Download presentation
Presentation is loading. Please wait.

1
Pathophysiology in the Treatment of Type 2 Diabetes Newer Agents Part 3 of 5

2
2 Incretins Nutrient stimulated gut hormones Favorable effects on glucose metabolism Major humans incretins 1,2 – Glucagon-like peptide-1 (GLP-1) – Glucose-dependent insulinotropic polypeptide (GIP) “Incretin effect” 1 Drucker DJ. Diabetes Educator. 2006;32(Suppl 2):65S-71S. 2 Vilsbøll T, Holst JJ. Diabetologia. 2004;47:357-366.
:65S-71S. 2 Vilsbøll T, Holst JJ. Diabetologia. 2004;47:")
3
3 Glucagon-like Peptide-1 (GLP-1) Most well-characterized incretin Secreted from L cells of the intestines Very short half-life Possibly deficient and GLP-1 resistance in type 2 diabetes Adapted from Aronoff SL, et al. Diabetes Spectrum. 2004;17:183-190.

5
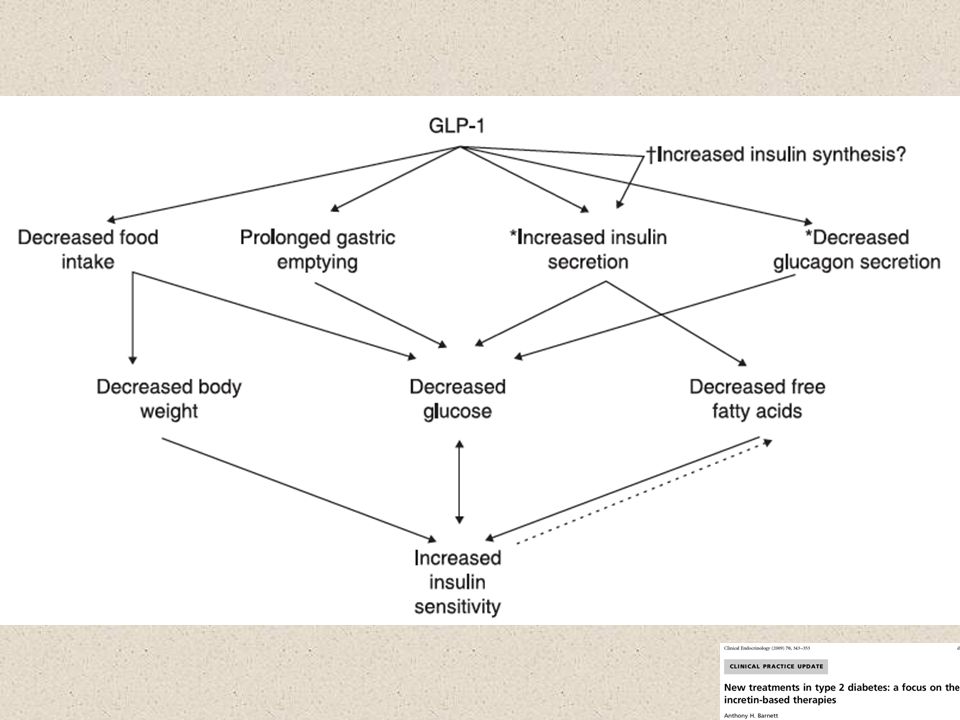
Insulin secretion - overcomes decreased insulin secretion of steroids and tacrolimus Glucagon secretion Gastric emptying Appetite Cardioprotection Cardiac output Insulin biosynthesis cell proliferation cell apoptosis Neuroprotection Glucose production Insulin sensitivity Brain Heart GI tract Liver Muscle Stomach GLP-1 Drucker D. J. Cell Metabolism 2006 Summary of Incretin Actions on Different Target Tissues Flint A, et al. J Clin Invest.1998;101:515-520. Larsson H, et al. Acta Physiol Scand.1997;160:413-422. Nauck MA, et al. Diabetologia.1996;1546-1553. Drucker DJ. Diabetes.1998;47:159-169. Schwartz, Kohl, "Type 2 Diabetes Mellitus and the Cardiometabolic Syndrome: Impact of Incretin-based Therapies","Diabetes, Metabolic Syndrome and Obesity: Targets and Therapy". 7/10

