Download presentation
Presentation is loading. Please wait.

1
1394 Annual Scientific Meeting Of Obstetricians and Gynecologists
In The Name of God Adjuvant endocrine therapy for non-metastatic, hormone receptor-positive breast cancer Dr Fariba behnamfar Associate Prof. Annual Isfahan University of Medical Sciences 1394 Annual Scientific Meeting Of Obstetricians and Gynecologists

2
Adjuvant endocrine therapy for non-metastatic, hormone receptor-positive breast cancer
The selective estrogen receptor modulator (SERM) tamoxifen ●Aromatase inhibitors, which block the peripheral conversion of androgens to estrogens. ●Ovarian suppression or ablation, which inhibits endogenous estrogen production from the ovaries, which can be done on a temporary basis (ovarian suppression) or permanently through oophorectomy or radiation therapy ,ablation
 tamoxifen. ●Aromatase inhibitors, which block the peripheral conversion of androgens to estrogens. ●Ovarian suppression or ablation, which inhibits endogenous estrogen production from the ovaries, which can be done on a temporary basis (ovarian suppression) or permanently through oophorectomy or radiation therapy ,ablation.")
3
Endocrine therapy For women who appear to not be at a high risk of recurrence, we administer tamoxifen as single-agent therapy. For women with high-risk breast cancer, we offer ovarian suppression plus exemestane rather than tamoxifen as single- agent therapy

4
SOFT trial In the SOFT trial, over 3000 premenopausal women were randomly assigned to one of three arms: tamoxifen alone, tamoxifen plus ovarian suppression, or exemestane plus ovarian suppression Women were allowed to enter following surgery alone (in which case they were randomized within 12 weeks of surgery) or within eight months of the end of chemotherapy, provided they had biochemical proof they were not menopausal. With a median follow-up of 67 months, compared with tamoxifen alone, tamoxifen plus ovarian suppression resulted in: ●No statistically significant difference in DFS at five years (HR 0.83, 95% CI ) ●A higher rate of serious (grade 3) toxicities (31 versus 23.7 percent, respectively). These included menopausal symptoms and depression
 or within eight months of the end of chemotherapy, provided they had biochemical proof they were not menopausal. With a median follow-up of 67 months, compared with tamoxifen alone, tamoxifen plus ovarian suppression resulted in: ●No statistically significant difference in DFS at five years (HR 0.83, 95% CI ) ●A higher rate of serious (grade 3) toxicities (31 versus 23.7 percent, respectively). These included menopausal symptoms and depression.")
5
SOFT trial patients with a higher risk of relapse may derive a benefit from ovarian suppression plus either aromatase inhibition or tamoxifen These include: ●Patients who were treated with chemotherapy ●Patients <35 years at diagnosis of breast cancer The results of the subgroup analysis of the SOFT trial suggest that patients with sufficiently higher-risk breast cancer that warranted chemotherapy administration may benefit from ovarian suppression plus aromatase inhibition or tamoxifen Adjuvant ovarian suppression in premenopausal breast cancer. Francis PA, Regan MM, Fleming GF..SOFT Investigators, International Breast Cancer Study Group N Engl J Med. 2015;372(5):436.
:436.")
6
Tamoxifen Tamoxifen is a selective estrogen receptor modulator (SERM) that inhibits the growth of breast cancer cells by competitive antagonism of the estrogen receptor (ER). It is the endocrine agent of choice for the adjuvant treatment of premenopausal women and for postmenopausal women who are not candidates for an aromatase inhibitor (AI) for whatever reason.
 that inhibits the growth of breast cancer cells by competitive antagonism of the estrogen receptor (ER). It is the endocrine agent of choice for the adjuvant treatment of premenopausal women and for postmenopausal women who are not candidates for an aromatase inhibitor (AI) for whatever reason.")
