Download presentation
Presentation is loading. Please wait.

1
Type I DM in Pediatric Prepared by: Dr Moslah Jabari Pediatric Endocrinologist Assistant Professor in Pediatrics

2
Introduction Insulin regimen Insulin dose Diet Monitoring Hypoglycemia Management during infection Management during surgery Screening for chronic complication

3
DIAGNOSTIC CRITERIA FOR IMPAIRED GLUCOSE TOLERANCE AND DIABETES MELLITUS

4
Diagnostic Criteria of Impaired Glucose Tolerance and Diabetes Mellitus Table Symptoms include polyuria, polydipsia, and unexplained weight loss with glucosuria and ketonuria. A fasting glucose concentration of 99 mg/dL is the upper limit of “normal”.

5
Etiologic Classification of Diabetes Mellitus Table

6
Epidemiology: The incidence among school-age children is about 1.9/ 1,000 in USA with annual incidence about 14.9 new cases/ 100,000 children. Sex: M:F ratio is 1:1. Age at presentation: Peaks occur in 2 age groups. At 5-7 yr of age and puberty Seasonal variations: More frequent in the autumn and winter months.

7
Etiology : The Mechanisms that lead to failure of pancreatic ß-cell function increasingly point to an auto immune destruction of pancreatic islet ß cells in predisposed individuals.

8
Evidences supporting the auto immune basis of type 1 DM (T1DM) 1.Type 1 DM is commonly associated with auto immune diseases as celiac disease, Addison disease, and thyroiditis. 2. Auto antibodies as (GAD)and islet cell cytoplasm antibodies (ICA) and insulin auto antibodies (IAA) are detected in the sera of newly diagnosed patients.
and islet cell cytoplasm antibodies (ICA) and insulin auto antibodies (IAA) are detected in the sera of newly diagnosed patients..")
9
Evidences supporting the auto immune basis of type 1 DM (T1DM) 3. Genetic predisposition (the increased protection and susceptibility to T1DM) The Genetics of type 1 DM cannot be classified according to a specific model of inheritances. The most important genes are located within the MHC HLA class II region on chromosome 6p21, accounting for about 60% of genetic susceptibility for the disease.
 The Genetics of type 1 DM cannot be classified according to a specific model of inheritances. The most important genes are located within the MHC HLA class II region on chromosome 6p21, accounting for about 60% of genetic susceptibility for the disease..")
10
Evidences supporting the auto immune basis of type 1 DM (T1DM) a.The inheritance of HLA-DR3 or DR4 antigens (susceptibility haplotypes) increases the risk for developing type 1 DM two to 3 folds. The inheritance of both antigens increases the risk 7-10 fold. b.Role of HLA Class : Certain alleles of class II HLA genes appear to have the strongest associations with diabetes, the most significant association is with HLA-B39, which confers high risk for type 1A diabetes.

11
Evidences supporting the auto immune basis of type 1 DM (T1DM) c. The inheritance of certain genotype HLA-DRB1-0401 DQB1-302 DQA1-0301 confer high risk susceptibility. d. The inheritance of certain genotype provide significant protection as HLA-DRB1-0403 DQB1-0301 DQA1-0102

12
Evidences supporting the auto immune basis of type 1 DM (T1DM) The homozygous absence of aspartic acid at position 57 of the HLA-DQ ß-chain confers about 100 fold relative risk for the development of T1DM. e. Insulin gene locus: It is found to be associated with risk of T1DM and it is estimated that this locus accounts for about 10% of the familiar risk of T1DM.

13
Evidences supporting the auto immune basis of type 1 DM (T1DM) 4. Environment Factors such as viral infections, chemicals, seasonal factors, and dietary factors have been suspected of contributing to differences in the incidence and prevalence of type 1 DM in various ethnic populations.

14
Evidences supporting the auto immune basis of type 1 DM (T1DM) a. Viral Infections: A variety of viruses and mechanisms may contribute to the development of T1DM in genetically susceptible hosts. Enteroviral, congenital rubella, and mumps infection leads to the development of ß-cell auto immunity with high frequency and to T1DM in some cases. Congenital rubella infection is associated with diabetes (up to 40%).
..")
15
Evidences supporting the auto immune basis of type 1 DM (T1DM) b. Diet Breast-feeding May lower the risk of T1DM, either directly or by delaying exposure to cow’s milk protein.

16
Evidences supporting the auto immune basis of type 1 DM (T1DM) Early introduction of cow’s milk protein and early exposure to gluten in cereals have both been implicated in the development of auto immunity and it has been suggested that this is due to the “leakiness” of the immature gut to protein antigen s. Antigens that have been implicated include ß- lactoglobulin, which is homologous to the human protein glycodelin (PP14), a T-cell modulator. Other studies have focused on bovine serum abumin as the inciting antigen,.
, a T-cell modulator. Other studies have focused on bovine serum abumin as the inciting antigen,..")
17
Evidences supporting the auto immune basis of type 1 DM (T1DM) Other dietary factors that have been suggested at various times as playing a role in diabetes risk include Omega-3 fatty acids, Vitamin D, ascorbic acid, zinc, and Vitamin E Vitamin D has a role in immune regulation, decreased Vitamin D levels in pregnancy or early childhood may be associated with diabetes risk; but the evidence is not yet conclusive.
 Other dietary factors that have been suggested at various times as playing a role in diabetes risk include Omega-3 fatty acids, Vitamin D, ascorbic acid, zinc, and Vitamin E Vitamin D has a role in immune regulation, decreased Vitamin D levels in pregnancy or early childhood may be associated with diabetes risk; but the evidence is not yet conclusive.")
18
Evidences supporting the auto immune basis of type 1 DM (T1DM) c. Psychologic stress: Several studies show an increased prevalence of stressful psychologic situations among children who subsequently developed T1DM. Whether these stresses only aggravate pre-existing auto immunity or whether they can actually trigger auto immunity remains unknown.

19
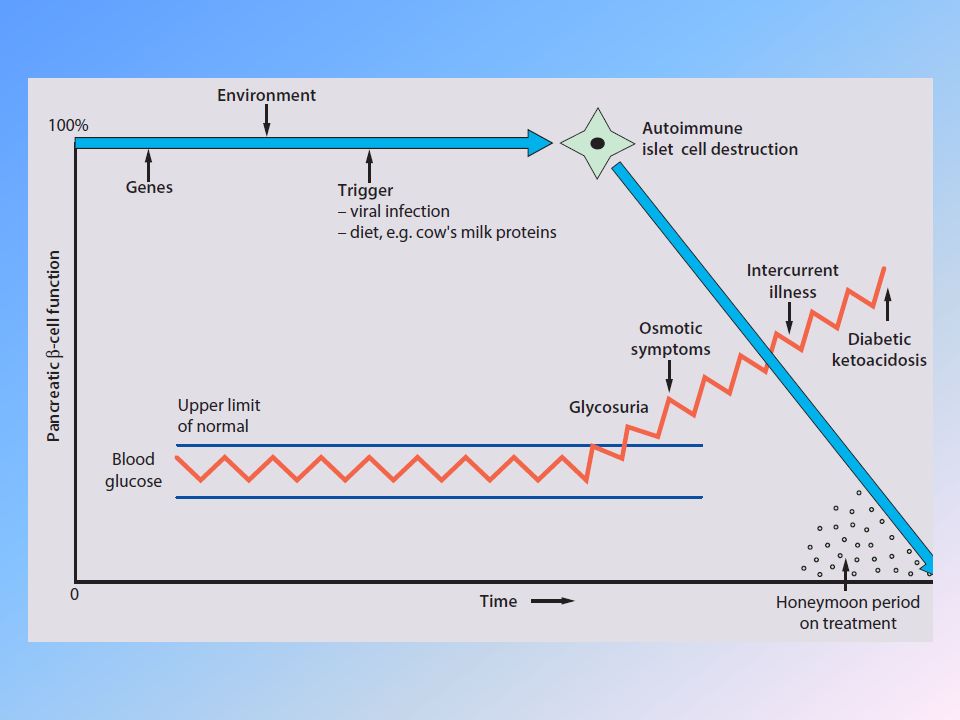
Pathogenesis and natural history of type 1 diabetes mellitus A genetically susceptible host develops auto immunity against his or her own ß cells. What triggers this auto immune response remains unclear at this time. In some ( But not all) patients, this auto immune process results in progressive destruction of ß cells until a critical mass of ß cells are destroyed and the patient becomes totally dependent on exogenous insulin for survival.
 patients, this auto immune process results in progressive destruction of ß cells until a critical mass of ß cells are destroyed and the patient becomes totally dependent on exogenous insulin for survival..")
20
Pathogenesis and natural history of type 1 diabetes mellitus 1.Initiation of auto immunity. 2. Preclinical auto immunity with progressive loss of ß-cell function. 3. Onset of clinical disease. 4. Transient remission (honeymoon period). 5. Established disease. 6. Development of complications.
. 5. Established disease. 6. Development of complications..")
22
Pathophysiology In normal individuals, there are normal swings between the postprandial, high-insulin anabolic state and fasted, low-insulin catabolic state that affect 3 major tissues: liver, muscle, and adipose tissue.

