Download presentation
Presentation is loading. Please wait.

1
Treatment of Fracture by Dr. Nimer Khraim DVMS, BVMS, MVSc, PhD(Dr.med.vet)
")
2
Treatment of Fracture Immediate treatment Control h. Control h. Prevent infection Prevent infection Control pain Control pain Treat shock Treat shock

3
Treatment of Fracture Temporary immobilization To prevent further soft T. damage To prevent further soft T. damage

4
Treatment of Fracture The basic principle of fracture treatment include: Accurate reduction Accurate reduction Stable fixation Stable fixation Preservation of blood supply and early return to function Preservation of blood supply and early return to function

5
Treatment of Fracture Accurate reduction Close reduction by manipulation Close reduction by manipulation The fragment are angulated until one cortex of each fragment are touching The fragment are angulated until one cortex of each fragment are touching The limb is then gradually extended to overcome the muscle spasm and over- righting The limb is then gradually extended to overcome the muscle spasm and over- righting

6
Treatment of Fracture Open reduction its indications: Failure to a chief reduction by close manipulation Failure to a chief reduction by close manipulation Intra-articular fracture Intra-articular fracture

7
Treatment of Fracture Distracted fracture Distracted fracture Delay union, mal-union or non-union Delay union, mal-union or non-union Application to internal fixation Application to internal fixation

8
Treatment of Fracture Immobilization The ideal fixation of fracture should be Maintain stable reduction Maintain stable reduction Not interfere with blood supply Not interfere with blood supply

9
Treatment of Fracture Allow free range of movement Allow free range of movement Chief Chief Removable Removable

10
Treatment of Fracture There is tow type of fixation Internal fixation Internal fixation External fixation External fixation

11
Internal Fixation

12
Internal fixation Rigid fixation Rigid fixation Adequate reduction Adequate reduction Impossible to maintain an acceptable position by external fixation Impossible to maintain an acceptable position by external fixation External fixation will not be tolerate External fixation will not be tolerate

13
Type of internal fixation

14
Intramedullary pinning

15
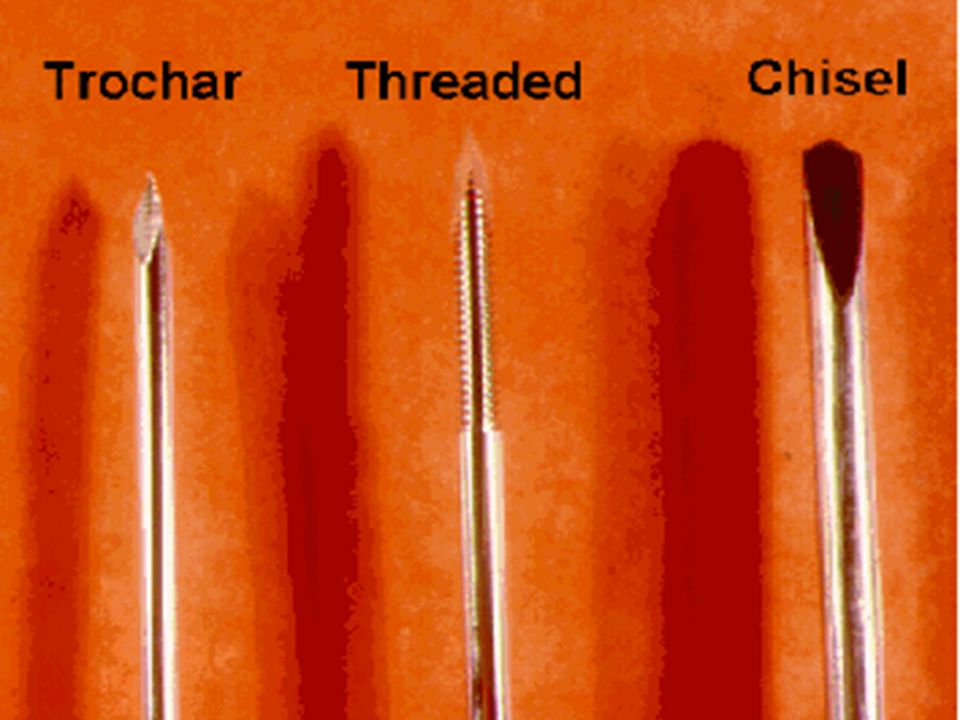
Type of internal fixation Intramedullary pinning Commonly use round pin like Steinmann pin, kirschner pin, rush pin Commonly use round pin like Steinmann pin, kirschner pin, rush pin

17
Intramedullary pinning The pin should be approximately the diameter of morrow cavity at the fracture site The pin should be approximately the diameter of morrow cavity at the fracture site Fixation of pin to both end of the bone with impingment of the inner surface of the cortex at the fracture site Fixation of pin to both end of the bone with impingment of the inner surface of the cortex at the fracture site

18
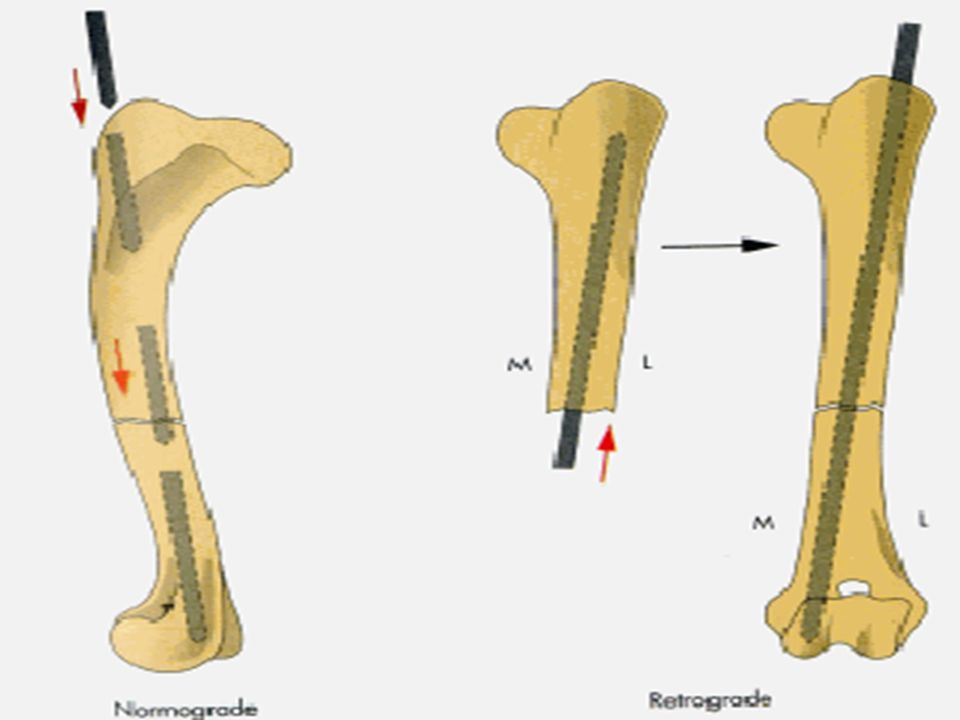
Intramedullary pinning Fracture that is readily palpation and reduction Fracture that is readily palpation and reduction In open method a pin may inserted through the end of the bone or retrograde direction from the fracture site In open method a pin may inserted through the end of the bone or retrograde direction from the fracture site

20
Intramedullary pinning Protruding end of the pin is cut enough to baired under the skin and soft T. Protruding end of the pin is cut enough to baired under the skin and soft T. The pin is remove when the clinical union has been a chief The pin is remove when the clinical union has been a chief