7
Managing the side effects of tamoxifen
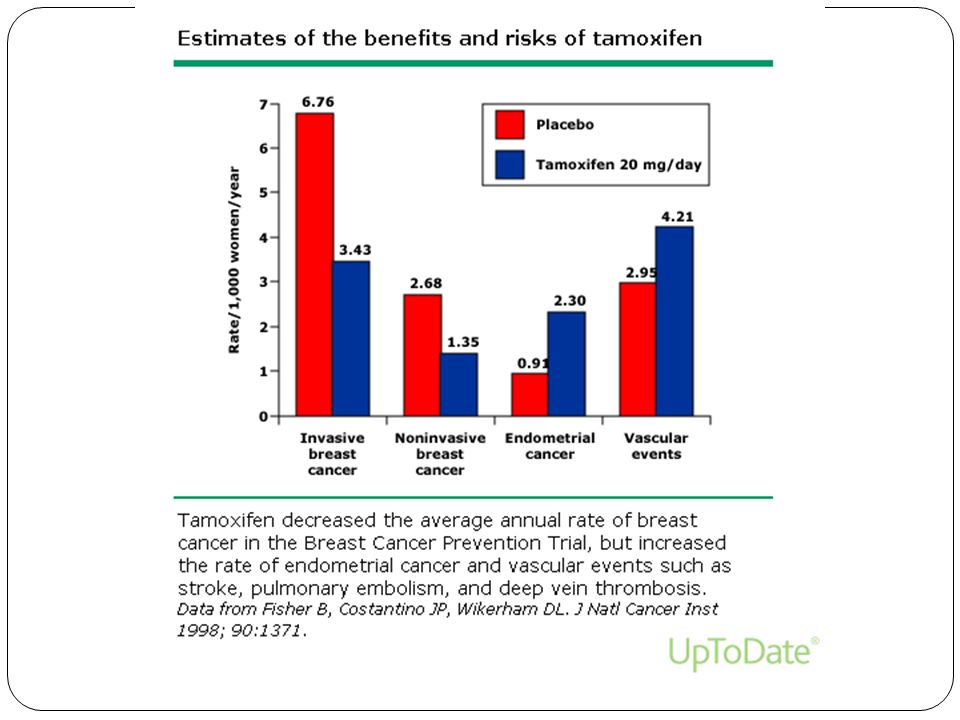
Tamoxifen and raloxifene are selective estrogen receptor modulators (SERMs) with both agonist and antagonist properties, depending on the individual target organ Both tamoxifen and raloxifene have antiestrogenic activity in breast tissue, reducing epithelial cell proliferation. This property has led to their clinical study as breast cancer chemopreventive agents However, an important difference between the two drugs is their effect on the uterus, where tamoxifen has an estrogen-like effect while raloxifene acts as an estrogen antagonist. In apparent contrast to raloxifene, tamoxifen has been associated with endometrial hyperplasia , fibroids, polyps , and endometrial tumors Endometrial cancer in tamoxifen-treated breast cancer patients: findings from the National Surgical Adjuvant Breast and Bowel Project (NSABP) B-14.Fisher B, Costantino JP, Redmond CK, J Natl Cancer Inst
 with both agonist and antagonist properties, depending on the individual target organ Both tamoxifen and raloxifene have antiestrogenic activity in breast tissue, reducing epithelial cell proliferation. This property has led to their clinical study as breast cancer chemopreventive agents. However, an important difference between the two drugs is their effect on the uterus, where tamoxifen has an estrogen-like effect while raloxifene acts as an estrogen antagonist. In apparent contrast to raloxifene, tamoxifen has been associated with endometrial hyperplasia , fibroids, polyps , and endometrial tumors. Endometrial cancer in tamoxifen-treated breast cancer patients: findings from the National Surgical Adjuvant Breast and Bowel Project (NSABP) B-14.Fisher B, Costantino JP, Redmond CK, J Natl Cancer Inst.")
8
Managing the side effects of tamoxifen
tamoxifen can cause other side effects, including hot flashes (an estrogen antagonist effect), vaginal discharge, menstrual irregularities, sexual dysfunction, and blood clots.
, vaginal discharge, menstrual irregularities, sexual dysfunction, and blood clots.")
9
HOT FLASHES Premenopausal women have a greater increase in hot flashes
sertraline and duloxetine are moderate inhibitors. sertraline :Antidepressant, Selective Serotonin Reuptake Inhibitor nitial: 50 mg daily duloxetine :Antidepressant, Serotonin/Norepinephrine Reuptake Inhibitor US labeling: Initial: 40 to 60 mg daily; For some patients it may be desirable to start at 30 mg once daily for 1 week before increasing to 60 mg once daily

10
THROMBOEMBOLIC DISEASE
increased rate of venous thromboembolic events, especially within the first two years significant additional procoagulant effect when tamoxifen is added to chemotherapy . The relative risks of pulmonary embolism and deep vein thrombosis are increased two- to three-fold in older women receiving tamoxifen. Risk factors for tamoxifen-induced VTE include prior surgery, fracture, and immobilization. These data suggest that women receiving tamoxifen should discontinue use for several days prior to prolonged immobilization from anticipated surgery or travel Garber JE, Halabi S, Tolaney SM, ..J Natl Cancer Inst. 2010;102(13):942
:942.")