6
Müller WA, et al. N Engl J Med. 1970;283:109-115. Hyperglycemia in Type 2 Diabetes Results from Abnormal Meal-Related Insulin and Glucagon Dynamics Glucose (mg %) Insulin (µU/mL) Glucagon (pg/mL) Time (min) -60 060120180240 PremealPostmeal Insulin Insulin Glucagon HGP Glucagon HGP FPG PPG Meal 120 90 60 30 0 140 130 120 110 100 90 360 330 300 270 T2DM (n=12) Normal (n=11) 240 110 80
 Insulin (µU/mL) Glucagon (pg/mL) Time (min) PremealPostmeal Insulin Insulin Glucagon HGP Glucagon HGP FPG PPG Meal T2DM (n=12) Normal (n=11)")
7
Mean (SE); *P < 0.05GLP-1 = glucagon-like peptide-1 Glucose-dependent Effects of GLP-1 Glucose (mg/dL)Insulin (pmol/L) Glucagon (pmol/L) Type 2 Diabetes (n = 10) Placebo GLP-1 270 180 90 0 -30060120180240 300 200 100 0 -30060120180240 20 10 0 -30060120180240 Time (min) * * * * * * * * * * * * * * * * * * * Adapted from Nauck MA, et al. Diabetologia. 1993;36:741–744.

8
CV effects of GLP-1, GLP-1 RA, DPP-4 Inh.

9
Glp1 in major Surgery in DM- Benefit in Stress/ Steroid DM Added by Dr S

10
Strategies for Enhancing GLP-1 Action GLP-1 receptor agonists (resistant to DPP-4) – Exenatide – Liraglutide DPP-4 inhibitors – Inhibit actions of DPP-4 – Sitagliptin, saxagliptin
 – Exenatide – Liraglutide DPP-4 inhibitors – Inhibit actions of DPP-4 – Sitagliptin, saxagliptin")
11
Pharmacologically achieving GLP-1 effects Release of active incretins GLP-1 and GIP Blood glucose in fasting and postprandial states Ingestion of food Glucagon Hepatic glucose production GI tract DPP-4 enzyme Inactive GLP-1 X Sitagliptin Saxagliptin (DPP-4 inhibitors) Insulin Glucose- dependent Glucose dependent Pancreas Inactive GIP GLP-1=glucagon-like peptide-1; GIP=glucose-dependent insulinotropic polypeptide. Beta cells Alpha cells Glucose uptake by peripheral tissue GLP-1 receptor agonists Resists degradation by DPP-4 GLP-1 like effect GLP agonists 7-10 x DPP4-I 2-3 x GLP-1 Receptor Agonists= parenteral, weight loss, nausea risk DPP-4 Inhibitor = oral, weight neutral, no nausea

12
Sitagliptin, Saxagliptin Mechanism: Glucose-dependent insulin secretion and glucagon secretion Lowers PPG more than FPG Efficacy: modest ( HbA1c 0.6-0.8%) Advantages: weight neutral, no hypoglycemia, may use in patients with any degree renal dysfunction (dose appropriately), infrequent dosing Disadvantages: hypersensitivity reactions, ?pancreatitis (sitagliptin); interaction with CYP3A 4/5 strong inhibitors (saxagliptin); cost DPP-4 Inhibitors
 Advantages: weight neutral, no hypoglycemia, may use in patients with any degree renal dysfunction (dose appropriately), infrequent dosing Disadvantages: hypersensitivity reactions, pancreatitis (sitagliptin); interaction with CYP3A 4/5 strong inhibitors (saxagliptin); cost DPP-4 Inhibitors")
13
HgA1c Drop with DPP-4 Inhibitors