23
Influence of feeding (High Insulin) or of fasting (Low Insulin) on some Metabolic processes in liver, muscles and adipose tissue. Tissue Postprandial State (High Plasma Insulin) Fasted State (Low Plasma Insulin) Liver Glucose uptake, glycogen synthesis, absence of gluconeogenesis Lipogenesis Absence of ketogenesis Glucose production (glycogenolysis + gluconeogenesis) Absence of lipogenesis Ketogenesis Muscle Glucose uptake and oxidation, and glycogen synthesis Protein synthesis Absence of glucose uptake Glycogenolysis Proteolysis and amino acid release Adipose Tissue Glucose uptake Triglyceride uptake Lipid synthesis Absence of glucose uptake Absence of triglyceride uptake Lipolysis and fatty acids release
 Fasted State (Low Plasma Insulin) Liver Glucose uptake, glycogen synthesis, absence of gluconeogenesis Lipogenesis Absence of ketogenesis Glucose production (glycogenolysis + gluconeogenesis) Absence of lipogenesis Ketogenesis Muscle Glucose uptake and oxidation, and glycogen synthesis Protein synthesis Absence of glucose uptake Glycogenolysis Proteolysis and amino acid release Adipose Tissue Glucose uptake Triglyceride uptake Lipid synthesis Absence of glucose uptake Absence of triglyceride uptake Lipolysis and fatty acids release.")
24
1.Hyperglycemia- (fasting and increases after eating): due to glucose production (glycogenolysis and gluconeogenesis) and absence of glucose uptake by muscle and adipose tissues.
: due to glucose production (glycogenolysis and gluconeogenesis) and absence of glucose uptake by muscle and adipose tissues.")
25
2.Glucosuria - When blood glucose level exceeds the renal tubular maximum (Tm) of glucose (180 mg/dL). Calories are lost in urine a compensatory hyperphagia. If the Hyperphagia does not keep pace with the glucosuria, loss of body fat ensues with clinical weight loss.

26
I nfluence of feeding (High Insulin) or of fasting (Low Insulin) on some Metabolic processes in liver, muscles and adipose tissue. 3. Metabolic Acidosis- Insulinopenia, diminished energy production from glucose lipolysis. Peripheral utilization of fatty acids is incomplete and they are converted to ketone bodies in the liver. Accumulation of ketoacids (acetoacetic, ß-hydroxybutyric acids) will lead to metabolic acedosis. Ketoacidosis leads Kussmaul respiration (deep rapid breathing), fruity breath odor (acetone), diminished neurocognitive function, and possible coma.
 will lead to metabolic acedosis. Ketoacidosis leads Kussmaul respiration (deep rapid breathing), fruity breath odor (acetone), diminished neurocognitive function, and possible coma..")
27
4.Dehydration and loss of electrolytes Ketones in association with cations are excreted in urine- loss of fluid and electrolytes, also hyperglycemia will lead to osmotic diuresis.

28
5.Hyperosmolality - It is due to dehydration and hyperglycemia. Serum osmolality in mOsm/kg=2 (serum Na) glucose mg/ dL /18 + BUN mg/ dL /3.
 glucose mg/ dL /18 + BUN mg/ dL /3..")
29
6.Impaired level of consciousness- it is due to dehydration, hyperosmolality, metabolic acidosis, and diminished cerebral oxygen utilization.

30
Clinical Manifestations Different clinical presentations 1. The classic presentation of diabetes in children is a history of polyuria, polydipsia, hyperphagia, and loss of weight (loss of body fat). The duration of these symptoms is often less than 1 mo. Hyperphagia occurs as a compensatory mechanism when calories are lost in the urine (glucosuria).
. The duration of these symptoms is often less than 1 mo. Hyperphagia occurs as a compensatory mechanism when calories are lost in the urine (glucosuria)..")
31
Clinical Manifestations 2. Enuresis (due to polyuria) in a previously toilet-trained child. 3. Insidious onset with lethargy, weakness, and weight loss (in spite of an increased Apetite). 4. Pyogenic skin infections or monolial vaginitis ( in teenage girls due to chronic glucosuria).
. 4. Pyogenic skin infections or monolial vaginitis ( in teenage girls due to chronic glucosuria)..")
32
Clinical Manifestations 5. Diabetic ketoacido sis- it is the clinical presentation of 20%-40% of new-onset diabetic children and in children with known diabetes who omit insulin doses or who do not successfully manage the precipitating factors (trauma, infection, vomiting, and psychologic disturbances).
..")
33
Clinical Manifestations The early manifestations may be mild (nausea, vomiting, polyuria and dehydration). Kussmaul respiration (deep rapid respiration due to metabolic acidosis in an attempt to excrete excess CO2) with an odor of acetone on the breath (acetone is formed by non enzymatic conversion of acetoacetate).
 with an odor of acetone on the breath (acetone is formed by non enzymatic conversion of acetoacetate)..")
34
Clinical Manifestations Abdominal pain or rigidity (DD: appendicitis, pancreatitis), nausea, and emesis. Severe dehydration Cerebral obtundation and ultimately coma.

36
Diagnosis of T1DM 1.Hyperglycemia- Non fasting blood glucose value exceeding 200 mg/ dL with typical symptoms. 2. Glucosuria

37
DD The differential diagnosis of diabetes mellitus is not difficult, since this is virtually the only condition that gives rise to hyperglycemia, glucosuria and ketosis.. Renal glucosuria Isolated Congenital disorder. Renal tubular disorder (Fanconi syndrome, Renal disorders due to intoxication by heavy metals {lead} or outdated tetracycline or inborn errors of metabolism {cystinosis}).
..")
38
DD. Causes of metabolic acidosis Uremia, gastroenteritis with metabolic acidosis, hypoglycemia, lactic acidosis, salicylate intoxication, sepsis and encephalitis.. Physical stress Transient hyperglycemia with glucosuria, this is induced by counter regulatory hormones.

39
New-Onset Diabetes without Ketoacidosis Excellent diabetes control involves many goals to maintain a balance between tight glucose control and avoiding hypoglycemia to eliminate polyuria and nocturia, to prevent ketoacidosis permit normal growth and development with minimal effect on lifestyle. initiation and adjustment of insulin, extensive teaching of the child and caretakers reestablishment of the life routines.

40
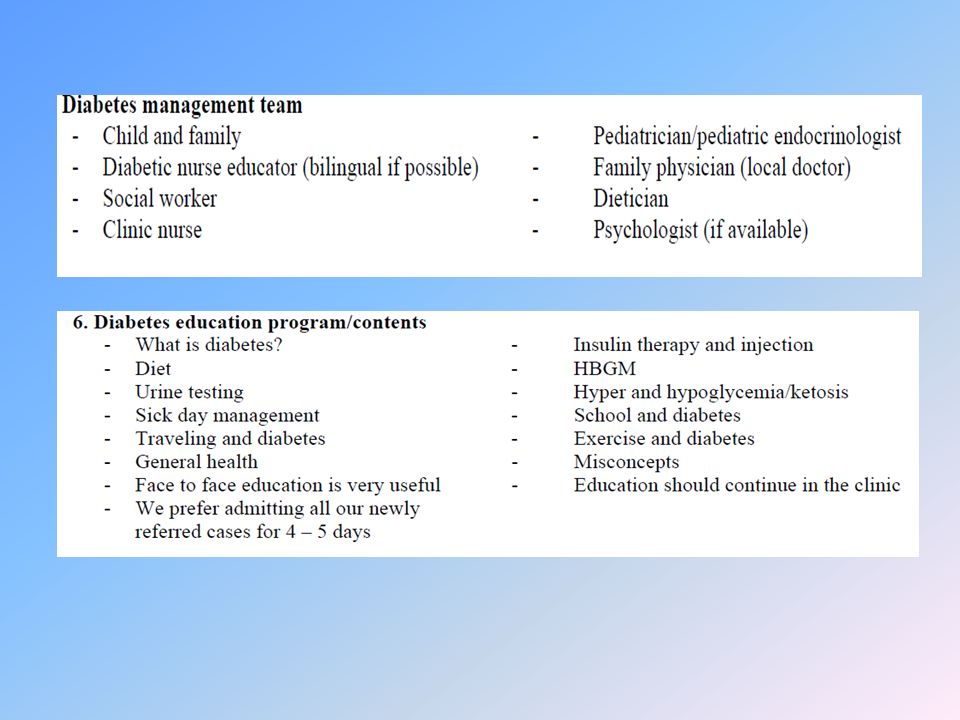
Each aspect should be addressed early in the overall care. therapy can begin in the outpatient setting, with complete team staffing by a pediatric endocrinologist, experienced nursing staff, dietitians with training as diabetes educators, and a social worker. Close contact between the diabetes team and family must be assured. Otherwise, initial therapy should be done in the hospital setting.