11
stroke The non-significant excess of stroke deaths (three extra per women during the first 15 years) in women treated with tamoxifen was exactly balanced by a non-significant reduction in cardiac deaths (three fewer per 1000 women during the first 15 years) . Thus, there was little net effect of tamoxifen on overall vascular mortality. Early Breast Cancer Trialists' Collaborative Group (EBCTCG), Lancet ;378(9793):771
 in women treated with tamoxifen was exactly balanced by a non-significant reduction in cardiac deaths (three fewer per 1000 women during the first 15 years) . Thus, there was little net effect of tamoxifen on overall vascular mortality. Early Breast Cancer Trialists Collaborative Group (EBCTCG), Lancet. 2011;378(9793):771.")
12
ENDOMETRIAL MALIGNANCIES
In the Adjuvant Tamoxifen: Longer Against Shorter (ATLAS) trial, which randomly assigned over 15,000 women to a 10 versus 5 year course of tamoxifen, the cumulative risk of endometrial cancer during years 5 to 14 was 3.1 versus 1.6 percent, respectively. This resulted in an increased mortality risk In terms of life-threatening toxicities, the two most commonly seen with tamoxifen therapy are risk of a secondary endometrial cancer and increased risk of a thromboembolic J Adv Pract Oncol Jan-Feb; 5(1): 57–6,The Long and Short of Tamoxifen Therapy: A Review of the ATLAS Trial
 trial, which randomly assigned over 15,000 women to a 10 versus 5 year course of tamoxifen, the cumulative risk of endometrial cancer during years 5 to 14 was 3.1 versus 1.6 percent, respectively. This resulted in an increased mortality risk. In terms of life-threatening toxicities, the two most commonly seen with tamoxifen therapy are risk of a secondary endometrial cancer and increased risk of a thromboembolic. J Adv Pract Oncol Jan-Feb; 5(1): 57–6,The Long and Short of Tamoxifen Therapy: A Review of the ATLAS Trial.")
13
ENDOMETRIAL MALIGNANCIES
In an updated report of the P-1 study with seven years of follow-up, 53 cases of endometrial cancer occurred in the tamoxifen group versus 17 in the placebo group (risk ratio 3.28) . In addition, there were four cases of uterine sarcoma, three in the tamoxifen group. Of the 70 total endometrial cancers, 67 were localized (stage I). The majority presented with vaginal bleeding . The increase in endometrial cancer was almost exclusively in women over the age of 50 years Gynecologic surveillance of women on tamoxifen: first do no harm. Runowicz CD J Clin Oncol. 2000;18(20):3457.
 . In addition, there were four cases of uterine sarcoma, three in the tamoxifen group. Of the 70 total endometrial cancers, 67 were localized (stage I). The majority presented with vaginal bleeding . The increase in endometrial cancer was almost exclusively in women over the age of 50 years. Gynecologic surveillance of women on tamoxifen: first do no harm. Runowicz CD J Clin Oncol. 2000;18(20):3457.")
15
ENDOMETRIAL MALIGNANCIES
A reduction in relative risk after treatment discontinuation was shown in the International Breast Cancer Study Group (IBIS)- tamoxifen chemoprevention trial, in which 7145 women at high risk for breast cancer were randomized to five years of tamoxifen or placebo Thirteen of the 17 endometrial cancers in the tamoxifen group were diagnosed during active treatment (versus 3 of 11 in the placebo group). In contrast, during the follow-up period, four endometrial cancers were diagnosed in the tamoxifen group compared to eight in the placebo group.
- tamoxifen chemoprevention trial, in which 7145 women at high risk for breast cancer were randomized to five years of tamoxifen or placebo Thirteen of the 17 endometrial cancers in the tamoxifen group were diagnosed during active treatment (versus 3 of 11 in the placebo group). In contrast, during the follow-up period, four endometrial cancers were diagnosed in the tamoxifen group compared to eight in the placebo group.")
