Download presentation
Presentation is loading. Please wait.

1
Wound Healing Natasha Holder MD, MSc, FRCSC
Orthopaedic Oncology Fellow For Dr. Joel Werier

2
Objectives Describe the pathophysiology of wound healing
Describe the complications of wound healing Describe how to treat and prevent wound complications Describe scar formation and clinical treatments for abnormal scars

3
What is a wound? A wound is a disruption of the normal structure and function of the skin and underlying soft tissue

4
Wound Classification Acute:
normal, healthy individuals heal through an orderly sequence of physiological events that include hemostasis, inflammation, epithelialization, fibroplasia, and maturation Easily identifiable mechanism e.g. trauma Chronic: Physiologic process is altered or stalled more likely to occur in patients with underlying disorders such as peripheral artery disease, diabetes, venous insufficiency, nutritional deficiencies, and other disease states Wounds are generally classified as acute or chronic. Although there is no specific time frame determining the difference between an acute or chronic wound, chronic wounds are generally associated with physiological impairments that slow or prevent wound healing. Wounds may be caused by a variety of mechanisms including acute injury to the skin (abrasion, puncture, crush), surgery and other etiologies that cause initially intact skin to break down (eg, ischemia, pressure).
, surgery and other etiologies that cause initially intact skin to break down (eg, ischemia, pressure).")
5
Phases of Wound Healing
Mediated by the activation of Keratinocytes Fibroblasts Endothelial cells Macrophages Platelets Organized cell migration and recruitment of endothelial cells for angiogenesis Many growth factors and cytokines are also released Wound healing occurs as a cellular response to tissue injury and involves the activation

6
Phases of Wound Healing
Immediately after injury to the skin, small vessels within the wound constrict to provide at least a measure of hemostasis for 5 to 10 minutes. Platelets aggregate in severed vessels and trigger the clotting cascade and release essential growth factors and cytokines that are important for the initiation and progression of wound healing (eg, platelet-derived growth factor, transforming growth factor-β). The fibrin matrix that results stabilizes the wound and provides a provisional scaffold for the wound healing process.
. The fibrin matrix that results stabilizes the wound and provides a provisional scaffold for the wound healing process.")
7
Phases of Wound Healing
Inflammatory Proliferative Maturation Once hemostasis is achieved acute wounds normally heal in an orderly and efficient manner characterized by overlapping phases that include inflammation, proliferation, and maturation