44
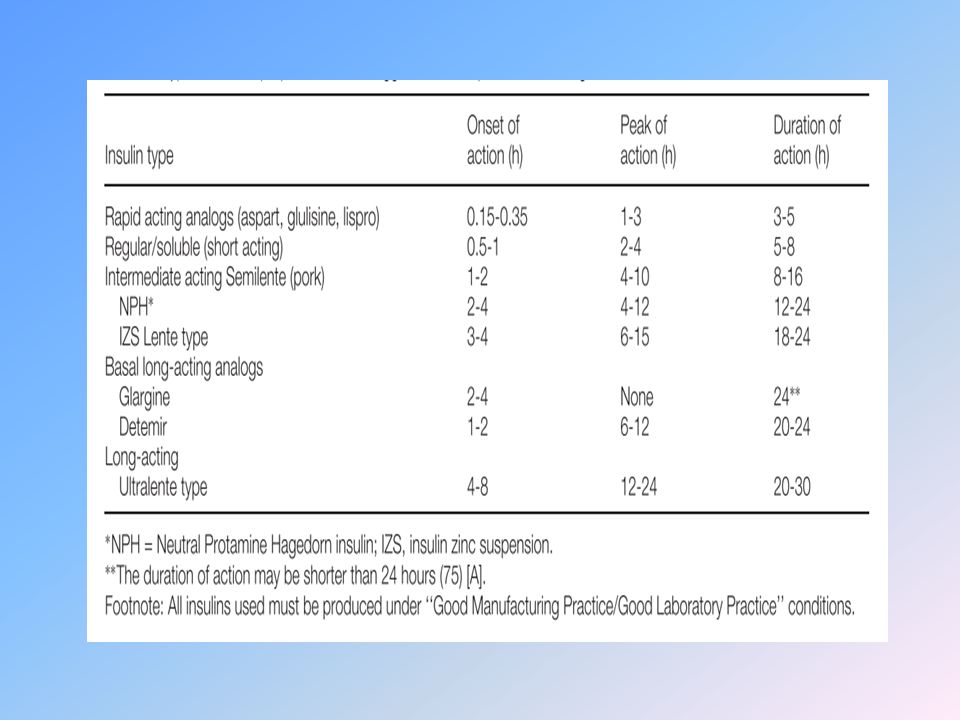
Types of Insulin Rapid Acting: – Insulin lispro (Humalog) ® – Insulin aspart (Novolog) ® – Insulin glulisine (Apidra) ® Short-acting: – Regular Intermediate-acting: – NPH Long-acting: – Insulin glargine (Lantus) ® – Insulin detemir (Levemir) ®
 ® – Insulin aspart (Novolog) ® – Insulin glulisine (Apidra) ® Short-acting: – Regular Intermediate-acting: – NPH Long-acting: – Insulin glargine (Lantus) ® – Insulin detemir (Levemir) ®")
45
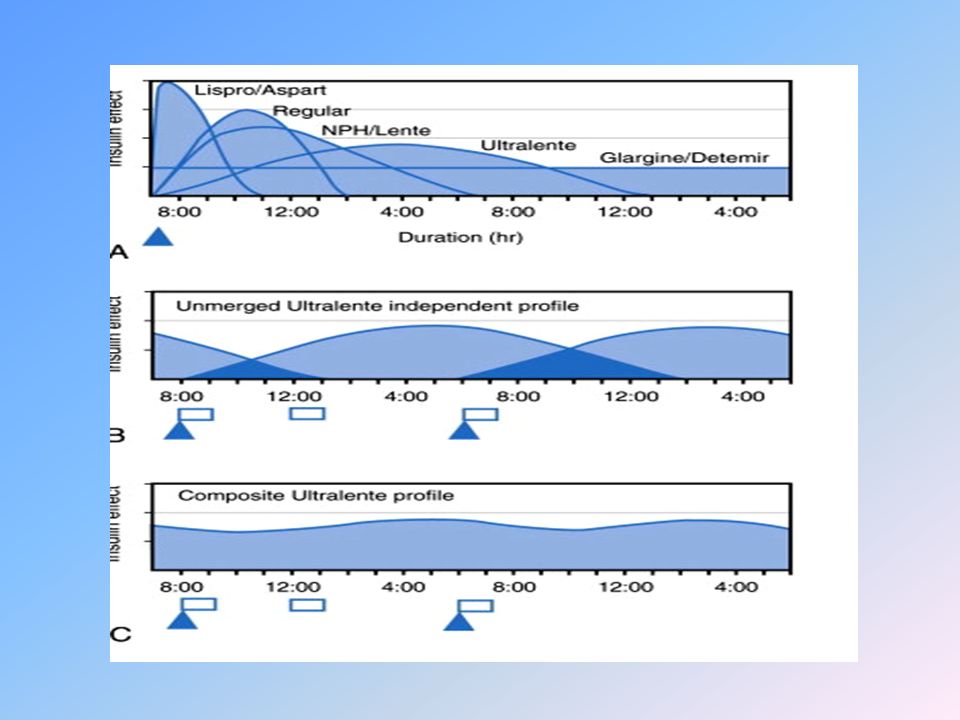
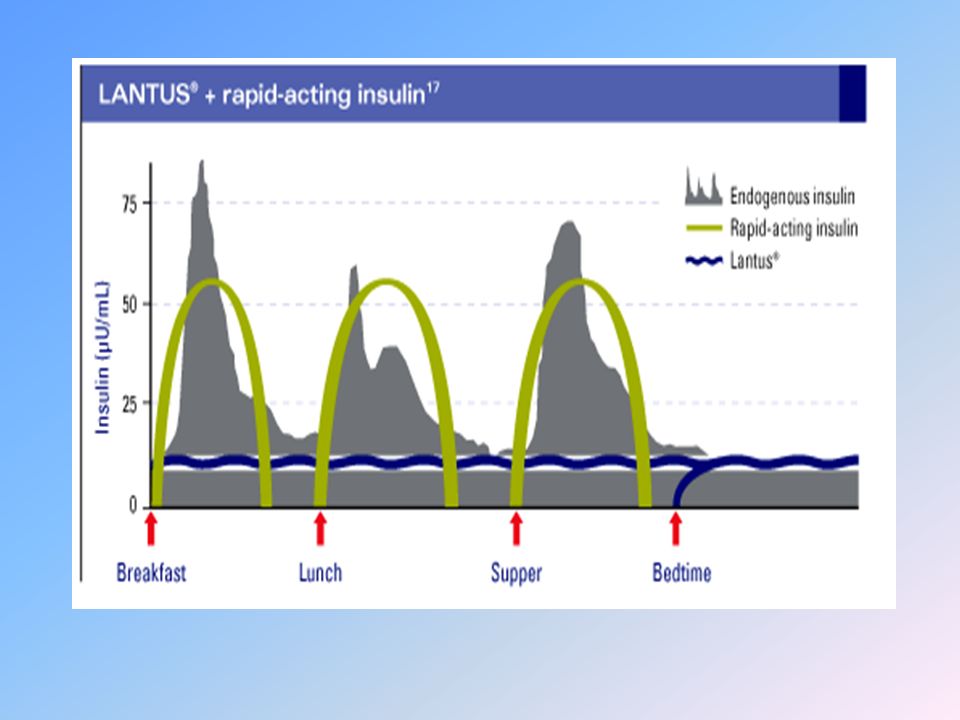
Rapid (lispro, aspart, glulisine) Hours Long (glargine) Short (regular) Intermediate (NPH) Long (detemir) Insulin Level 0 2 4 6 8 10 12 14 16 18 20 22 24 Pharmacokinetics of Insulin Products Adapted from Hirsch I. N Engl J Med. 2005;352:174-183.

47
Normal Insulin Secretion Basal (background) insulin needs 0 10 20 30 40 50 024681012141618202224 Serum insulin (µU/mL) Time Meal Bolus (meal) insulin needs 60
 insulin needs Serum insulin (µU/mL) Time Meal Bolus (meal) insulin needs 60")
48
Common Insulin Regimens The goal of treatment in type 1 DM is to provide insulin in as physiologic a manner as possible. Insulin replacement is accomplished by giving a basal insulin and a preprandial (premeal) insulin The basal insulin is either long-acting (glargine or detem The preprandial insulin is either rapid-acting (lispro, aspart, or glulisine) or short-acting (regular)
 insulin The basal insulin is either long-acting (glargine or detem The preprandial insulin is either rapid-acting (lispro, aspart, or glulisine) or short-acting (regular).")
49
For patients on intensive insulin regimens (multiple daily injections or insulin pumps), the preprandial dose is based on the carbohydrate content of the meal (the carbohydrate ratio) plus a correction dose if their blood glucose level is elevated This method allows patients more flexibility in caloric intake and activity, but it requires more blood glucose monitoring and closer attention to the control of their diabetes.blood glucose monitoring
, the preprandial dose is based on the carbohydrate content of the meal (the carbohydrate ratio) plus a correction dose if their blood glucose level is elevated This method allows patients more flexibility in caloric intake and activity, but it requires more blood glucose monitoring and closer attention to the control of their diabetes.blood glucose monitoring")
50
4:0016:0020:0024:004:00 BreakfastLunchDinner 8:00 12:008:00 Glargine or detemir Plasma insulin Basal/Bolus Treatment Program With Rapid- Acting and Long-Acting Analogs Bed Rapid (lispro, aspart, glulisine)
")
51
Subcutaneous Insulin Dosing Age (years) 0-5 5-12 12-18 Target Glucose (mg/dL) 100-200 80-150 80-130 Target Daily Insulin (units/kg/d) 0.6-0.7 0.7-1.0 1.0-1.2 Basal Insulin (% of total daily dose) 25-30 40-50 Bolus Units added per 100 mg/dL above target Insulin Units Added per 15 g at Meal 0.5 0.75 1.0-2.0
 Target Glucose (mg/dL) Target Daily Insulin (units/kg/d) Basal Insulin (% of total daily dose) Bolus Units added per 100 mg/dL above target Insulin Units Added per 15 g at Meal")
52
A four-step dosing schedule The basal insuline glargine should be 25-30% of the total dose in toddlers and 40-50% in older children. The remaining portion of the total daily dose is divided evenly as bolus injections for the three meals.