21
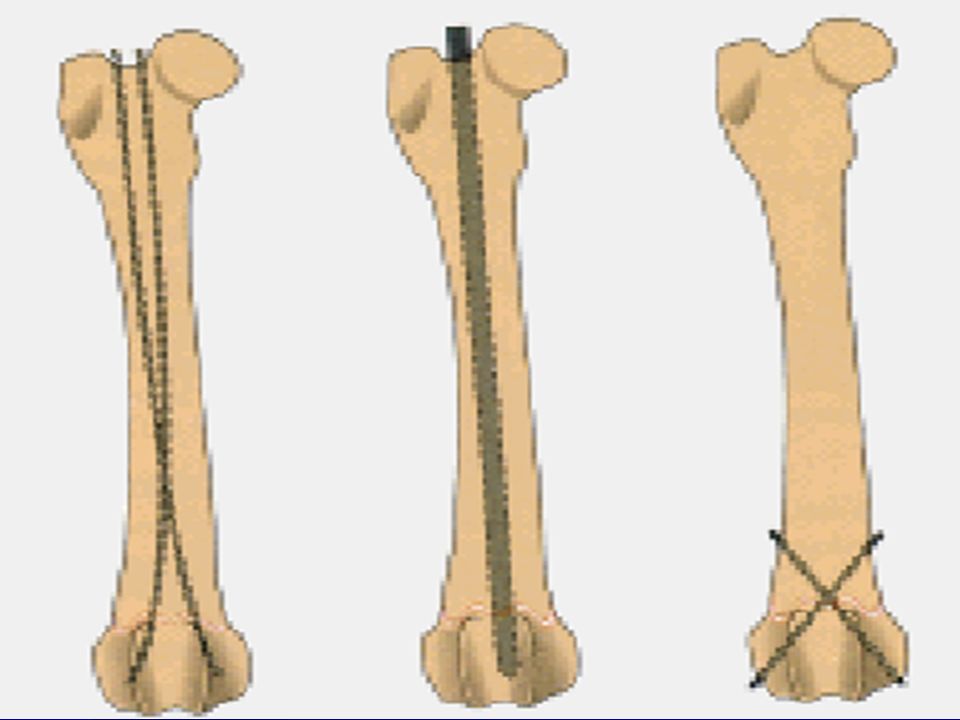
Intramedullary pinning Inter medullary pinning dose not provide sufficient stability Inter medullary pinning dose not provide sufficient stability fixation medullary fixation that include fixation medullary fixation that include

22
Intramedullary pinning Wire Wire Kirschner splint Kirschner splint 2 pin or more 2 pin or more Screw Screw In large animal cast or splint to prevent blent of pin In large animal cast or splint to prevent blent of pin

25
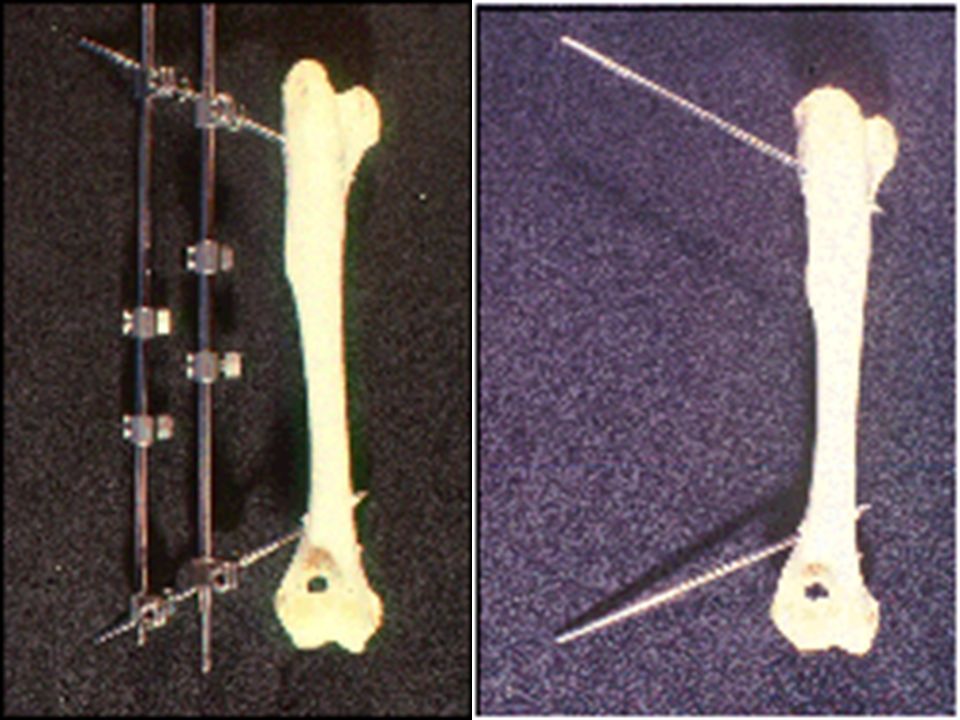
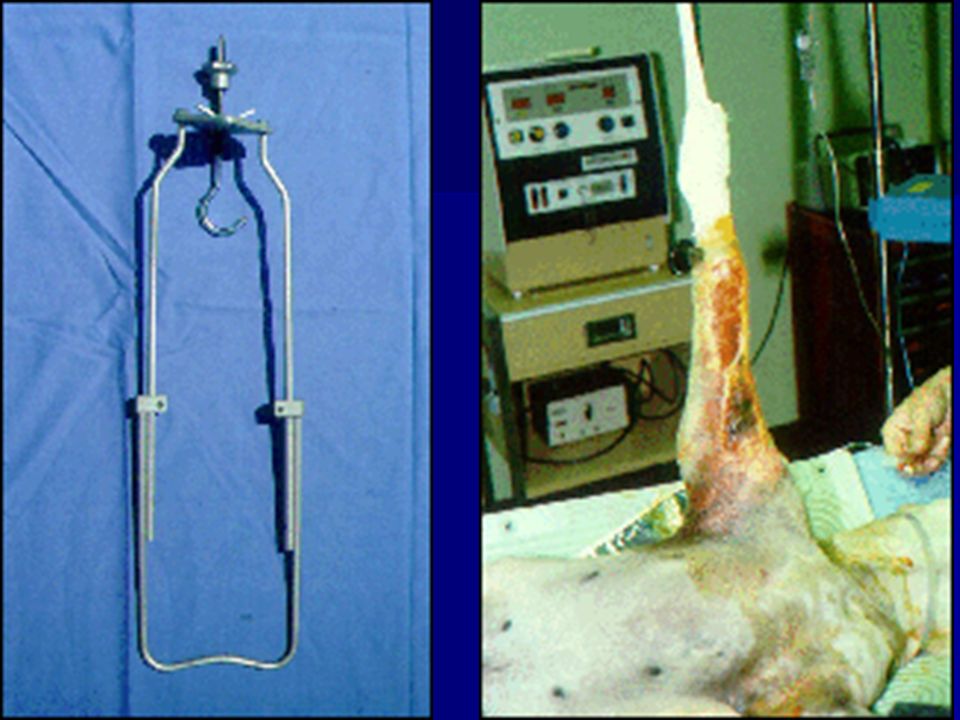
Intramedullary pinning Kirshner splint (Kirshner Ehmer splint) Insert 2 pin in proximal and distal bone segment and the pin connected by external bar Insert 2 pin in proximal and distal bone segment and the pin connected by external bar The splint may be apply following close or open reduction using pin-chuck to drill the both cortex The splint may be apply following close or open reduction using pin-chuck to drill the both cortex
 Insert 2 pin in proximal and distal bone segment and the pin connected by external bar Insert 2 pin in proximal and distal bone segment and the pin connected by external bar The splint may be apply following close or open reduction using pin-chuck to drill the both cortex The splint may be apply following close or open reduction using pin-chuck to drill the both cortex")
27
Kirshner splint The 2 pin in each segment are inserted at approximately 34 to 40 degree into each other The 2 pin in each segment are inserted at approximately 34 to 40 degree into each other as healing approach the stage of clinical union it may be tested by removing the bar and gentile bending the bone to determine the strength of the callus as healing approach the stage of clinical union it may be tested by removing the bar and gentile bending the bone to determine the strength of the callus