8
Phases of Wound Healing
Inflammatory Immediate to 2-5 days Hemostasis is achieved Constriction of blood supply Platelets aggregate to start clotting cascade Inflammation Increased vascular permeability Multiple cellular cascades The inflammatory phase is completed within three days, except in the presence of infection or other causes of wound chronicity (arrested in this phase). Key components of this phase are increased vascular permeability and cellular recruitment. Multiple events contribute to these processes including: ●Mononuclear leukocytes accumulate and are transformed into macrophages ●Mast cells degranulate, releasing histamine and other mediators of vasodilation and cellular migration. ●Release of vasoactive substances from stromal mast cells makes small vessels permeable to molecular and cellular mediators of the inflammatory response. The resulting accumulation of plasma and cellular elements is noted clinically as edema, or swelling. ●Chemotaxis results in migration and concentration of polymorphonuclear leukocytes that digest bacteria, foreign debris, and necrotic tissue with lysosomal enzymes.
. Key components of this phase are increased vascular permeability and cellular recruitment. Multiple events contribute to these processes including: ●Mononuclear leukocytes accumulate and are transformed into macrophages. ●Mast cells degranulate, releasing histamine and other mediators of vasodilation and cellular migration. ●Release of vasoactive substances from stromal mast cells makes small vessels permeable to molecular and cellular mediators of the inflammatory response. The resulting accumulation of plasma and cellular elements is noted clinically as edema, or swelling. ●Chemotaxis results in migration and concentration of polymorphonuclear leukocytes that digest bacteria, foreign debris, and necrotic tissue with lysosomal enzymes.")
9
Phases of Wound Healing
Proliferative 5 days to 3 weeks Granulation New collagen New capillaries Contraction Wounds edges pull together Mediated by myofibroblasts (similar to SM) Epithelialization Cells cross over the moist surface This phase is characterized by the proliferation of fibroblast cells. Collagen matrix stimulates angiogenesis. Granaulation tissue is the result of the combined productions of collagen and growth of capillaries. Epithelialization (also called migration) refers to basal cell proliferation and epithelial migration occurring in the fibrin bridgework inside a clot. Proliferation continues until individual cells are surrounded by cells of similar type. Migration ceases when the layer is rejuvenated; this is normally completed within 48 hours of surgery. The superficial layer of epithelium creates a barrier to bacteria and other foreign bodies. However, it is very thin, easily traumatized, and gives little tensile strength.
 Epithelialization. Cells cross over the moist surface. This phase is characterized by the proliferation of fibroblast cells. Collagen matrix stimulates angiogenesis. Granaulation tissue is the result of the combined productions of collagen and growth of capillaries. Epithelialization (also called migration) refers to basal cell proliferation and epithelial migration occurring in the fibrin bridgework inside a clot. Proliferation continues until individual cells are surrounded by cells of similar type. Migration ceases when the layer is rejuvenated; this is normally completed within 48 hours of surgery. The superficial layer of epithelium creates a barrier to bacteria and other foreign bodies. However, it is very thin, easily traumatized, and gives little tensile strength.")
10
Phases of Wound Healing
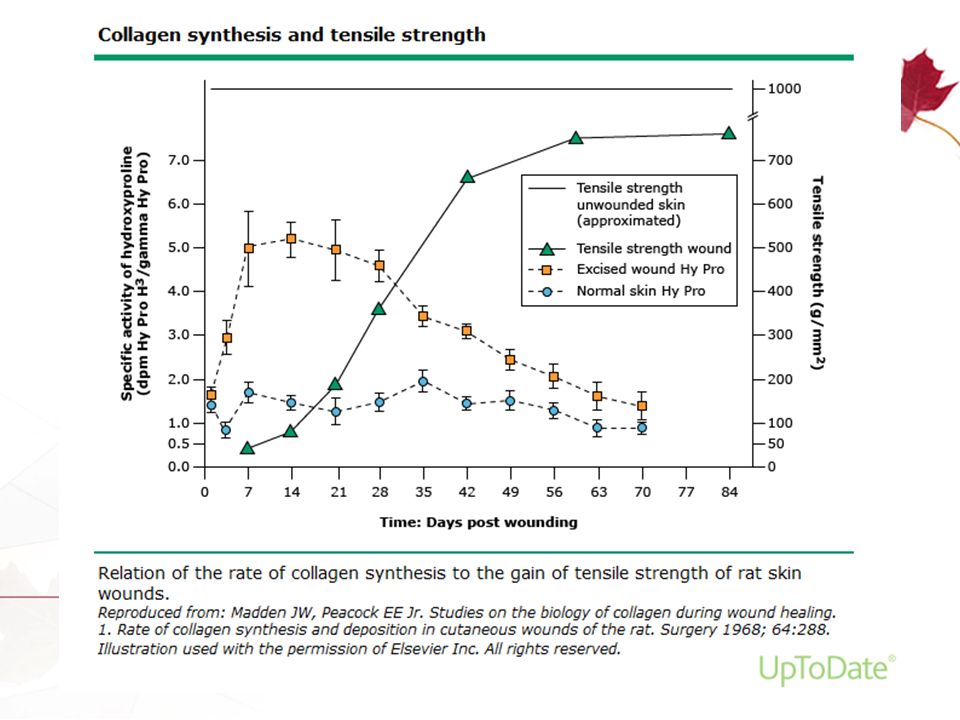
Maturation 3 weeks to 2 years Collagen crosslinks which increases the tensile strength of wounds Scar tissue is only 80% as strong as the original tissue at 6 weeks Normal collagen seen at 180 days Collagen remodeling, wound contraction and repigmentation

13
Impaired Wound Healing
Occurs due to disruption of the phases of healing Local tissue ischemia Neuropathy Tissue necrosis Infection Wound edema As examples, local tissue ischemia and neuropathy can impair chemotaxis during the hemostasis and inflammatory stages. Tissue necrosis and infection alter the balance of inflammation and compete for oxygen. Uncontrolled periwound edema and wound instability disrupt myofibroblast activity, and collagen deposition and cross-linking. >90% are venous ulcers, pressure ulcers, or diabetic wounds