53
Newly diagnosed children in the “honeymoon” may only need 60-70% of a full replacement dose. Total daily dose per kg increases with puberty. Newly diagnosed children who do not use carbohydrate dosing should divide the nonbasal portion of the daily insulin dose into equal doses for each meal

54
For example: a 6 yr old child who weighs 20 kg needs about (0.7 U/kg/24 hr ? 20 kg) = 14 U/24 hr with 7 U (50%) as basal and 7 U as total daily bolus. Give basal as glargine at bedtime. Give 2 U lispro or aspart before each meal if the blood glucose is within target subtract 1 U if below target; add 0.75 U for each 100 mg/dL above target (round the dose to the nearest 0.5 U). For finer control, extra insulin may be added in 50-mg/dL increments.
 = 14 U/24 hr with 7 U (50%) as basal and 7 U as total daily bolus. Give basal as glargine at bedtime. Give 2 U lispro or aspart before each meal if the blood glucose is within target subtract 1 U if below target; add 0.75 U for each 100 mg/dL above target (round the dose to the nearest 0.5 U). For finer control, extra insulin may be added in 50-mg/dL increments..")
55
Indeed, bolus-basal treatment with multiple injections is better adapted to the physiologic profiles of insulin and glucose and can therefore provide better glycemic control than the conventional two-to-three dose regimen. This approach allows insulin doses to be changed as needed to correct hyperglycemia, supplement for additional anticipated carbohydrate intake, or subtract for exercise.

56
Some families may be unable to administer four daily injections. In these cases, a compromise may be needed: A three-injection regimen: Combining NPH with a rapid analog bolus at breakfast, a rapid acting analog bolus at supper, and NPH at bed time. This regimen may provide fair glucose control. A two-injection regimen: This would require NPH combined with a rapid analog bolus at breakfast and supper. However, such a schedule would provide poor coverage for lunch and early morning, and would increase the risk of hypo glycemia at midmorning and early night.

58
a. The total daily insulin requirement is calculated. b. 2/3 of the daily dose is given before breakfast and 1/3 before supper (if the total dose is 30 U, 20 U will be given before breakfast and 10 U before supper). c. Each injection consists of intermediate and regular insulins in proportions of 2: 1 or 3:1 (20 U before breakfast =14U of NPH + 6 U of regular insulin, and 10 U before supper= 6 U of NPH + 4 U of regular insulin).
. c. Each injection consists of intermediate and regular insulins in proportions of 2: 1 or 3:1 (20 U before breakfast =14U of NPH + 6 U of regular insulin, and 10 U before supper= 6 U of NPH + 4 U of regular insulin)..")
59
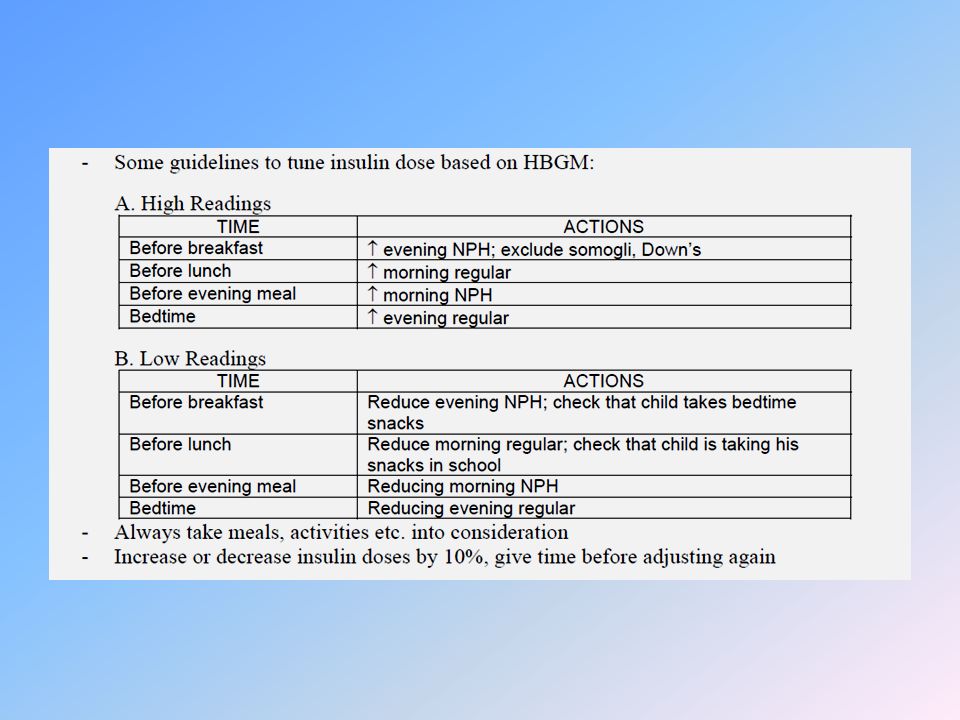
Fine adjustment of insulin dose NPH in the morning dose has primary influence on before supper blood glucose (after about 12 hr). Morning regular insulin has primary influence on before lunch blood glucose (after about 6 hr). NPH in the evening dose has primary influence on breakfast blood glucose (after about 12 hr). Evening regular insulin has primary influence on before bed blood glucose (after about 6 hr).
. NPH in the evening dose has primary influence on breakfast blood glucose (after about 12 hr). Evening regular insulin has primary influence on before bed blood glucose (after about 6 hr)..")
60
Fine Adjustment of the Two Injection Regimen

61
Examples Before lunch blood glucose level If the level is less than 80 mg/dL, decrease the dose of A.M regular insulin by 1-2 units. If the level is more than 150 mg/dL, increase the dose of A.M regular insulin by 1-2 units. Before supper blood glucose level If the level is less than 80 mg/dL, decrease the dose of A.M- NPH by 1-3 units. If the level is more than 150 mg/dl, increase the dose of A.M- NPH by 1-3 units and so on.

62
Common insulin regimens include thefollowing Split or mixed – NPH with rapid-acting (eg, lispro, aspart, or glulisine) or regular insulin before breakfast and supper Split or mixed variant – NPH with rapid-acting or regular insulin before breakfast, rapid-acting or regular insulin before supper, and NPH before bedtime (the idea is to reduce fasting hypoglycemia by giving the NPH later in the evening) Continuous subcutaneous insulin infusion (CSII) – Rapid-acting insulin infused continuously 24 hours a day through an insulin pump at 1 or more basal rates, with additional boluses given before each meal and correction doses administered if blood glucose levels exceed target levels
 or regular insulin before breakfast and supper Split or mixed variant – NPH with rapid-acting or regular insulin before breakfast, rapid-acting or regular insulin before supper, and NPH before bedtime (the idea is to reduce fasting hypoglycemia by giving the NPH later in the evening) Continuous subcutaneous insulin infusion (CSII) – Rapid-acting insulin infused continuously 24 hours a day through an insulin pump at 1 or more basal rates, with additional boluses given before each meal and correction doses administered if blood glucose levels exceed target levels")
63
The initial insulin schedule should be directed toward the optimal degree of glucose control in an attempt to duplicate the activity of the β cell. There are inherent limits to our ability to mimic the β cell. Exogenous insulin does not have a 1st pass to the liver, whereas 50% of pancreatic portal insulin is taken up by the liver, a key organ for the disposal of glucose; absorption of an exogenous dose continues despite hypoglycemia, whereas endogenous insulin release ceases and serum levels quickly lower with a normally rapid clearance; and absorption rate from an injection varies by injection site and patient activity level, whereas endogenous insulin is secreted directly into the portal circulation