31
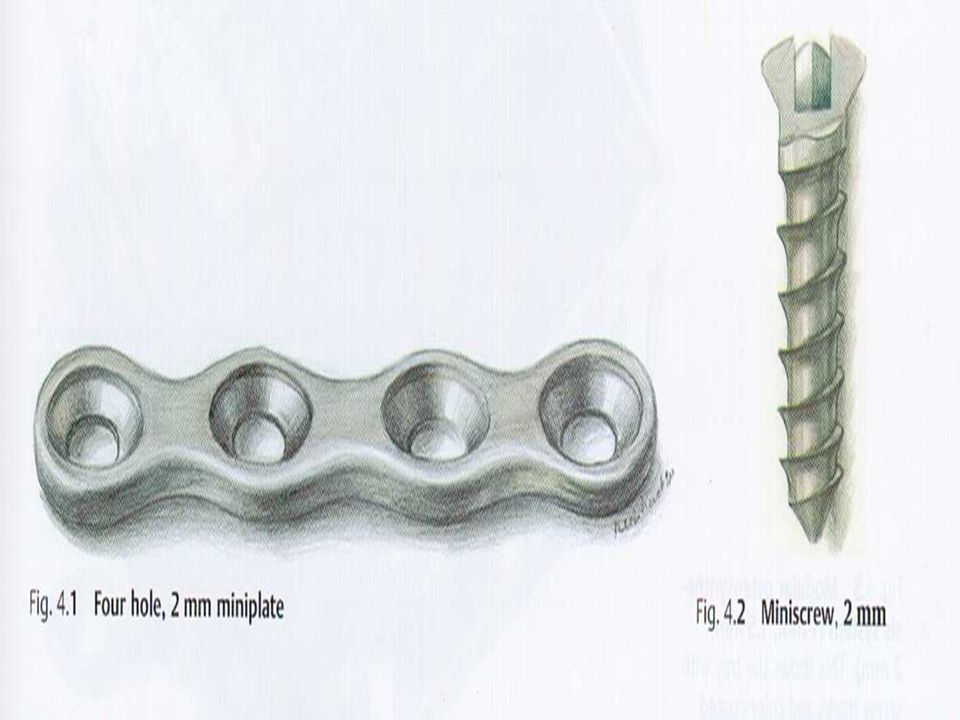
Bone plate

32
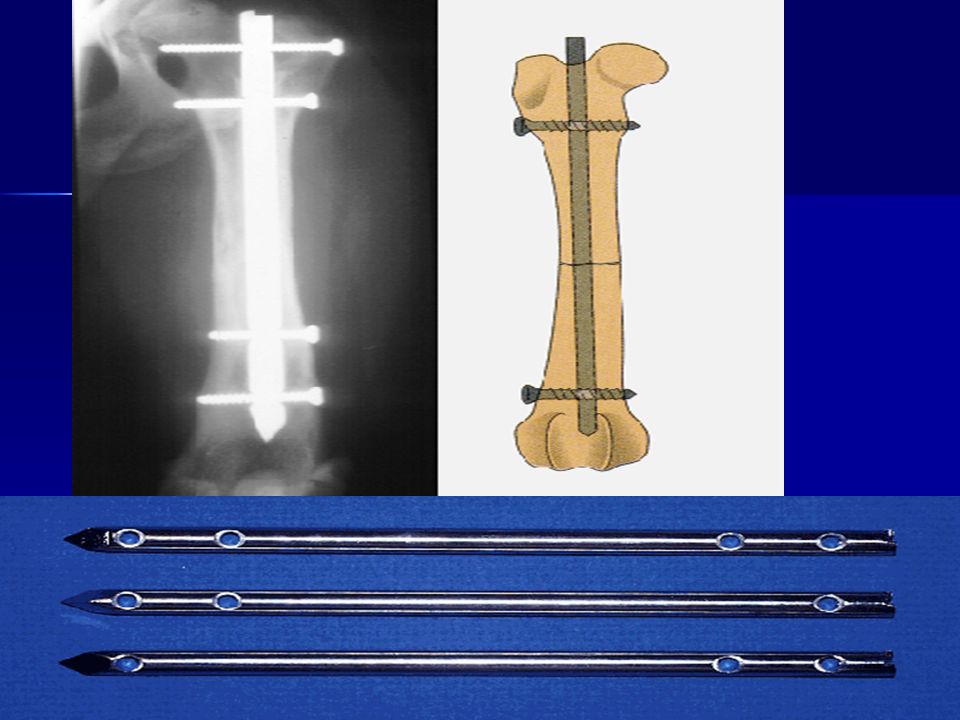
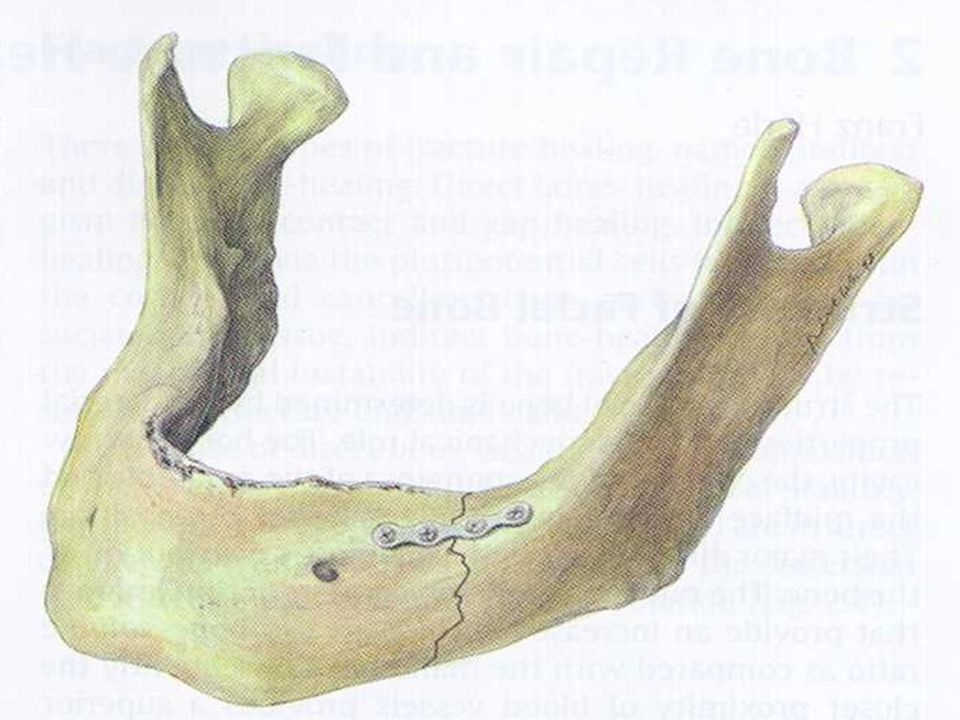
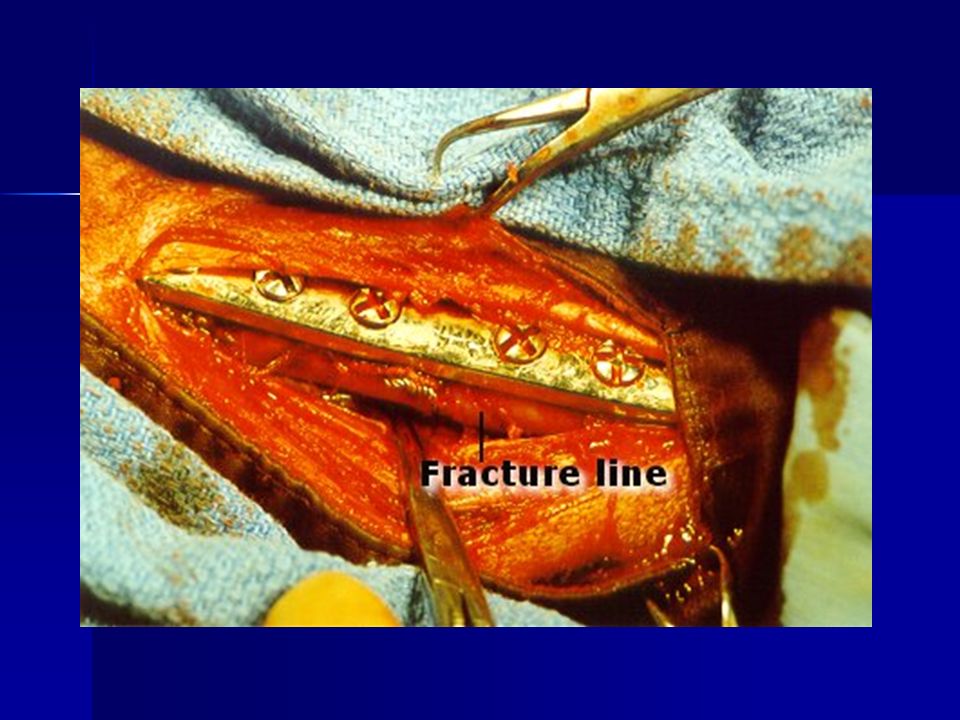
The technique provide rigid internal fixation which eliminate all shortening rotation and angular forces at the fracture The technique provide rigid internal fixation which eliminate all shortening rotation and angular forces at the fracture