14
Risk Factors for Non-healing Wounds
Peripheral Artery Disease Diabetes Chronic venous insufficiency Aging Immunosuppressive therapy Sickle cell disease Cancer Therapy Radiation therapy Spinal cord disease and immobilization Malnutrition Infection Smoking Certain patients are at risk for development of a non-healing wound such as those with impaired arterial or venous circulation, immunocompromised states, the elderly, those with diabetes, and any patient with neuropathy or spinal cord injury. The most common nonhealing wounds affecting the lower extremities are associated with peripheral artery disease, diabetes and chronic venous insufficiency

15
Wound Management Primary Closure (Primary Intention)
Secondary Closure (Secondary Intention) Delayed Primary Closure (Tertiary Intention)
 Delayed Primary Closure (Tertiary Intention)")
16
Primary Closure Primary closure – The wound edges are apposed with sutures, staples or adhesive tapes (Steri-Strips).
.")
17
Skin & Subcutaneous With primary closure in the operating room, absorbable polyfilament suture material can be used. In the Emergency Room where most wounds have some degree of contamination, non-absorbable monofilament wounds such as nylon or prolene are used. Nylon is the most common. For most purposes 4-0 (read “four-oh”) is best for hands, facial wounds etc. It is tempting, with swelling present, to want to go to a thicker suture such as 2-0 to pull skin edges together. Marginal wound necrosis is rare when 4-0 nylon is used. The suture will simply break if the tension is excessive at the skin edge. Tight sutures can result in strangulation of the dermal skin circulation, necrosis and a much poorer cosmetic result.
 is best for hands, facial wounds etc. It is tempting, with swelling present, to want to go to a thicker suture such as 2-0 to pull skin edges together. Marginal wound necrosis is rare when 4-0 nylon is used. The suture will simply break if the tension is excessive at the skin edge. Tight sutures can result in strangulation of the dermal skin circulation, necrosis and a much poorer cosmetic result.")
18
This is an example of a right total hip replacement wound closed using staples. The trunk is at left and the knee to the right of the screen. It is an example of primary wound closure.

19
Secondary Wound Closure
Spontaneous or “secondary” wound closure. The open wound is not closed by any external mechanism but rather heals by contraction with deposition of scar tissue

20
Secondary Wound Healing
Remember that granulation tissue is teaming with bacteria!!! Skin is a huge organ and prevents bacteria from entering the body. Granulation: Capillary proliferation, leukocytes, bacteria

21
Platelets and Fibrin – Clot, Cytokines
Hemostasis The first step in secondary or spontaneous healing is the formation of a clot. Platelets and Fibrin – Clot, Cytokines

22
PMN’s and macrophages Inflammation
The clot dries and forms a protective scab or eschar. Sequential migration of leukocytes into wound. Wound is populated within 24 hours. Followed by macrophages. Cytokines are released. PMN’s and macrophages

23
Macrophages attract fibroblasts New connective tissue matrix
Fibroplasia This is the phase which is most important to a surgeon or ER physician. Fibroplasia increases wound strength. Wound collagen synthesis begins within 10 hours of injury and peaks by 5 to 7 days following injury (remember 5 days on a facial wound due to excellent blood supply). Blood vessels also proliferate locally. Macrophages attract fibroblasts New connective tissue matrix
. Blood vessels also proliferate locally. Macrophages attract fibroblasts. New connective tissue matrix.")
24
Maturation Inflammatory cells decrease, angiogenesis stops,
With remodelling, the inflammatory cells disappear, angiogenesis is discontinued and collagen synthesis falls into equalibrium. Inflammatory cells decrease, angiogenesis stops, Equalization of collagen synthesis & degradation

25
Contraction Ancient peoples: Skin wounds heal & contract
Powerful mechanical forces in the body Ancient peoples: Skin wounds heal & contract if kept clean & protected with a dressing Skin margins move together to produce a healed wound Contraction can yield a devastating result in some injuries ie. burns Contraction of a wound by way of secondary wound healing is a very powerful force. It is still used with great success in many clinical situations.

