Download presentation
Presentation is loading. Please wait.

1
Dr. Ibrahim Khasraw Lecturer in pediatrics School of Medicine University of Sulaimani

2
- Age of onset: 4-10y.,10% of all epilep. In children. - F.H. +ve in 13% of cases. - Attacks closely related to sleep, when the patient asleep or awake. - It is focal, involve the face, pharynx and possibly the arm. - - The patient is conscious but unable to speak and may drool saliva. - Excellent prognosis and resolves after puberty, may need no treatment. - E.E.G. during sleep show abnormal 1 or both prerolandic gyrus. - Rx. : carbamazapine or phenytoin.

4
- There are sensory and motor phenomena. - Consciousness impaired. - The motor manifestations are complex and semipurposful e.g.; picking at clothes or walking in a circle (Automatism). - There is postical state : a period of confusion or exhaustion after the attack. - E.E.G. Show temporal spikes or waves. - Rx. : carbamazapin, phenytoin ± tiagabine.
. - There is postical state : a period of confusion or exhaustion after the attack. - E.E.G. Show temporal spikes or waves. - Rx. : carbamazapin, phenytoin ± tiagabine..")
6
- Commonly starts between 4-6y of age. - Characterized by staring and loss of awareness of the environment. - Attacks are brief lasts <30 sec. and terminates abruptly without postictal state. - Hyperventilation for 3-4 min. will bring the attack. - E.E.G. : Typical spike and wave discharge 3/sec.. - Rx. : Ethosuximide or valproate are 1 st choice, clonazipam 2 nd line.

8
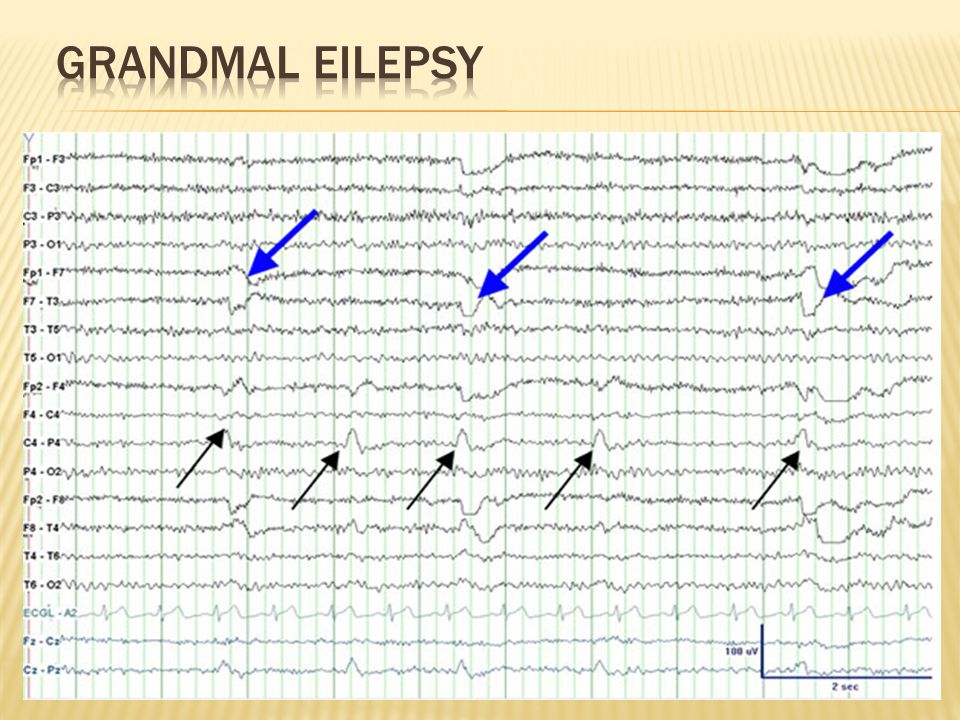
- It is generallized very common may follow partial S. or occur denovo. - Presence of aura always indicate a focal onset of S. - The patient suddenly loss consciousness, eye roll back and entire body muscles undergo tonic contractions, apnea and cyanosis.The clonic phase slows toward the end of the S. and the patient sigh as the S. stops abruptly. - Postictal children are initaially semicomatous and remain asleep for 30-120 min. Then the patient often get vomiting, severe frontal headache. - E.E.G. show generalized spikes and waves. - Rx. : valproate is the drug of choice, 2 nd carbamazopine and phenytoin.

10
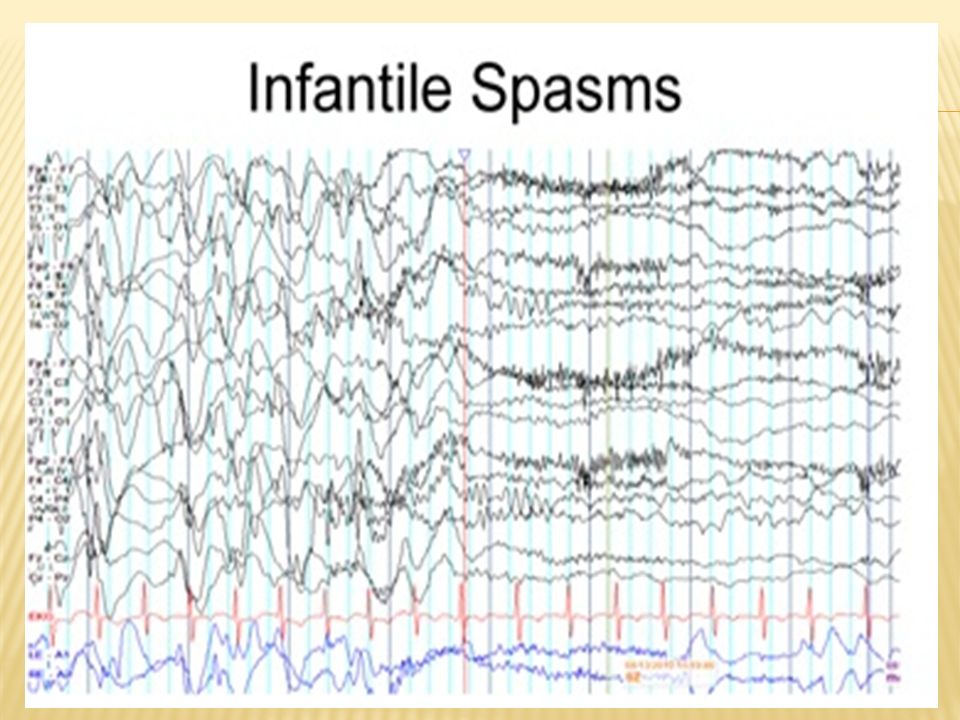
-Its called (west-syndrom) if associated with M.R - May be idiopathic or symptomatic e.g.: tuberosclerosis. - Onset usually at 4-8 m of age. - Characterized by brief symmetric contraction of the neck, tranck and extremities occuring in clusters of S. persisting for minutes with brief interval between each spasm. - - E.E.G shows chaotic pattern of high voltage bilaterally asynchronus, slow wave activity (hyps arrythmia). - Rx. : A.C.T.H., oral prednisolone. are drugs of choice or vigabatrin, clonazipam, valproate alternative. - Prognosis : poor in symptomatic better in idop.
. - Rx. : A.C.T.H., oral prednisolone. are drugs of choice or vigabatrin, clonazipam, valproate alternative. - Prognosis : poor in symptomatic better in idop..")
Similar presentations




 The only diagnostic test for absence seizures Ambulatory EEG monitoring over 24 hours may be useful to.>")









 are brief (lasting seconds) generalised epileptic seizures of abrupt onset.>")