33
Bone plate Its type are: Compression bone plate insertion under tension Compression bone plate insertion under tension Neutralizing bone plate insertion not under tension Neutralizing bone plate insertion not under tension Bridging bone plate used to short up a gap in the bone Bridging bone plate used to short up a gap in the bone

34
Bone plate Buttress bone plate: holdup one cortex relative to the other mainly use in epiphyseal and metaphysical fracture Buttress bone plate: holdup one cortex relative to the other mainly use in epiphyseal and metaphysical fracture Dynamic compression bone plate used in any of these method Dynamic compression bone plate used in any of these method

37
The basic principle in application of bone plate and screw

38
Bone plate One of the most stable forms of fracture fixation. One of the most stable forms of fracture fixation. Loaded bones have compression and tension sides. Loaded bones have compression and tension sides. Bone plates should be applied to the tension side of a bone to provide maximum stability. Bone plates should be applied to the tension side of a bone to provide maximum stability.

39
Bone plate Clinically these surfaces are the lateral side of the femur, medial or cranial surface of the tibia, cranial or lateral surface of the humorous, and the cranio-medial or cranial surface of the radius. Clinically these surfaces are the lateral side of the femur, medial or cranial surface of the tibia, cranial or lateral surface of the humorous, and the cranio-medial or cranial surface of the radius.

40
Bone plate Bone plates are capable of neutralizing compression, tension, shear, bending and torsion forces. Bone plates are capable of neutralizing compression, tension, shear, bending and torsion forces. The bending stiffness of a plated bone is related to the length of the plate; the longer the plate the greater the stiffness. The bending stiffness of a plated bone is related to the length of the plate; the longer the plate the greater the stiffness.

41
Bone plate Filling all screw holes with screws improves the strength and stiffness of a plate. Filling all screw holes with screws improves the strength and stiffness of a plate. The use of wider and/or thicker plates can enhance a plate’s ability to counteract the disruptive forces. The use of wider and/or thicker plates can enhance a plate’s ability to counteract the disruptive forces.

42
Bone plate Dynamic Compression Plate (DCP) Dynamic Compression Plate (DCP) –A plate applied to a bone so that it is under tension and the fracture fragments are under compression.
 Dynamic Compression Plate (DCP) –A plate applied to a bone so that it is under tension and the fracture fragments are under compression.")
43
Bone plate –As the screw is tightened the fragment into which it is being placed is displaced toward the fracture line and the center of the plate.

44
Bone plate –By alternate tightening of “loaded” screws on each side of a fracture line the fragments are compressed.

45
DCP Types

46
Narrow DCP: the width of the plate is just slightly greater than the screw holes and the holes are arranged in a straight line.

49
DCP Types Broad DCP: the plate is considerably wider than the screw holes; the holes may be in a straight line or staggered, and the plate is thicker than a narrow DCP.

51
DCP Types Limited contact DCP: Not all of the surface of the plate is in contact with the bone.

53
Special Plates

54
C-shaped plates for dorsal acetabular fractures C-shaped plates for dorsal acetabular fractures T-shaped plates have a variety of applications including distal radial fractures and certain types of arthrodesis T-shaped plates have a variety of applications including distal radial fractures and certain types of arthrodesis

57
Special Plates Cuttable plates. They can be cut to the specific length needed and can be stacked one on the other if additional strength is needed. Cuttable plates. They can be cut to the specific length needed and can be stacked one on the other if additional strength is needed.

60
Plate Function

61
Neutralization plate: is applied to the tension side of a fractured bone. Neutralization plate: is applied to the tension side of a fractured bone. Buttress plate: The plate is placed to span or bridge a fractured area to maintain length when fragments are left unreduced or are missing and replaced with a cancellous bone graft. Buttress plate: The plate is placed to span or bridge a fractured area to maintain length when fragments are left unreduced or are missing and replaced with a cancellous bone graft.

62
Plate Application

63
Plates are placed on the tension side of a long bone and secured to the bone with bone screws.Plates are placed on the tension side of a long bone and secured to the bone with bone screws. A minimum of 3 to 4 screws must be placed on each side of a fracture for a compression, neutralization or bridging plate.A minimum of 3 to 4 screws must be placed on each side of a fracture for a compression, neutralization or bridging plate.

68
Plate Application Screws are placed so they engage both cortices of the bone.Screws are placed so they engage both cortices of the bone. The minimum distance between a screw and a fracture line should be between 4 and 5 mm.The minimum distance between a screw and a fracture line should be between 4 and 5 mm.

72
Plate Application Long plates are more effective than short plates in neutralizing disruptive forces.Long plates are more effective than short plates in neutralizing disruptive forces. The ideal in most cases is to use a plate that is just short of the entire length of the bone.The ideal in most cases is to use a plate that is just short of the entire length of the bone.

73
Plate Application The plate must be in contact with and conform to the shape of the bone to which it is being applied. The plate must be in contact with and conform to the shape of the bone to which it is being applied. Plates are bent or twisted so that they can fit the contours of a bone. Plates are bent or twisted so that they can fit the contours of a bone. The bends and twists must be placed between the screw holes. The bends and twists must be placed between the screw holes.