26
Excision & Full Thickness Skin Grafting
Severe Contracture This type of wound contraction can have a deleterious clinical outcome, as in the case of this child who sustained a full-thickness burn to the anterior neck and upper chest wall. The mouth is held open by thick fibrotic skin. Split thickness skin grafts are not generally used in this area because they tend to contract much more than full thickness skin. When full thickness skin is harvested, it contracts by up to 40 % immediately as it is detached from its durrounding skin. But, thereafter there is very little or no contraction. The child in this slide has undergone plastic surgical reconstruction with full thickness skin grafting. Full thickness skin grafts are somewhat more challenging from a technical stand-point. Any serum or blood which collects under the full thickness skin will lift it off and impair neovascularization. Split thickness skin graft is meshed to allow blood and serum to drain. Plastic surgeons avoid the problem of graft lift-off by using a 15 scalpel blade to make perforations in full thickness skin and tying down bolsters which apply gentle pressure over the surface of the full thickness skin. Excision & Full Thickness Skin Grafting

27
This young man was involved in a motorcycle accident many years years ago. He sustained an abrasion type wound from the socket of his below knee prosthesis. Contraction of the wound with secondary healing is beneficial.

28
These are the lateral and AP views of his residual limb
These are the lateral and AP views of his residual limb. The distal tip of the tibia was “pencil-tipped” and the sharp tip was excised to prevent recurrence of the wound. Try to zoom in on the distal tip of the tibia to get a closer look.

29
Delayed Primary Closure
Beware in the ER that you do not bow to the pressure to close a wound. Patients may feel they are not being treated appropriately when a wound is kept open and not sutured. They respond well to a simple explanation regarding wound principles. If there is dirt in the wound, debride it and arrange for a 24 hour check-up. Antibiotics are prescribed. Delayed wound closure is possible at 48 hours if the 24 and 48 hour assessments reveal no sign of infection. It is important to remember that if a wound has been open for more than 12 hours, bacteria have been multiplying every 7 minutes or so since the injury and the risk of deep infection increases. It is best to debride these wounds. Redebride at 24 to 48 hours and consider delayed primary closure when suitable generally at about 48 hours. Remember, it takes 48 hours to make pus. Wound is left open due to gross contamination

30
Delayed Primary Closure
The wound is allowed to remain open for several days to ensure all contamination is removed. A redebridement in the operating room can also be carried out at 24 to 48 hours to decrease the bacterial load in the wound. Sometimes many debridements are necessary in the case of an oil injection gun injury where the initial extent of injury and chemical contamination is not evident.

31
Delayed Primary or Secondary Closure But Never Primary Closure
This is a characteristic medial ankle open fracture wound. The medial malleolus has torn the skin open as lateral talar shift occurred. Note that hemorrhage is the first stage of wound healing and that coagulation has not yet occurred. An open fracture is an acute surgical emergency and the goal is to get the patient to the OR as soon as possible. The natural history of an untreated open fracture is osteomyelitis. Open Fracture Wounds Delayed Primary or Secondary Closure But Never Primary Closure

32
Here is the accompanying AP ankle x-ray
Here is the accompanying AP ankle x-ray. Note the marked widening of the medial clear space. The displaced distal fibular fracture is difficult to see but look closely. The anterior and posterior fracture surfaces are seen (small arrows).
.")
33
Since this is an intra-articular fracture, the medial wound is debrided and irrigated. A lateral incision allows open reduction internal fixation (ORIF). An interfragmentary screw does all the work and neutralizing plate prevents rotational forces from pulling the interfragmentary screw out. Normally, antibiotics would be given intravenously for 48 hours. The cast would be changed while in hospital to make sure there is no sign of erythema, purulent drainage, etc. The patient would be discharged with a cast in place for another cast change at 5 days post-surgery. Weekly cast-changes are carried out until 4 weeks, at which time a below knee walking cast or walking boot is applied. The walking boot would be used for a further 2 weeks, full weight-bearing.
. An interfragmentary screw does all the work and neutralizing plate prevents rotational forces from pulling the interfragmentary screw out. Normally, antibiotics would be given intravenously for 48 hours. The cast would be changed while in hospital to make sure there is no sign of erythema, purulent drainage, etc. The patient would be discharged with a cast in place for another cast change at 5 days post-surgery. Weekly cast-changes are carried out until 4 weeks, at which time a below knee walking cast or walking boot is applied. The walking boot would be used for a further 2 weeks, full weight-bearing..")
34
Wound Complications Early Late Seroma/Hematoma Dehiscence Infection
Hernia Hypertrophic and Keloid Scars Hypertrophic scar Keloid formation Necrosis Abscess