16
Screening for uterine tumors
The American College of Obstetricians and Gynecologists has developed the following recommendations for monitoring women on tamoxifen ●Premenopausal women have no known increased risk of uterine cancer with tamoxifen and require no additional monitoring beyond routine gynecologic care. ●For postmenopausal women, perform an annual gynecologic examination. ●Monitor for symptoms of endometrial hyperplasia or cancer. Women should be educated to report any abnormal vaginal symptoms (eg, bloody discharge, spotting, staining, leukorrhea). ●Investigate any abnormal vaginal symptoms. ●Limit tamoxifen use to five years duration because benefit beyond this time has not been demonstrated. ●If atypical endometrial hyperplasia develops, the use of tamoxifen should be reassessed and appropriate gynecologic management should be initiated. Hysterectomy should be considered for women with atypical endometrial hyperplasia in whom tamoxifen therapy must be continued.
. ●Investigate any abnormal vaginal symptoms. ●Limit tamoxifen use to five years duration because benefit beyond this time has not been demonstrated. ●If atypical endometrial hyperplasia develops, the use of tamoxifen should be reassessed and appropriate gynecologic management should be initiated. Hysterectomy should be considered for women with atypical endometrial hyperplasia in whom tamoxifen therapy must be continued.")
17
Gynecologic and ultrasound examination
There are no evidence-based recommendations for uterine cancer screening in women taking tamoxifen; investigators from the P-1 study recommend annual gynecologic examinations and a thorough evaluation of abnormal bleeding The utility of transvaginal ultrasound is unproven. One prospective study evaluated semiannual transvaginal ultrasound (TVUS) to screen for endometrial pathology in 247 asymptomatic women receiving tamoxifen
 to screen for endometrial pathology in 247 asymptomatic women receiving tamoxifen.")
18
Gynecologic and ultrasound examination
The endometrial thickness increased from a mean of 3.5 mm pretreatment to 9.2 mm after three years of tamoxifen, a value that was significantly greater than controls (n = 98) [34]. Even with a cutoff value of 10 mm for abnormal endometrial thickness, screening TVUS resulted in a high false positive rate and substantial iatrogenic morbidity. Histologically, endometrial cancer was detected in only one case, atrophy in 38 (73 percent), polyps in nine, and hyperplasia in four. Four of 52 hysteroscopy and D&C procedures, which were prompted by abnormal TVUS findings, were complicated by uterine perforations.
 [34]. Even with a cutoff value of 10 mm for abnormal endometrial thickness, screening TVUS resulted in a high false positive rate and substantial iatrogenic morbidity. Histologically, endometrial cancer was detected in only one case, atrophy in 38 (73 percent), polyps in nine, and hyperplasia in four. Four of 52 hysteroscopy and D&C procedures, which were prompted by abnormal TVUS findings, were complicated by uterine perforations.")
19
Gynecologic and ultrasound examination
Furthermore, pelvic ultrasound should be interpreted with caution, as up to 25 percent of asymptomatic women ontamoxifen have ultrasonographic changes that are suggestive of endometrial cancer, but that are not associated with endometrial pathology [35-38]. Endometrial polyps appear to be the most common endometrial pathology [39]

20
Endometrial biopsy Endometrial biopsy — Likewise, routine endometrial biopsy in asymptomatic women on tamoxifen is not useful . A prospective study of semiannual screening office endometrial biopsies was performed in 159 asymptomatic women beginning adjuvant tamoxifen. An average of 5.8 endometrial biopsies were performed per patient, and no cases of endometrial cancer were diagnosed. However, screening led to an increase in operative procedures; fourteen of 111 assessable patients (13 percent) underwent D&C (all for benign pathology) and three underwent hysterectomy.
 underwent D&C (all for benign pathology) and three underwent hysterectomy.")
21
Endometrial protection
Endometrial protection — Endometrial protection from the effects of tamoxifen may be possible with local application of the levonorgestrel-releasing intrauterine device (LNG-IUD), a progestational agent. While LNG-IUD may prevent polyps and other endometrial issues among women taking tamoxifen, it may increase the risk of cancer recurrence; these data are reviewed below. Until more data becomes available, we suggest not administering LNG-IUD for endometrial protection.