77
CERCLAGE OR HEMICERCLAGE WIRE

78
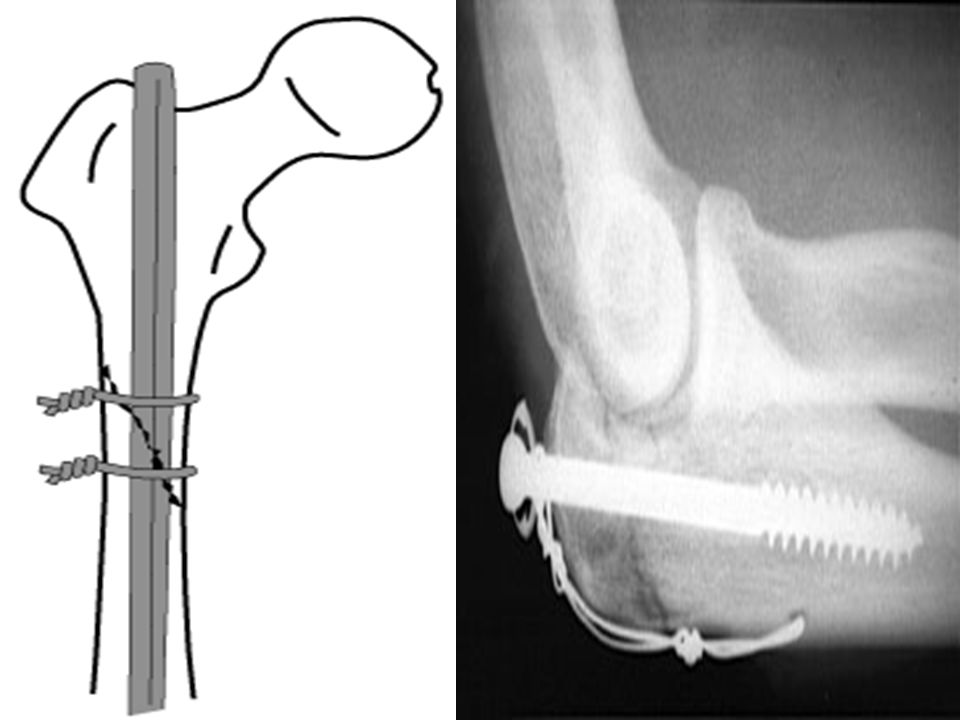
Circle of wire that completely or partially goes around the circumference of a bone Circle of wire that completely or partially goes around the circumference of a bone They are not used as sole method of repair or fixation in any type of fracture They are not used as sole method of repair or fixation in any type of fracture

80
CERCLAGE OR HEMICERCLAGE WIRE Indications Long oblique, spiral & comminuted Fr Long oblique, spiral & comminuted Fr For auxillary fixation For auxillary fixation

81
CERCLAGE OR HEMICERCLAGE WIRE Use wires of sufficient strength 10, 20,22 gauge Use wires of sufficient strength 10, 20,22 gauge Apply tightly Apply tightly

82
CERCLAGE OR HEMICERCLAGE WIRE Space them about l cm apart & 0.5 cm from Fr. line Space them about l cm apart & 0.5 cm from Fr. line Never use less than 2 wires Never use less than 2 wires

83
Screws

84
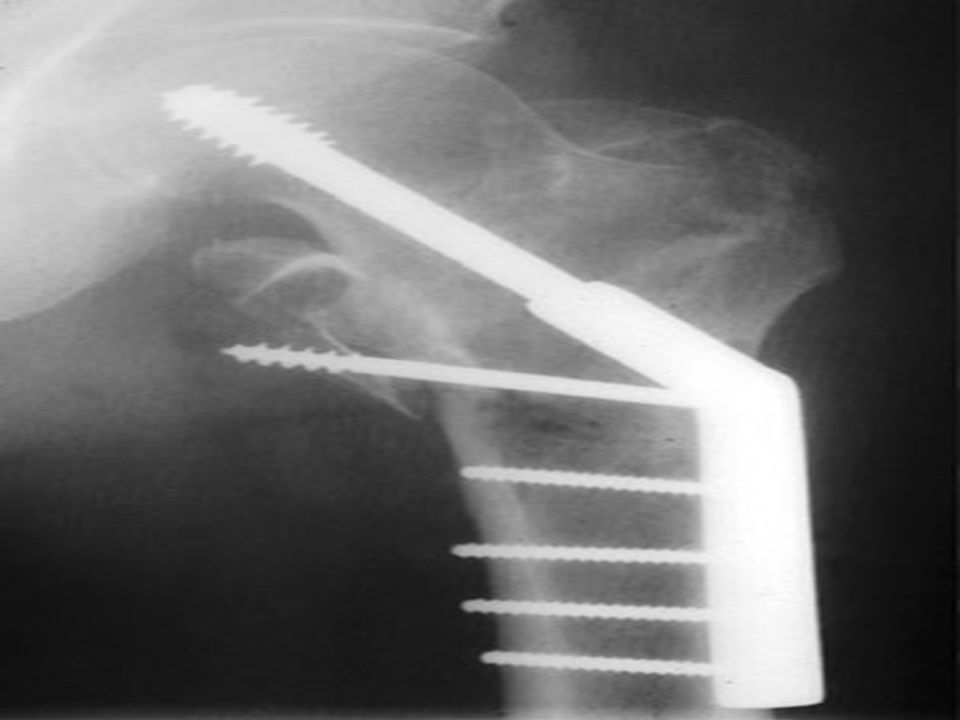
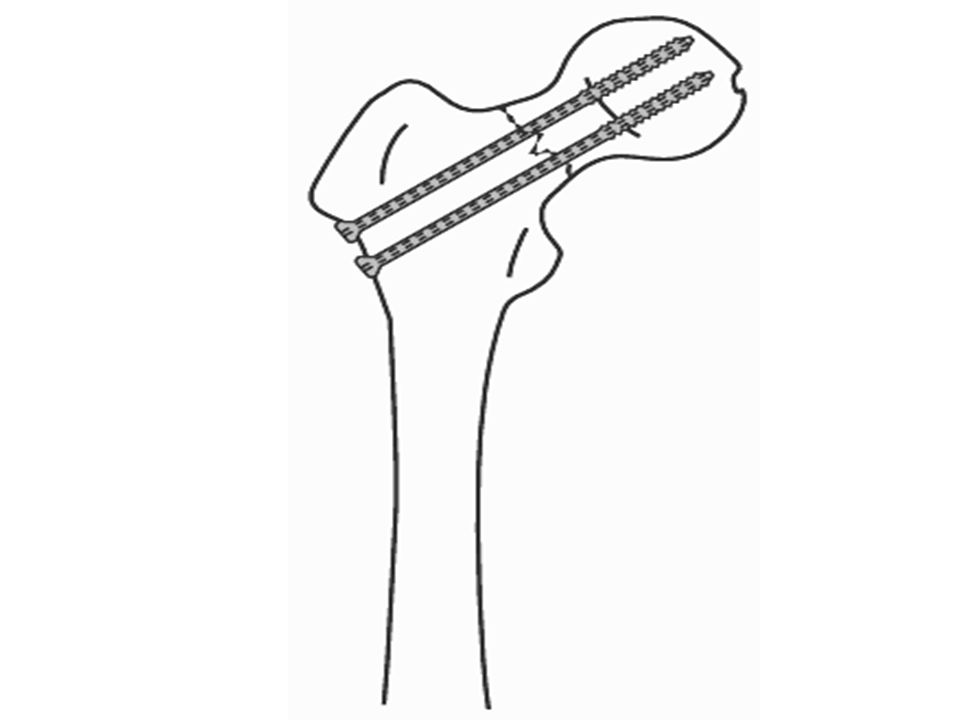
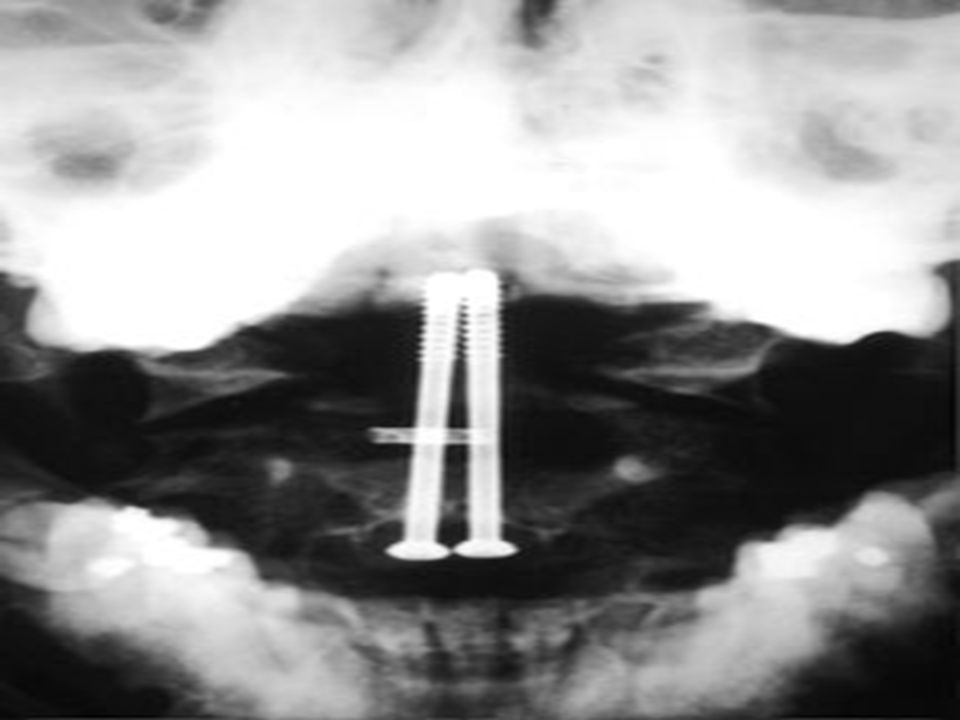
Screws INDICATIONS INDICATIONS –Screws can be used by themselves for fractures of the femoral neck and for intercondylar fractures of the distal humerus and femur.