35
Seroma and Hematoma Seroma Hematoma Collection of serous fluid
Fluctuation, swelling, redness, tenderness TREATMENT: Sterile punture and compression Suction drain Collection of blood –Bleeding, anticoagulant Risk of infection Swelling, fluctuation, pain, redness TREATMENT Sterile puncture Surgical exploration

36
Wound Dehiscence Complete breakdown of the wound closure
Systemic Risk Factors: Diabetes, Malnutrition, obesity, COPD, steroids, cytotoxic drugs Local Risk factors: Technical error, infection, hematoma, ischemia, radiation

37
VAC Assisted therapy designed to promote the formation of granulation tissue for faster healing in the wound beds of patients with acute and chronic wounds Uses topical negative pressure - removes extracellular fluid and exudate, reduces edema and improves blood flow, thereby providing oxygenation and nutrition to a wound site

39
Skin does not grow over exposed dead bone
This is important to remember. In general, skin graft can be placed over granulation tissue which has proliferated on healthy bleeding cancellous bone. This situation is not ideal though because the risk of developing osteomyelitis is much higher. Muscle flaps (either rotation or free transplants) are placed over the bone and split thickness skin placed on the muscle.
 are placed over the bone and split thickness skin placed on the muscle.")
40
Gastrocnemius Rotation Flap
Patella This man was out on a fishing trip with his buddies. The boat docked. He jumped out of the boat but lost his balance. He fell into the water while the propellor of the outboard motor was still going. A severe open tibia fracture occurred. Exposed cancellous bone can be seen at the small white arrow. A medial gastrocnemius flap (large block arrow) covers this area. The entire wound was covered with split-thickness skin graft and the wound and fracture healed. 70 yr. old male 3B Prox. tibia Prop injury Right: Lateral View
 covers this area. The entire wound was covered with split-thickness skin graft and the wound and fracture healed. 70 yr. old male. 3B Prox. tibia. Prop injury. Right: Lateral View.")
41
Superficial (Cortical) Osteo
Patella Patella Left Tibia This man has multiple draining sinuses from a 40 year old chronic osteomyelitis. He was managing well for his entire life until a supra-infection resulted in the development of a very foul, pungent odour. His spouse was unable to cope with the odour. Surgical excision of fibrous, indurated skin was carried out and deep debridement of the tibia performed. Osteomyelitic bone was removed and the defect covered with a medial gastrocnemius rotation flap. A split thickness skin graft is placed over the muscle. STSG cannot be placed reliably or with great success over bone. It can adhere to bleeding cancellous bone but the skin is very delicate and easily scraped/traumatized. Typically, medial aspect proximal tibia Medial gastrocnemius is “workhorse”

42
Gastrocnemius Muscle: Vascular Supply
Lateral sural artery Medial sural artery A medial gastrocnemius flap is based on the medial sural artery. Therefore, the muscle is rotating on this vascular pedicle. Branches of popliteal artery

43
Gastrocnemius Rotation Flap
Medial goes farther Midline defect Femoral condyles Key is to take a slip of distal tendon The medial flap reaches a little further. When such a flap is healing, remember that the 4 stages of wound healing are at play. Remodelling will take up to a year and is characterized by fading of the skin from red/pink to whitish or white-pink. Medial Lateral

44
This is a 70 year old female who underwent total knee replacement at another hospital 4 months ago. Wound necrosis occurred. The wound was described as being filled with “good granulation tissue”. Remember that granulation tissue is filled with bacteria, leukocytes and capillary buds. The presence of bacteria in close proximity to a prosthesis is of major concern.

45
Here is a close-up view. Palpation with the tip of a sterile forcep would reveal that the patella is directly beneath the white fibrin-covered “ring” indicated to the left.