64
Despite these fundamental physiologic differences, acceptable glucose control can be obtained with new insulin analogs used in a basal-bolus regimen, that is, with slow-onset, long-duration background insulin for between-meal glucose control and rapid-onset insulin at each meal. All preanalog insulins form hexamers, which must dissociate into monomers subcutaneously before being absorbed into the circulation. Thus, a detectable effect for regular (R) insulin is delayed by 30-60 min after injection. This, in turn, requires delaying the meal 30-60 min after the injection for optimal effect—a delay rarely attained in a busy child's life
 insulin is delayed by min after injection. This, in turn, requires delaying the meal min after the injection for optimal effect—a delay rarely attained in a busy child s life.")
65
R has a wide peak and a long tail for bolus insulin (Figs. 583-6 and 583-7). This profile limits postprandial glucose control, produces prolonged peaks with excessive hypoglycemic effects between meals, and increases the risk of nighttime hypoglycemia. These unwanted between-meal effects often necessitate “feeding the insulin” with snacks and limiting the overall degree of blood glucose control.
. This profile limits postprandial glucose control, produces prolonged peaks with excessive hypoglycemic effects between meals, and increases the risk of nighttime hypoglycemia. These unwanted between-meal effects often necessitate feeding the insulin with snacks and limiting the overall degree of blood glucose control..")
66
NPH and Lente insulins also have inherent limits because they do not create a peakless background insulin level (see Fig. 583-7C-E). This produces significant hypoglycemic effect during the midrange of their duration. Thus, it is often difficult to predict their interaction with fast-acting insulins. When R is combined with NPH or Lente (see Fig. 583-7E), the composite insulin profile poorly mimics normal endogenous insulin secretion. There are broad areas of excessive insulin effect alternating with insufficient effect throughout the day and night. Lente and Ultralente insulins have been discontinued and are no longer available.
. This produces significant hypoglycemic effect during the midrange of their duration. Thus, it is often difficult to predict their interaction with fast-acting insulins. When R is combined with NPH or Lente (see Fig E), the composite insulin profile poorly mimics normal endogenous insulin secretion. There are broad areas of excessive insulin effect alternating with insufficient effect throughout the day and night. Lente and Ultralente insulins have been discontinued and are no longer available..")
68
Frequent blood glucose monitoring and insulin adjustment are necessary in the 1st weeks as the child returns to routine activities and adapts to a new nutritional schedule, and as the total daily insulin requirements are determined. The major physiologic limit to tight control is hypoglycemia. Intensive control dramatically reduces the risk of long-term vascular complications; it is associated with a 3-fold increase in severe hypoglycemia. Use of insulin analogs moderates but does not eliminate this problem. Some families may be unable to administer 4 daily injections. In these cases, a compromise may be needed. A 3-injection regimen combining NPH with a rapid analog bolus at breakfast, a rapid-acting analog bolus at supper, and NPH at bedtime may provide fair glucose control

69
Further compromise to a 2-injection regimen (NPH and rapid analog at breakfast and supper) may occasionally be needed. However, such a schedule would provide poor coverage for lunch and early morning, and would increase the risk of hypoglycemia at midmorning and early night.

70
Insulin Therapy Several factors influence the initial daily insulin dose per kilogram of body weight. The dose is usually higher in pubertal children. most children with new-onset diabetes have some residual β-cell function (the honeymoon period), which reduces exogenous insulin needs Children with long-standing diabetes and no insulin reserve require about 0.7 U/kg/day if prepubertal 1.0 U/kg/day at midpuberty, 1.2 U/kg/day by the end of puberty. The optimal insulin dose can only be determined empirically, with frequent self- monitored blood glucose levels and insulin adjustment by the diabetes team Residual β-cell function usually fades within a few months and is reflected as a steady increase in insulin requirements and wider glucose excursions.
, which reduces exogenous insulin needs Children with long-standing diabetes and no insulin reserve require about 0.7 U/kg/day if prepubertal 1.0 U/kg/day at midpuberty, 1.2 U/kg/day by the end of puberty. The optimal insulin dose can only be determined empirically, with frequent self- monitored blood glucose levels and insulin adjustment by the diabetes team Residual β-cell function usually fades within a few months and is reflected as a steady increase in insulin requirements and wider glucose excursions..")
71
INSULIN DOSAGE Insulin requirement is based upon the body weight, age, and pubertal stage of the child In general, the newly diagnosed child requires an initial total daily insulin dose of 0.5 to 1.0 units/kg. Prepubertal children usually require lower doses, and the dose requirement may be as low as 0.25 units/kg for a variable period following diagnosis. Higher doses are needed in pubertal children, patients in ketoacidosis, or in patients receiving glucocorticoid therapy.

72
INSULIN DOSAGE In infants and toddlers who receive their insulin by syringe, the insulin dose may be so small that dilution is required to allow for easier and more precise administration. The smallest dose of insulin that can be accurately administered without dilution using a syringe is 0.5 units. Many insulins can be diluted either at a specialized pharmacy or at home with proper training. Specific diluent for many insulin preparations is available from the insulin manufacturer. Some insulin pumps can deliver much smaller doses of insulin, of the order of 0.025 units at a time, often obviating this problem.

73
INSULIN DOSAGE On average, 1 unit of insulin is required to cover: 20 grams of carbohydrates in most young children (1 to 6 years of age) 10 to 12 grams of carbohydrates in older prepubertal children 8 to 10 grams in pubertal adolescents
 10 to 12 grams of carbohydrates in older prepubertal children 8 to 10 grams in pubertal adolescents")
74
INSULIN DOSAGE When converting a patient from MDI or conventional therapy to insulin pump, the initial dose is dependent on diabetes control and total daily insulin dose. If control has been excellent, the initial daily insulin pump dose is 10 to 20 percent less than the previous dose. If control has been poor, the same total previous daily dose should be used. One study suggests patients using detemir insulin may require greater dose reductions (26 to 33 percent) when switching from MDI to the insulin pump.
 when switching from MDI to the insulin pump..")
75
Glycemic Targets Glucose values are plasma (mg/mL Glycemic Targets Glucose values are plasma (mg/mL) Age Pre-Meal BG HS/Night BG HbA1c Toddler (0-5 yrs) 100-180110-200 ≥7.5 & ≤8.5% School-age (6-11 yrs) 90-180100-180<8% Adolescent (12-19 yrs) 90-13090-150<7.5% Adults <7%
 Age Pre-Meal BG HS/Night BG HbA1c Toddler (0-5 yrs) ≥7.5 & ≤8.5% School-age (6-11 yrs) <8% Adolescent (12-19 yrs) <7.5% Adults <7%")
86
Insulin is sensitive to heat and exposure to oxygen. Once a bottle of insulin is open, it should be used for no more than 28 days and then discarded; even if there is still some insulin in the bottle, it may have lost its clinical effectiveness. Insulin kept in a pump reservoir for longer than 3 days may lose its clinical effectiveness (though insulin aspart has now been approved for use for as long as 6 days in a pump). Sometimes, insulin distributed from the pharmacy has been exposed to heat or other environmental factors and therefore may be less active. If a patient is experiencing unexplained high blood sugar levels, new insulin vials should be opened and used.
. Sometimes, insulin distributed from the pharmacy has been exposed to heat or other environmental factors and therefore may be less active. If a patient is experiencing unexplained high blood sugar levels, new insulin vials should be opened and used..")
87
Insulin absorption ♦ Insulin activity profiles show substantial variability both day to day in the same individuals and between individuals, particularly children. ♦ The onset, peak effect and duration of action depend upon many factors which significantly affect the speed and consistency of absorption. ♦ Young people and care providers should know the factors which influence insulin absorption such as: Age (young children, less subcutaneous fat→faster absorption). Fat mass (large subcutaneous fat thickness, lipohypertrophy, also with rapid-acting analogs →slower absorption).
. Fat mass (large subcutaneous fat thickness, lipohypertrophy, also with rapid-acting analogs →slower absorption)..")
89
Regular insulin (short acting) Regular soluble insulin (usually identical to human insulin) is still used as an essential component of most daily replacement regimens in many parts of the world either combined with: ♦ Intermediate-acting insulin in twice daily regimen. ♦ As pre-meal bolus injections in basal-bolus regimens (given 20–30 min before meals) together with intermediate-acting insulin twice daily or a basal analog given once or twice daily.
 together with intermediate-acting insulin twice daily or a basal analog given once or twice daily..")
90
Intermediate acting insulins The action profiles of these insulinsmake them suitable for twice daily regimens and for pre-bed dosage in basal-bolus regimens Two principal preparations exist: ♦ Isophane NPH (neutral protamine Hagedorn) insulins. ♦ Crystalline zinc acetate insulin (insulin zinc suspensions, IZS or lente insulins). Isophane insulins are mostly used in children, mainly because of their suitability for mixing with regular insulin in the same syringe, vial or cartridge without interaction. Lente insulins are discontinued in many countries. NOTE: When regular insulin is mixed with lente preparations it reacts with excess zinc, blunting its short acting properties.
. Isophane insulins are mostly used in children, mainly because of their suitability for mixing with regular insulin in the same syringe, vial or cartridge without interaction. Lente insulins are discontinued in many countries. NOTE: When regular insulin is mixed with lente preparations it reacts with excess zinc, blunting its short acting properties..")
91
Regular Insulin are best suited for IV therapy and are used in the following crisis situations: Diabetic ketoacidosis. Control of diabetes during surgical procedures. Rapid-acting analog insulin can also be given IV. However, the effect is not superior to that of regular insulin and it is more expensive.