87
Screws In these situations one screw is often used together with a Kirschner wire to prevent rotation. In these situations one screw is often used together with a Kirschner wire to prevent rotation.

88
Screws –Screws should never be used alone for diaphyseal fractures, since weight bearing will cause loosening and collapse of the fracture site.

89
Screws –Screws are used together with plates for diaphyseal fractures and all comminuted fractures of long bones, including fractures into joints.

90
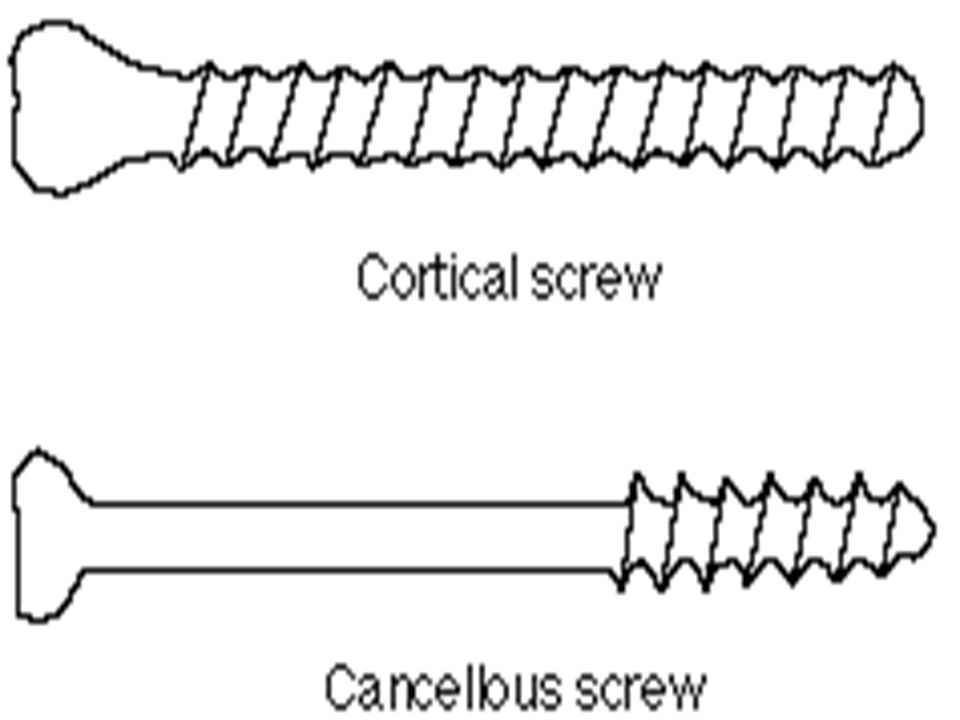
Screws Two basic types of screws Two basic types of screws –Fully threaded cortical screw –The partially threaded cancellous screw

92
Screws A cortical screw is a fully threaded screw A cortical screw is a fully threaded screw produces interfragmentary compression by means of a large gliding hole in the ciscortex (near cortex) and a smaller threaded hole in the transcortex (far cortex). produces interfragmentary compression by means of a large gliding hole in the ciscortex (near cortex) and a smaller threaded hole in the transcortex (far cortex).
 and a smaller threaded hole in the transcortex (far cortex)..")
93
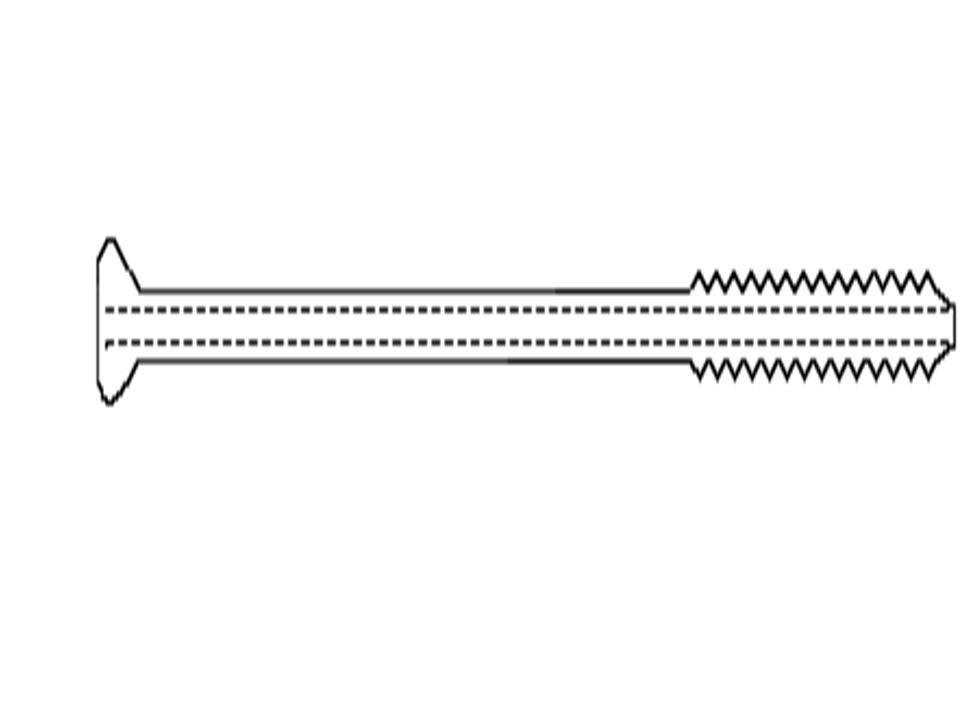
Screws A cancellous screw is a partially threaded screw A cancellous screw is a partially threaded screw exerts its interfragmentary compression by having all its threads on one side of the fracture plane exerts its interfragmentary compression by having all its threads on one side of the fracture plane

96
Lag Screw Effect

97
In addition to securing plates to bone, screws are used to provide static interfragmentary compression by means of the lag screw principle.