14
*P<0.001 vs comparator. 1. Aschner P, et al. Diabetes Care. 2006;29:2632-2637. 2. Nauck MA, et al. Diabetes Obes Metab. 2007;9:194-205. 3. Rosenstock J, et al. Clin Ther. 2006;28:1556-1568. 4. Hermansen K, et al. Diabetes Obes Metab. 2007;9:733-745. 5. Vilsbøll T, et al. Diabetes Obes Metab. 2010;12:167-177. 6. Derosa G, et al. Metab Clin Exp. 2010;59:887-895. Weight (kg) Weight Changes With Sitagliptin: Mono and Combination Therapy Monotherapy 24 Weeks 1 Monotherapy 24 Weeks 2 Add-on to Pioglitazone 24 Weeks 3 Add-on to Glimepiride 24 Weeks 4 Add-on to Insulin 24 Weeks 5 Add-on to Pio vs Met+Pio 12 Months 6 N741793353441641151 TreatmentPBOSitGlipSitPioSit + Pio GlimSit + Glim InsSit + Ins Met + Pio Sit + Pio * *
 Weight Changes With Sitagliptin: Mono and Combination Therapy Monotherapy 24 Weeks 1 Monotherapy 24 Weeks 2 Add-on to Pioglitazone 24 Weeks 3 Add-on to Glimepiride 24 Weeks 4 Add-on to Insulin 24 Weeks 5 Add-on to Pio vs Met+Pio 12 Months 6 N TreatmentPBOSitGlipSitPioSit + Pio GlimSit + Glim InsSit + Ins Met + Pio Sit + Pio * *.")
15
*P=0.01 vs glyburide uptitration. 1. Rosenstock J, et al. Curr Med Res Opin. 2009;25:2401-2411. 2. Jadzinsky M, et al. Diabetes Obes Metab. 2009;11:611-622. 3. DeFronzo RA, et al. Diabetes Care. 2009;32:1649-1655. 4. Scheen AJ, et al. Diabetes Metab Res Rev. 2010;26:540-549. 5. Chacra AR, et al. Int J Clin Pract. 2009;63:1395-1406. 6. Hollander P, et al. J Clin Endocrinol Metab. 2009;94:4810-4819. Weight (kg) Weight Changes With Saxagliptin: Mono and Combination Therapy Monotherapy 24 Weeks 1 Initial Combo w/ Metformin 24 Weeks 2 Add-on to Metformin 24 Weeks 3 Add-on to Metformin 18 Weeks 4 Add-on to Glyburide vs Uptitration 24 Weeks 5 Add-on to TZD 24 Weeks 6 N4011306743801768565 TreatmentPBOSaxMetSax + Met MetSax + Met Sit + Met Sax + Met GlySax + Gly TZDSax + TZD *
 Weight Changes With Saxagliptin: Mono and Combination Therapy Monotherapy 24 Weeks 1 Initial Combo w/ Metformin 24 Weeks 2 Add-on to Metformin 24 Weeks 3 Add-on to Metformin 18 Weeks 4 Add-on to Glyburide vs Uptitration 24 Weeks 5 Add-on to TZD 24 Weeks 6 N TreatmentPBOSaxMetSax + Met MetSax + Met Sit + Met Sax + Met GlySax + Gly TZDSax + TZD *.")
16
16 DPP-4 Inhibitors: Summary Oral once-daily agents with glucose-lowering potential Can be used as monotherapy and as part of combination therapy strategies (sitagliptin approved for combination with Insulin) A1C reduction Well tolerated Weight neutral
 A1C reduction Well tolerated Weight neutral")
Similar presentations



 + GIP = incretin effect =Augmentation of insulin after oral glucose Type 2 diabetics little incretin effect Reduced GLP-1 secretion.>")
 HbA1c – IFFC (mmol/mol) 6.042 6.548 7.053 7.559 8.064 9.075.>")














 8 : 20 ~ 8 : 50 B 棟 8 階カンファレンスルーム 薬剤部 TTSP 石井 英俊.>")