92
Insulin concentrations ♦ The most widely available insulin concentration is 100 IU/ml (U 100). ♦ Treatment with U 40 (40 IU/ml), U50 or other concentrations such as U500 is also acceptable, subject to availability and special needs. ♦ Care must be taken to ensure that the same concentration is supplied each time new supplies are received. ♦ Very young children occasionally require insulin diluted with diluent obtained from the manufacturer, but special care is needed in dilution and drawing up the insulin into the syringe. Rapid acting insulin can be diluted to U10 or U50 with sterile NPH diluent and stored for 1 month for use in pumps for infants or very young children.
, U50 or other concentrations such as U500 is also acceptable, subject to availability and special needs. ♦ Care must be taken to ensure that the same concentration is supplied each time new supplies are received. ♦ Very young children occasionally require insulin diluted with diluent obtained from the manufacturer, but special care is needed in dilution and drawing up the insulin into the syringe. Rapid acting insulin can be diluted to U10 or U50 with sterile NPH diluent and stored for 1 month for use in pumps for infants or very young children..")
93
Basal/Bolus Treatment Program With Rapid- Acting and Long-Acting Analogs 4:0016:0020:0024:004:00 BreakfastLunchDinner 8:00 12:008:00 Glargine or detemir Plasma insulin Bed Rapid (lispro, aspart, glulisine)
")
94
HbA1c Statistics for CHLA 2003 Type 1: Diabetes > 1 year, followed > 1 year Enrolled in Long-term study – total n 1800 nAverage ± SD All patients11818.2 ± 1.6 Males5798.2 ± 1.6 Females6028.2 ± 1.6 < 5517.8 ± 1.3 5-103557.9 ± 1.3 11-164898.4 ± 1.8 17-19 >20 157 127 8.3 ± 1.5 7.4 + 1.3

95
PenFill Cartridges or NovoLog (insulin aspart [rdna origin] inj) FlexPen Prefilled syringe. Keep at room temperature below 86°F (30°C) for up to 28 days. Do not store a PenFill cartridge or NovoLog (insulin aspart [rdna origin] inj) FlexPen Prefilled syringe that you are using in the refrigerator. Keep PenFill cartridges and NovoLog (insulin aspart [rdna origin] inj) FlexPen Prefilled syringe away from direct heat or light. Throw away a used PenFill cartridge or NovoLog (insulin aspart [rdna origin] inj) FlexPen Prefilled syringes after 28 days, even if there is insulin left in the cartridge or syringe.
![PenFill Cartridges or NovoLog (insulin aspart [rdna origin] inj) FlexPen Prefilled syringe.](http://images.slideplayer.com/27/8945241/slides/slide_95.jpg "Keep at room temperature below 86°F (30°C) for up to 28 days. Do not store a PenFill cartridge or NovoLog (insulin aspart [rdna origin] inj) FlexPen Prefilled syringe that you are using in the refrigerator. Keep PenFill cartridges and NovoLog (insulin aspart [rdna origin] inj) FlexPen Prefilled syringe away from direct heat or light. Throw away a used PenFill cartridge or NovoLog (insulin aspart [rdna origin] inj) FlexPen Prefilled syringes after 28 days, even if there is insulin left in the cartridge or syringe..")
99
Monitoring Success in the daily management of the diabetic child can be measured by the competence acquired by the family, and subsequently by the child, in assuming responsibility for daily “diabetic care.” Their initial and ongoing instruction in conjunction with their supervised experience can lead to a sense of confidence in making intermittent adjustments in insulin dosage for dietary deviations, for unusual physical activity and even for some minor intercurrent illnesses, as well as for otherwise unexplained repeated hypoglycemic reactions and excessive glycosuria. Such acceptance of responsibility should make them relatively independent of the physician for their ordinary care. The physician must maintain ongoing interested supervision and shared responsibility with the family and the child.

100
Self-monitoring of blood glucose (SMBG) is an essential component of managing diabetes. Monitoring often also needs to include insulin dose, unusual physical activity, dietary changes, hypoglycemia, intercurrent illness, and other items that may influence the blood glucose. These items may be valuable in interpreting the SMBG record, prescribing appropriate adjustments in insulin doses, and teaching the family. If there are discrepancies in the SMBG and other measures of glycemic control (such as the HbA 1c ), the clinician should attempt to clarify the situation in a manner that does not undermine their mutual confidence
, the clinician should attempt to clarify the situation in a manner that does not undermine their mutual confidence.")
101
Daily blood glucose monitoring has been markedly enhanced by the availability of strips impregnated with glucose oxidase that permit blood glucose measurement from a drop of blood. A portable calibrated reflectance meter can approximate the blood glucose concentration accurately. Many meters contain a memory “chip” enabling recall of each measurement, its average over a given interval, and the ability to display the pattern on a computer screen. Such information is a useful educational tool for verifying degree of control and modifying recommended regimens. A small, spring-loaded device that automates capillary bloodletting (lancing device) in a relatively painless fashion is commercially available.
 in a relatively painless fashion is commercially available..")
102
Parents and patients should be taught to use these devices and measure blood glucose at least 4 times daily—before breakfast, lunch, and supper and at bedtime. When insulin therapy is initiated and when adjustments are made that may affect the overnight glucose levels, SMBG should also be performed at 12 a.m. and 3 a.m. to detect nocturnal hypoglycemia. Ideally, the blood glucose concentration should range from approximately 80 mg/dL in the fasting state to 140 mg/dL after meals. In practice, however, a range of 60-220 mg/dL is acceptable based on age of the patient (Blood glucose measurements that are consistently at or outside these limits, in the absence of an identifiable cause such as exercise or dietary indiscretion, are an indication for a change in the insulin dose.

103
If the fasting blood glucose is high, the evening dose of long-acting insulin is increased by 10-15% and/or additional fast-acting insulin (lispro or aspart) coverage for bedtime snack may be considered. If the noon glucose level exceeds set limits, the morning fast-acting insulin (lispro or aspart) is increased by 10-15% If the pre-supper glucose is high, the noon dose of fast-acting insulin is increased by 10-15%. If the pre-bedtime glucose is high, the pre-supper dose of fast-acting insulin is increased by 10-15%. Similarly, reductions in the insulin type and dose should be made if the corresponding blood glucose measurements are consistently below desirable limits.
 is increased by 10-15% If the pre-supper glucose is high, the noon dose of fast-acting insulin is increased by 10-15%. If the pre-bedtime glucose is high, the pre-supper dose of fast-acting insulin is increased by 10-15%. Similarly, reductions in the insulin type and dose should be made if the corresponding blood glucose measurements are consistently below desirable limits..")
105
Hypoglycemic Reactions Hypoglycemia is the major limitation to tight control of glucose levels. Once injected, insulin absorption and action are independent of the glucose level, thus creating a unique risk of hypoglycemia from an unbalanced insulin effect. Insulin analogs may help reduce but cannot eliminate this risk. Most children with T1DM can expect mild hypoglycemia each week, moderate hypoglycemia a few times each year, and severe hypoglycemia every few years. These episodes are usually not predictable, although exercise, delayed meals or snacks, and wide swings in glucose levels increase the risk.

106
Infants and toddlers are at higher risk because they have more variable meals and activity levels, are unable to recognize early signs of hypoglycemia, and are limited in their ability to seek a source of oral glucose to reverse the hypoglycemia. The very young have an increased risk of permanently reduced cognitive function as a long-term sequela of severe hypoglycemia. For this reason, a more relaxed degree of glucose control is necessary until the child matures Hypoglycemia can occur at any time of day or night.

107
Early symptoms and signs (mild hypoglycemia) may occur with a sudden decrease in blood glucose to levels that do not meet standard criteria For hypoglycemia in nondiabetic children. The child may show pallor, sweating, apprehension or fussiness, hunger, tremor, and tachycardia, all due to the surge in catecholamines as the body attempts to counter the excessive insulin effect. Behavioral changes such as tearfulness, irritability, aggression, and naughtiness are more prevalent in children.

108
As glucose levels decline further, cerebral glucopenia occurs with drowsiness, personality changes, mental confusion, and impaired judgment (moderate hypoglycemia) progressing to inability to seek help and seizures or coma (severe hypoglycemia). Prolonged severe hypoglycemia can result in a depressed sensorium or Stroke like focal motor deficits that persist after the hypoglycemia has resolved. Although permanent sequelae are rare, severe hypoglycemia is frightening for the child and family and can result in significant reluctance to attempt even Moderate glycemic control afterward.