98
Lag Screw Effect To function as a lag screw the screw head engages the first (near) cortex and the threads engage bone only on the opposite side of the fracture line in the second cortex.
 cortex and the threads engage bone only on the opposite side of the fracture line in the second cortex.")
99
Lag Screw Effect As the screw is tightened the threads engage the bone on the far cortex and compress the fracture line.

100
External Fixation

101
First Aid To prevent complications To prevent complications –Splinting the affected limb –Safe transportation –Sedation to relieve anxiety

102
First Aid –Assessment of the general status of the animal –Radiograph the affected part

103
Principles of Management Reduction Reduction Realignment Realignment Immobilization Immobilization Physical therapy Physical therapy

104
Principles of Management Reduction: is the process of apposing the fracture fragments It is usually described as anatomic reduction anatomic reduction near anatomic reduction near anatomic reduction or non-anatomic reduction or non-anatomic reduction

105
Principles of Management Reduction should be undertaken as soon as the patient's condition permits Reduction should be undertaken as soon as the patient's condition permits Delay typically results in a more difficult and then traumatic reduction process Delay typically results in a more difficult and then traumatic reduction process

107
Principles of Management Alignment refers to the relative orientation or position of the fragments, or more specifically, deal with the joints above and below the fracture. refers to the relative orientation or position of the fragments, or more specifically, deal with the joints above and below the fracture.

108
Principles of Management Anatomic alignment is always strived Anatomic alignment is always strived for that it has a large bearing on function following healing for that it has a large bearing on function following healing

109
Principles of Management Alignment can be anatomic without anatomic reduction Alignment can be anatomic without anatomic reduction however, anatomic reduction will always achieve anatomic alignment. however, anatomic reduction will always achieve anatomic alignment.

110
Principles of Management Fixation is the mechanism by which the fracture fragments are stabilized until sufficient healing occurs.

111
Principles of Management The combination of the fixation device and the fracture segments is called an osteosynthesis. The combination of the fixation device and the fracture segments is called an osteosynthesis.

112
Principles of Management In general, the fixation should allow near normal function during the healing process. In general, the fixation should allow near normal function during the healing process.

113
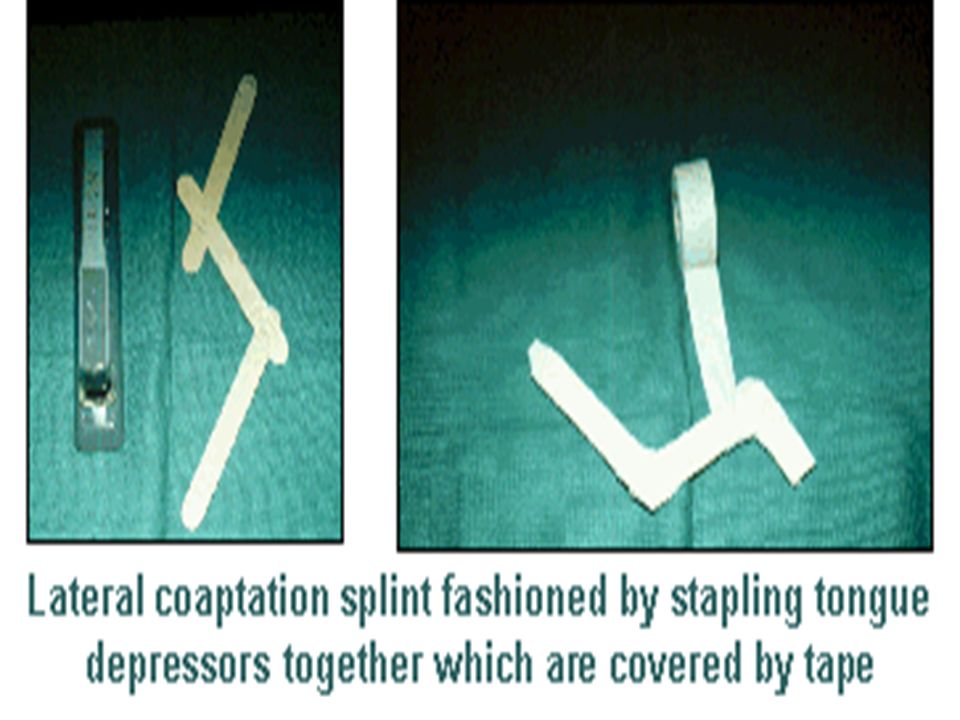
External Coaptation

114
Proper coaptation device for fractures in the darkly shaded area should extend the length of the lightly shaded area

115
External Coaptation Advantages of coaptation Applied immediately following closed reduction Applied immediately following closed reduction Additional trauma of surgery is avoided Additional trauma of surgery is avoided Fracture healing is not disrupted. Fracture healing is not disrupted.

116
External Coaptation Disadvantages of splints and casts Substantial amount of motion at the fracture site may persist Substantial amount of motion at the fracture site may persist Limit limb function Limit limb function

117
External Coaptation Require constant monitoring and/or changing Require constant monitoring and/or changing Fracture disease may occur Fracture disease may occur

118
External Coaptation Used for: Fractures distal to the elbow and stifle Fractures distal to the elbow and stifle Fractures that are relatively stable Fractures that are relatively stable Fractures that do not involve articular structures Fractures that do not involve articular structures Fractures in young animals Fractures in young animals

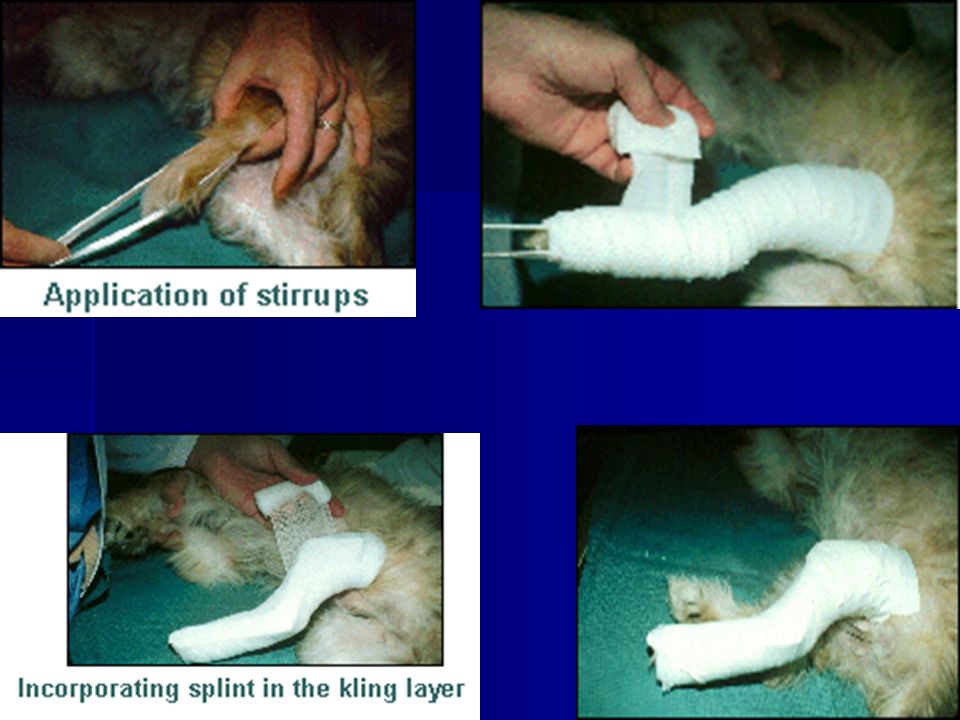
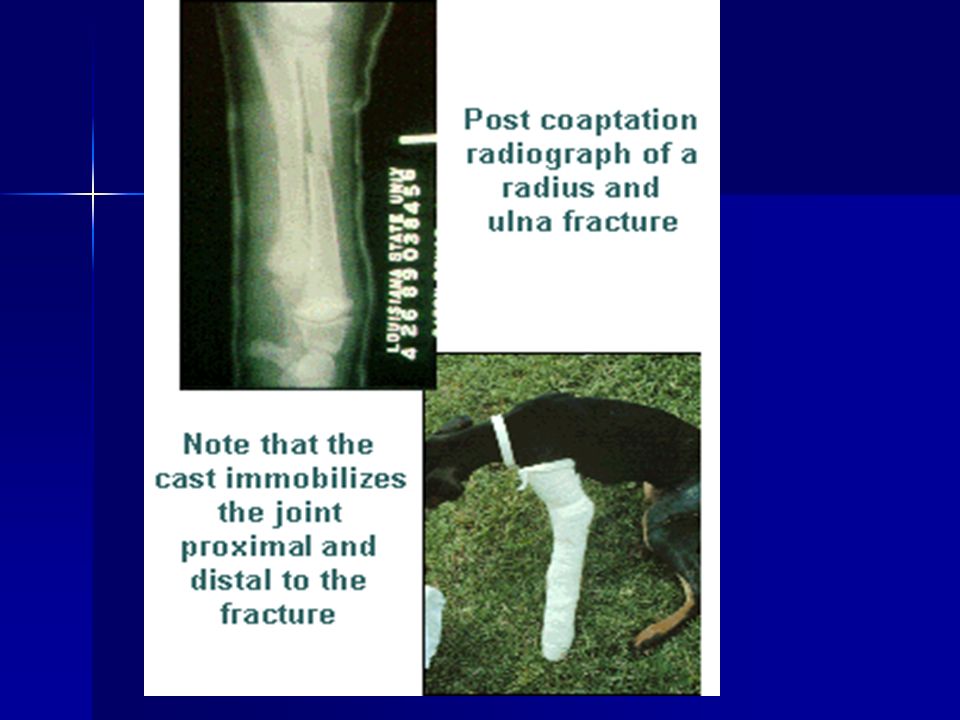
121
The cast should extend from the digits and extend above the joint proximal to the fracture. When applying casts which are molded to conform to the limb, it is protuberances that receive additional padding, rather than depressions.