46
Your suspicions are correct. The CBC reveals a WBC (white count of 10
Your suspicions are correct. The CBC reveals a WBC (white count of 10.5) and the erythrocyte sedimentation rate (ESR) is 65 (normal less than 10). The radiolucency seen at the yellow area is occurring as a result of deep infection. This type of finding wound occur with aseptic polyethylene wear after 6 to 10 years, not 4 months. So, the prosthesis needs to come out.
 and the erythrocyte sedimentation rate (ESR) is 65 (normal less than 10). The radiolucency seen at the yellow area is occurring as a result of deep infection. This type of finding wound occur with aseptic polyethylene wear after 6 to 10 years, not 4 months. So, the prosthesis needs to come out.")
47
This is the appearance of the knee on exposing it
This is the appearance of the knee on exposing it. The patellar button is seen on the partially everted patella, immediately above the 6-prong rake. There was no frank pus but the patient had been placed on antibiotics at the referring hospital without a clear organism having been identified. The tissue at the centre of the wound is infective synovium, organizing hematoma and required excision.

48
Antibiotic-Loaded Acrylic Cement Spacer Block
The implants have been removed and the bone debrided. An antibiotic-loaded methylmethcrylate (acrylic bone cement) spacer block is placed to keep the collateral ligaments from contracting for the 6 to 8 weeks of IV antibiotic therapy required prior to 2nd stage revision knee prosthesis re-implantation. Note the patellar component has been removed and 3 indentations are evident in the patella. Antibiotic-Loaded Acrylic Cement Spacer Block
 spacer block is placed to keep the collateral ligaments from contracting for the 6 to 8 weeks of IV antibiotic therapy required prior to 2nd stage revision knee prosthesis re-implantation. Note the patellar component has been removed and 3 indentations are evident in the patella. Antibiotic-Loaded Acrylic Cement Spacer Block.")
49
These AP and lateral views show the antibiotic cement spacer in place
These AP and lateral views show the antibiotic cement spacer in place. Some orthopaedic surgeons refer to this as a “hockey puck” but actually there are prongs which extend superiorly and inferiorly into the medullary canal of the femur and tibia respectively which help to keep it in place. The patient’s knee is placed in a velcro knee splint for skin care but, obviously, knee range of motion is not possible.

50
Right Knee-Calf: Medial View

51
The anterior soft tissue envelop was not very good, so a medial gastrocnemius rotation flap is elevated. This is the medial view with the muscle exposed.

52
In this view, the medial gastrocnemius flap has been elevated and rotated beneath an anteromedial skin bridge. The distal end of the muscle has been detached and is being held using 3 Allis clamps. The soleus muscle is now visible with its fascial covering in the deep portion of the wound (blue arrow). The Metzenbaum scissors are pointing at a minor vascular pedicle which is entering the muscle from its posterior boder. It could be ligated if necessary to further mobilize the muscle. The main blood supply comes from the medial sural artery, a branch of the popliteal artery and passes down the centre of the muscle
. The Metzenbaum scissors are pointing at a minor vascular pedicle which is entering the muscle from its posterior boder. It could be ligated if necessary to further mobilize the muscle. The main blood supply comes from the medial sural artery, a branch of the popliteal artery and passes down the centre of the muscle.")
53
Right Knee Lateral View
Ankle This is the corresponding anterolateral view which shows the Allis clamps on the distal tendon slip of the medial gastrocnemius muscle.

54
8 Weeks Later – IV Antibiotics
Right Knee This is the appearance of the skin-grafted flap almost completely healed. It is taken immediately before resection of the antibiotic spacer and placement of a revision knee prosthesis. What type of healing is occurring at the periphery. Note that every orthopaedic patient must have the operative extremity signed by the surgeon, fellow or resident prior to coming into the operating theatre. This is also an extremely useful practice for other surgical specialties such as urology (nephrectomy for tumour). Type of Healing Here? 8 Weeks Later – IV Antibiotics
. Type of Healing Here 8 Weeks Later – IV Antibiotics.")
55
This is the revised knee with stemmed components
This is the revised knee with stemmed components. The patient’s wound has been closed with skin staples. See them on the x-ray? She returned at her one month and 3 month visit complaining bitterly of anterior knee pain and stiffness. Is this surprising? Think about the fibroblast proliferation which occurred in response to the muscle flap, skin graft and one resection surgery and one revision implant surgery. By her 6 month visit, the wounds were fading from pink to white in some areas and her pain was improving. She felt better since her wound was entering the remodelling phase of healing.