109
Important counter-regulatory hormones in children include growth hormone, cortisol, epinephrine, and glucagon. The latter 2 seem more critical in the older child. Many older patients with long-standing T1DM lose their ability to secrete glucagon in response to hypoglycemia. In the young adult, epinephrine deficiency may also develop as part of a general autonomic neuropathy. This substantially increases the risk of hypoglycemia because the early warning signals of a declining glucose level are due to catecholamine release.

110
Recurrent hypoglycemic episodes associated with tight metabolic control may aggravate partial counter-regulatory deficiencies, producing a syndrome of hypoglycemia unawareness and reduced ability to restore euglycemia (hypoglycemia-associated autonomic failure). Avoidance of hypoglycemia allows some recovery from this unawareness syndrome

113
The most important factors in the management of hypoglycemia are an understanding by the patient and family of the symptoms and signs of the reaction and an anticipation of known precipitating factors such as gym or sports activities. Tighter glucose control increases the risk. Families should be taught to look for typical hypoglycemic scenarios or patterns in the home blood glucose log, so that they may adjust the insulin dose and avert predictable episodes. A source of emergency glucose should be available at all times and places, including at school and during visits to friends. If possible, it is initially important to document the hypoglycemia before treating, because some symptoms may not always be due to hypoglycemia. Most families and children develop a good sense for true hypoglycemic episodes and can institute treatment before testing. Any child suspected of having a moderate to severe hypoglycemic episode should also be treated before testing.

114
It is important not to give too much glucose; 5-10 g should be given as juice or a sugar-containing carbonated beverage or candy, and the blood glucose checked 15-20 minutes later. Patients, parents, and teachers should also be instructed in the administration of glucagon when the child cannot take glucose orally. An injection kit should be kept at home and school. The intramuscular dose is 0.5 mg if the child weighs less than 20 kg and 1.0 mg if more than 20 kg. This produces a brief release of glucose from the liver. Glucagon often causes emesis, which precludes giving oral supplementation if the blood glucose declines after the glucagon effects have waned. Caretakers must then be prepared to take the child to the hospital for IV glucose administration,

115
Dawn Phenomenon There are several reasons that blood glucose levels increase in the early morning hours before breakfast. The most common is a simple decline in insulin levels and is seen in many children using NPH or Lente as the basal insulin at supper or bedtime. This usually results in routinely elevated morning glucose. The thought to be due mainly to overnight growth hormone secretion and increased insulin clearance. It is a normal physiologic process seen in most nondiabetic adolescents, who compensate with more insulin output. A child with T1DM cannot compensate and may actually have declining insulin levels if using evening NPH or Lente. The dawn phenomenon is usually recurrent and modestly elevates most morning glucose levels.

116
Somogyi phenomenon Rarely, high morning glucose is due to the Somogyi phenomenon, a theoretical rebound from late night or early morning hypoglycemia, thought to be due to an exaggerated counter-regulatory response. It is unlikely to be a common cause, in that most children remain hypoglycemic (do not rebound) once nighttime glucose levels decline. Continuous glucose monitoring systems may help clarify ambiguously elevated morning glucose levels.
 once nighttime glucose levels decline. Continuous glucose monitoring systems may help clarify ambiguously elevated morning glucose levels..")
117
Brittle Diabetes The term has been used to describe the child, usually an adolescent female, with unexplained wide fluctuations in blood glucose, often with recurrent DKA, who is taking large doses of insulin. An inherent physiologic abnormality is rarely present because these children usually show normal insulin responsiveness when in the hospital environment. Psychosocial or psychiatric problems, including eating disorders, and dysfunctional family dynamics are usually present, which preclude effective diabetes therapy. Hospitalization is usually needed to confirm the environmental effect, and aggressive psychosocial or psychiatric evaluation is essential. Therefore, clinicians should refrain from using “brittle diabetes” as a diagnostic term.

118
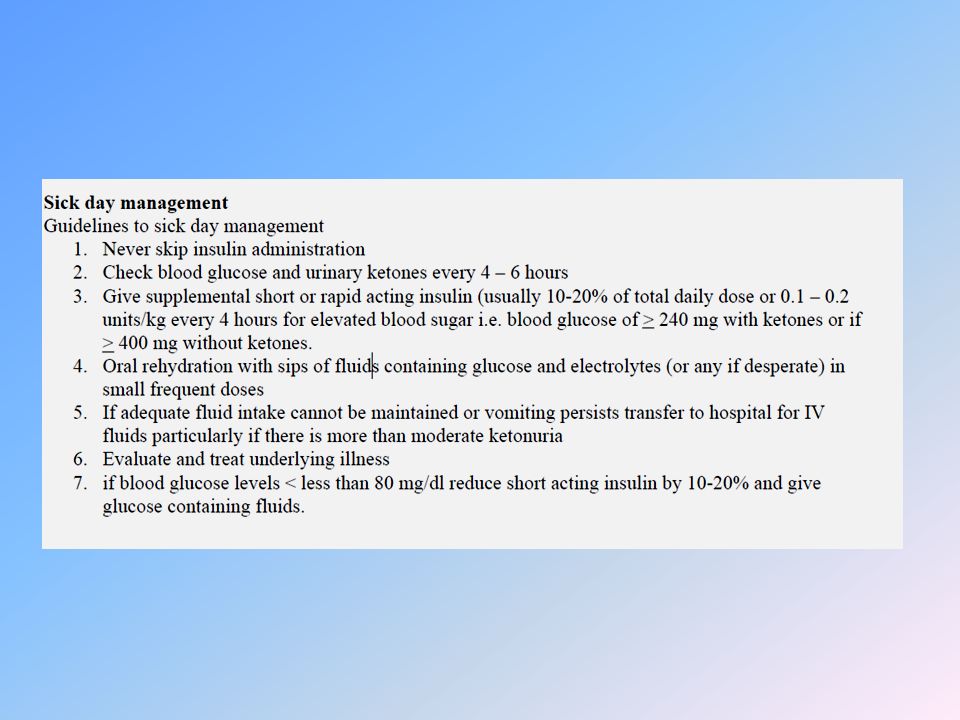
Management During Infections Although infections are no more common in diabetic children than in nondiabetic ones, they can often disrupt glucose control and may precipitate DKA. In addition, the diabetic child is at increased risk of dehydration if hyperglycemia causes an osmotic diuresis or if ketosis causes emesis. Counter-regulatory hormones associated with stress blunt insulin action and elevate glucose levels. If anorexia occurs, however, lack of caloric intake increases the risk of hypoglycemia. Although children younger than 3 yr tend to become hypoglycemic and older children tend toward hyperglycemia, the overall effect is unpredictable. Therefore, frequent blood glucose monitoring and adjustment of insulin doses are essential elements of sick day guidelines