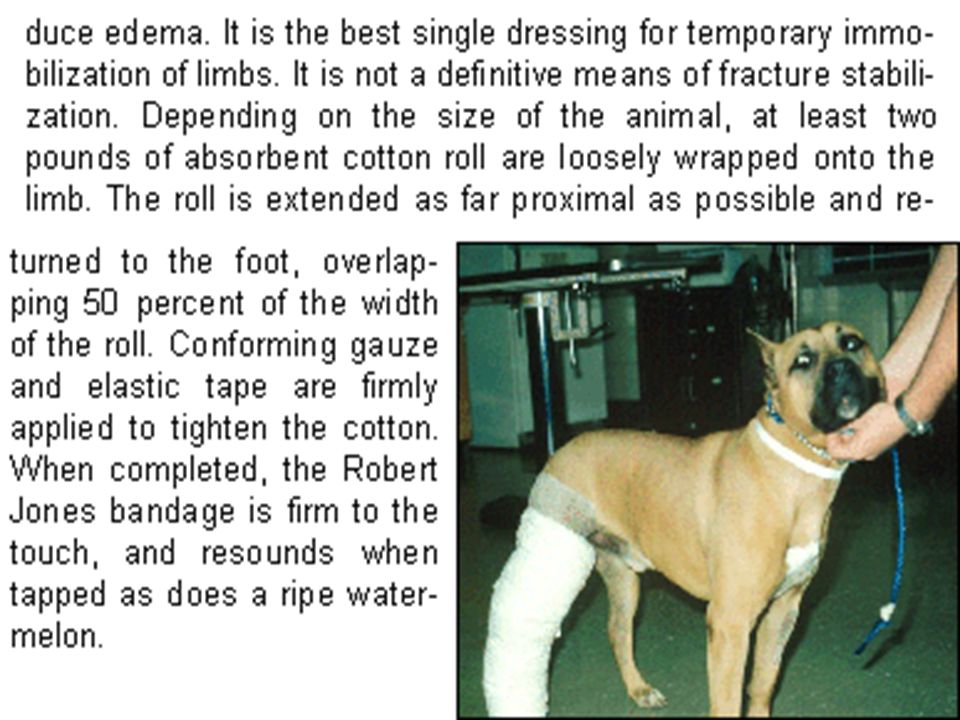
123
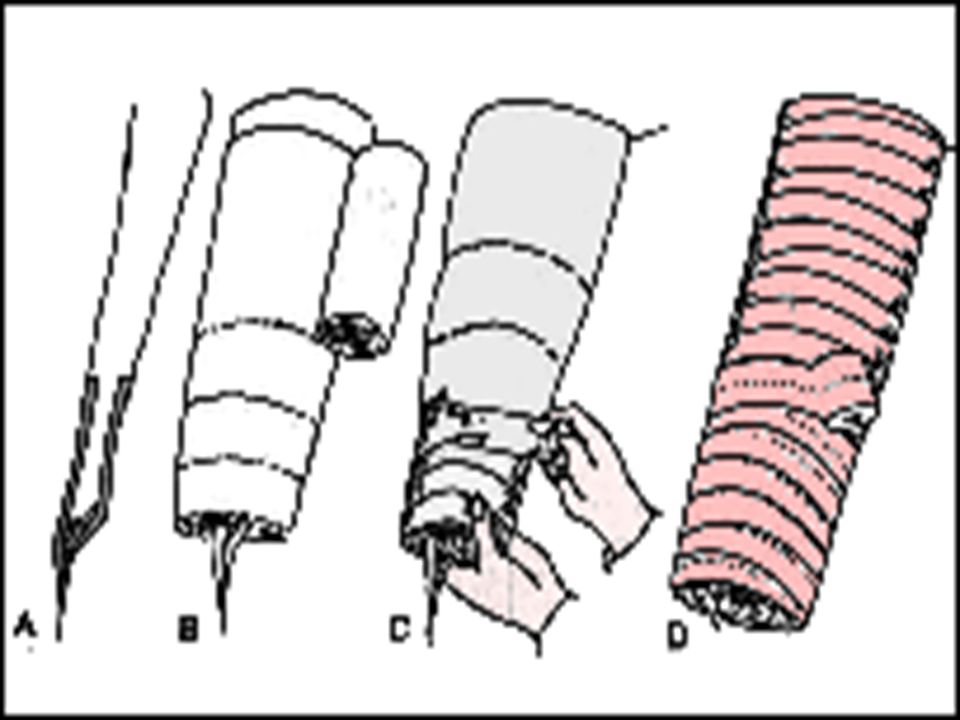
Robert Jones Bandage It immobilizes the limb and applies even pressure to prevent or reduce edema

124
Robert Jones Bandage Indications: 1. 1. Temporary bandage for the initial treatment of traumatized limbs 2. Initial postoperative treatment following internal fixation.

Similar presentations
















, F.R.C.S.(C )>")




![Thigh and knee. CLASSIFICATION FRACTURES OF THE FEMUR [1 ]Fracture of the neck of the femur, and [2]Fracture of the trochanteric region [3] Fracture of.](/14/4311083/big_thumb.jpg "Thigh and knee. CLASSIFICATION FRACTURES OF THE FEMUR [1 ]Fracture of the neck of the femur, and [2]Fracture of the trochanteric region [3] Fracture of.>")






>")
![Wrist and hand. CLASSIFICATION The injuries to be described may be classified by anatomical site as follows: Injuries of the carpus [1] Fracture of the.](/17/5380042/big_thumb.jpg "Wrist and hand. CLASSIFICATION The injuries to be described may be classified by anatomical site as follows: Injuries of the carpus [1] Fracture of the.>")
