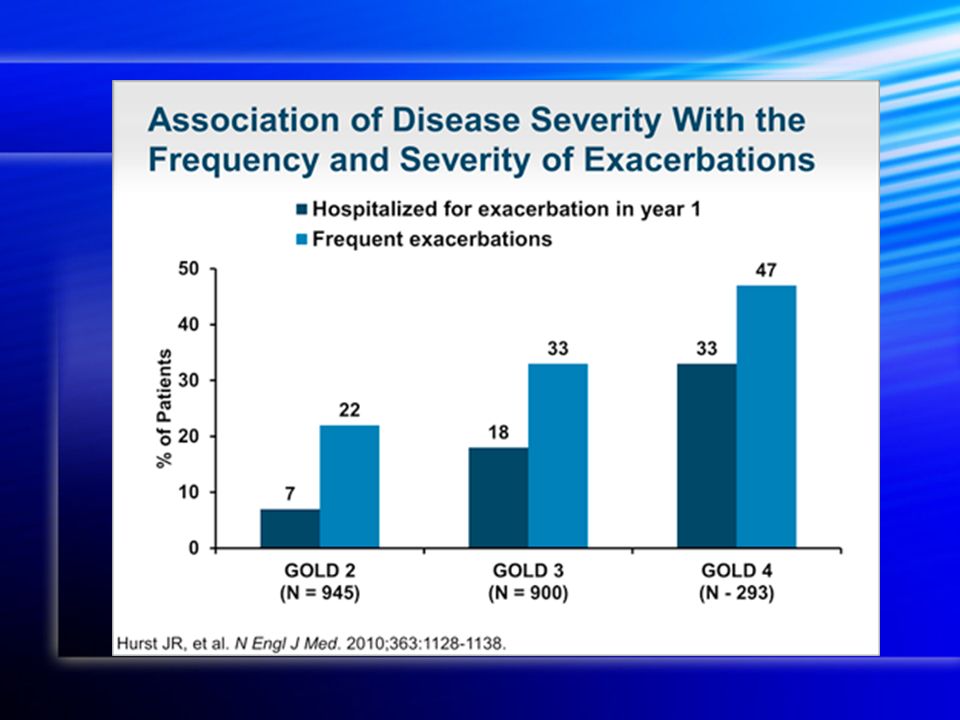
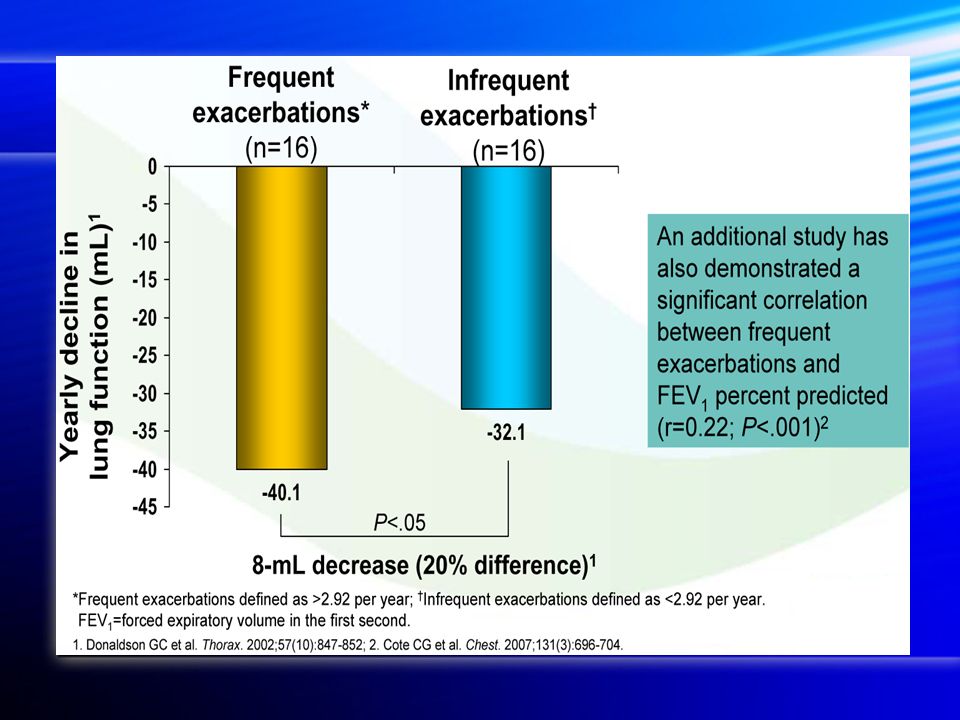



>")
:880-887. Beta-blockers may reduce.>")

 Note to the Speaker: All bold underlined statements must be read aloud to the.>")









>")




 as:*>")