56
Flap Options Gastrocnemius rotation flaps are used to cover defects of the proximal 1/3 to ½ of tibia. Latissimus dorsi free flaps are used for large defects, rectus abdominis for medium sided defects. Remember that the pluripotential cells from the muscle flap will stimulate fibroblast proliferation at the base of every wound.

57
Infection Superficial versus deep? Superficial wound infection:
Treatment: Antibiotics Deep wound infection: Treatment: identify organism with cultures surgical exploration (irrigation and debridement) IV antibiotics based on cultures and ID consultation
 IV antibiotics based on cultures and ID consultation.")
58
Wound Debridement Gentle handling of tissues minimizes bleeding
Control residual bleeding with compression, ligation or cautery Dead or devitalized muscle is dark in color, soft, easily damaged and does not contract when pinched. During debridement, excise only a very thin margin of skin from the wound edge

59
Wound Debridement Debride the wound meticulously to remove any loose foreign material such as dirt, grass, wood, glass or clothing. With a scalpel or dissecting scissors, remove all adherent foreign material along with a thin margin of underlying tissue and then irrigate the wound again. Continue the cycle of surgical debridement and saline irrigation until the wound is completely clean. Leave the wound open after debridement to allow healing by secondary intention. Pack it lightly with damp saline gauze and cover the packed wound with a dry dressing. Change the packing and dressing daily or more often if the outer dressing becomes damp with blood or other body fluids. Large defects will require closure with flaps or skin grafts but may be initially managed with saline packing

60
Hypertrophic and Keloid Scars
Excessive tissue response to dermal injury characterized by local fibroblast proliferation and overproduction of collagen Overexpression of growth factors, such as transforming growth factor-beta (TGF-beta), vascular endothelial growth factor (VEGF), and connective tissue growth factor (CTGF) Keloids and hypertrophic scars represent an excessive tissue response to dermal injury characterized by local fibroblast proliferation and overproduction of collagen
, vascular endothelial growth factor (VEGF), and connective tissue growth factor (CTGF) Keloids and hypertrophic scars represent an excessive tissue response to dermal injury characterized by local fibroblast proliferation and overproduction of collagen.")
61
Hypertrophic Scars Sites of surgical wounds, lacerations, burns, or inflammatory or infectious skin conditions (eg, acne, folliculitis, chicken pox, and vaccinations). They are raised, may be erythematous, and typically do not exceed the margins of the original wound Hypertrophic scars usually show a rapid growth phase of up to six months, followed by possible regression over the following 12 to 18 months.
. They are raised, may be erythematous, and typically do not exceed the margins of the original wound. Hypertrophic scars usually show a rapid growth phase of up to six months, followed by possible regression over the following 12 to 18 months.")
63
Keloid Scars Raised dermal lesions that extend beyond the boundaries of the original wound and invade the surrounding healthy skin Sites of minor injuries to the skin, such as earlobe piercings, or may develop in the absence of an obvious inciting stimulus In contrast with hypertrophic scars, keloids do not regress spontaneously but enlarge progressively over time

64
Keloids occur more frequently in certain ethnic populations; people of African and Asian descent are most susceptible to the development of keloids Pain and pruritus are frequently associated symptoms. Full-thickness burn injuries impair or destroy hair follicles, sweat glands, sebaceous glands, capillaries, and nerve endings, leading to loss of temperature regulation, dry skin, and neuropathic pain. These scars may also cause functional impairment from contracture or mechanical irritation.

65
Treatment of Hypertrophic and Keloid Scars
Intralesional Cortisone injection Silicone gel sheets Pressure therapy Cyrotherapy Surgical Excision Surgical excision of hypertrophic scars and keloids may be indicated if conservative therapies alone are unsuccessful or unlikely to result in significant improvement. Surgical excision of keloids is associated with recurrence rates of up to 100 percent. The combination of surgery with adjunctive perioperative therapies can significantly lower the risk of recurrence

66
Thank You

Similar presentations