120
The overall goals are to maintain hydration, control glucose levels, and avoid ketoacidosis. This can usually be done at home if proper sick day guidelines are followed and with telephone contact with health care providers. The family should seek advice if home treatment does not control ketonuria, hyperglycemia, or hypoglycemia, or if the child shows signs of dehydration. A child with large ketonuria and emesis should be seen in the emergency department for a general examination, to evaluate hydration, and to determine whether ketoacidosis is present by checking serum electrolytes, glucose, pH, and total CO 2. A child whose blood glucose declines to less than 50-60 mg/dL (2.8-3.3 mmol/L) and who cannot maintain oral intake may need IV glucose, especially if further insulin is needed to control ketonemia.
 and who cannot maintain oral intake may need IV glucose, especially if further insulin is needed to control ketonemia..")
123
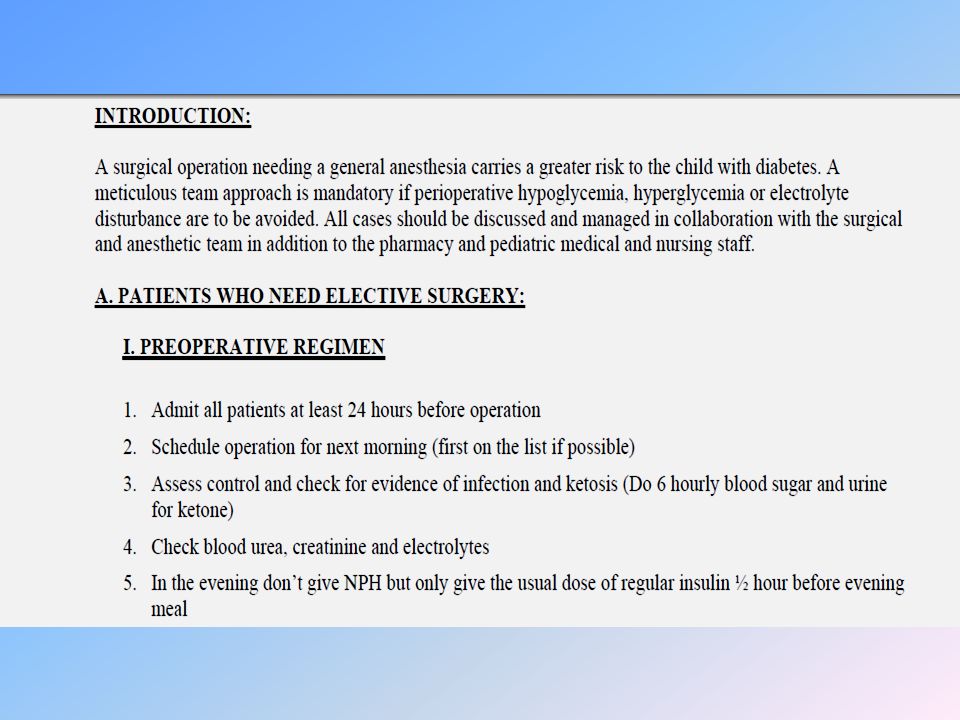
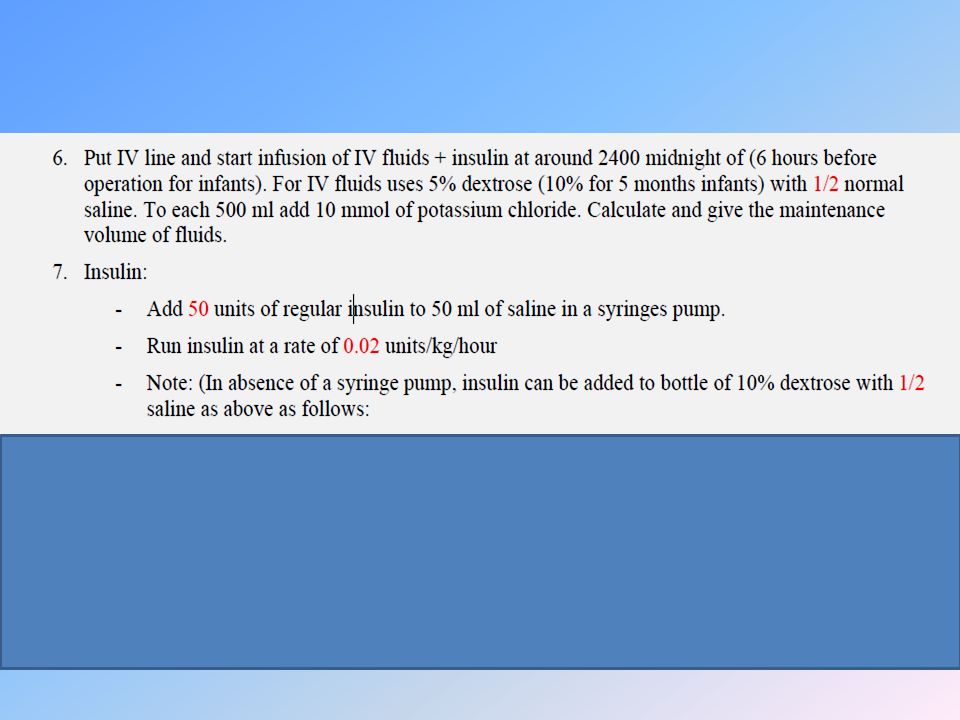
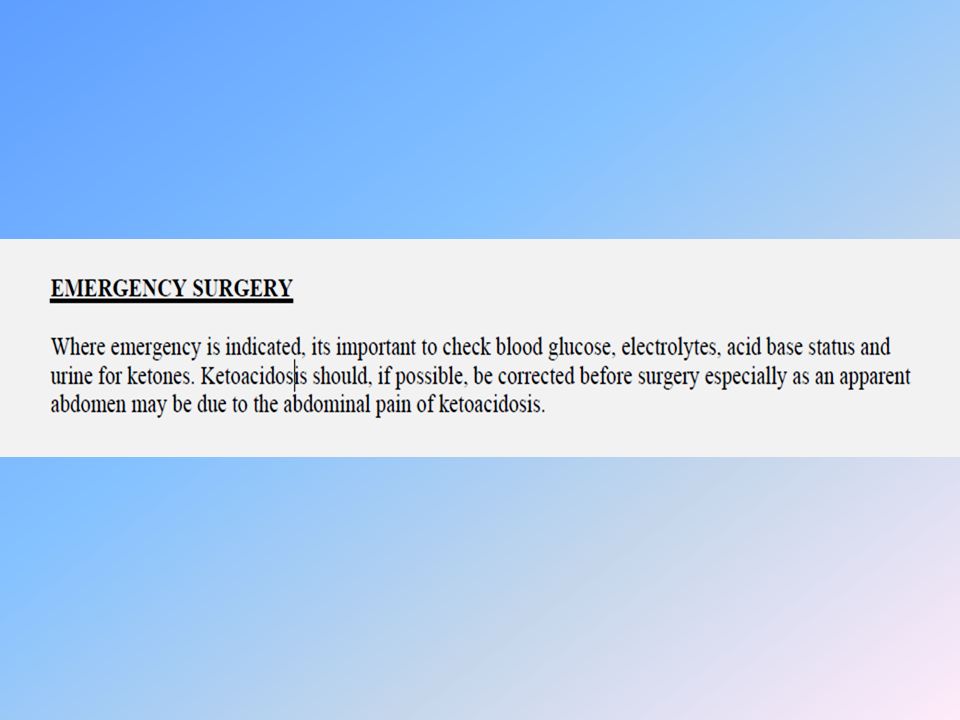
Management During Surgery Surgery can disrupt glucose control in the same way as can intercurrent infections. Stress hormones associated with the underlying condition as well as with surgery itself decrease insulin sensitivity. This increases glucose levels, exacerbates fluid losses, and may initiate DKA. On the other hand, caloric intake is usually restricted, which decreases glucose levels. The net effect is as difficult to predict as during an infection. Vigilant monitoring and frequent insulin adjustments are required to maintain euglycemia and avoid ketosis.

130
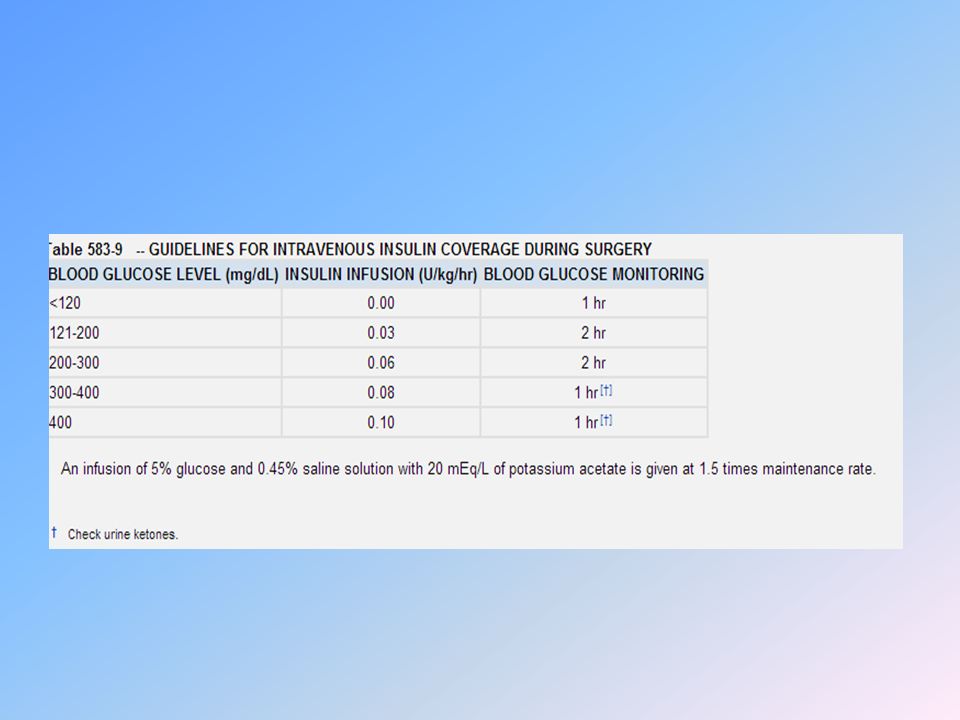
Maintaining glucose control and avoiding DKA are best accomplished with IV insulin and fluids. A simple insulin adjustment scale based on the patient's weight and blood glucose level can be used in most situations The IV insulin is continued after surgery as the child begins to take oral fluids; the IV fluids can be steadily decreased as oral intake increases. When full oral intake is achieved, the IV may be capped and subcutaneous insulin begun. When surgery is elective, it is best performed early in the day, allowing the patient maximal recovery time to restart oral intake and subcutaneous insulin therapy.

131
When elective surgery is brief (less than 1 hr) and full oral intake is expected shortly afterward, one may simply monitor the blood glucose hourly and give a dose of insulin analog according to the child's home glucose correction scale. If glargine or detemir is used as the basal insulin, a full dose is given the evening before planned surgery. If NPH or Lente is used, one half of the morning dose is given before surgery. The child should not be discharged until blood glucose levels are stable and oral intake is tolerated.

Similar presentations





























. 2 Hyperglycaemia Learning objectives >Can state what hyperglycaemia is >Is aware of the short term and.>")











>")


. Type 2 DM 90% of diabetics (in USA) Develops gradually may be without obvious symptoms may be detected by routine screening.>")