, a progestational agent. While LNG-IUD may prevent polyps and other endometrial issues among women taking tamoxifen, it may increase the risk of cancer recurrence; these data are reviewed below. Until more data becomes available, we suggest not administering LNG-IUD for endometrial protection.")
22
In a 2009 systematic review of two randomized trials of LNG-IUD versus endometrial surveillance in women ontamoxifen as adjuvant treatment for hormone-positive breast cancer, compared to surveillance, LNG-IUD use resulted in [43]: •A significant reduction in the incidence of endometrial polyps (1.6 versus 10.6 percent, respectively, odds ratio [OR] 0.14, 95% CI ) •A trend towards a lower incidence of endometrial hyperplasia (OR 0.30, 95% CI ) •A trend towards a lower incidence of endometrial fibroids (1.6 versus 4.1 percent, OR 0.37, 95% CI )
![In a 2009 systematic review of two randomized trials of LNG-IUD versus endometrial surveillance in women ontamoxifen as adjuvant treatment for hormone-positive breast cancer, compared to surveillance, LNG-IUD use resulted in [43]:](http://slideplayer.com/slide/8942144/27/images/22/In+a+2009+systematic+review+of+two+randomized+trials+of+LNG-IUD+versus+endometrial+surveillance+in+women+ontamoxifen+as+adjuvant+treatment+for+hormone-positive+breast+cancer%2C+compared+to+surveillance%2C+LNG-IUD+use+resulted+in+%5B43%5D%3A.jpg "•A significant reduction in the incidence of endometrial polyps (1.6 versus 10.6 percent, respectively, odds ratio [OR] 0.14, 95% CI ) •A trend towards a lower incidence of endometrial hyperplasia (OR 0.30, 95% CI ) •A trend towards a lower incidence of endometrial fibroids (1.6 versus 4.1 percent, OR 0.37, 95% CI )")
23
A European study retrospectively evaluated the risk of recurrence among women with breast cancer in LNG-IUD users (n = 79) and nonusers (n = 120), matched for age, breast cancer characteristics (ie, stage, grade), and previous treatments [44]. Compared to non-users, use of the LNG-IUD resulted in a slightly higher rate of breast cancer recurrence (22 versus 17 percent, OR 1.86, 95% ). However, the timing of initiation of LNG-IUD before and during breast cancer treatment was associated with risk of recurrence: •Women who initiated LNG-IUD at the time of the initial breast cancer diagnosis and continued to use it during treatment had a significantly increased risk of recurrence (hazard ratio [HR] for recurrence 3.4, 95% CI ). •Women who initiated LNG-IUD following completion of breast cancer treatment had a trend towards an increased risk of recurrence (HR 1.48, 95% CI
![A European study retrospectively evaluated the risk of recurrence among women with breast cancer in LNG-IUD users (n = 79) and nonusers (n = 120), matched for age, breast cancer characteristics (ie, stage, grade), and previous treatments [44]. Compared to non-users, use of the LNG-IUD resulted in a slightly higher rate of breast cancer recurrence (22 versus 17 percent, OR 1.86, 95% ). However, the timing of initiation of LNG-IUD before and during breast cancer treatment was associated with risk of recurrence:](http://slideplayer.com/slide/8942144/27/images/23/A+European+study+retrospectively+evaluated+the+risk+of+recurrence+among+women+with+breast+cancer+in+LNG-IUD+users+%28n+%3D+79%29+and+nonusers+%28n+%3D+120%29%2C+matched+for+age%2C+breast+cancer+characteristics+%28ie%2C+stage%2C+grade%29%2C+and+previous+treatments+%5B44%5D.+Compared+to+non-users%2C+use+of+the+LNG-IUD+resulted+in+a+slightly+higher+rate+of+breast+cancer+recurrence+%2822+versus+17+percent%2C+OR+1.86%2C+95%25+%29.+However%2C+the+timing+of+initiation+of+LNG-IUD+before+and+during+breast+cancer+treatment+was+associated+with+risk+of+recurrence%3A.jpg "•Women who initiated LNG-IUD at the time of the initial breast cancer diagnosis and continued to use it during treatment had a significantly increased risk of recurrence (hazard ratio [HR] for recurrence 3.4, 95% CI ). •Women who initiated LNG-IUD following completion of breast cancer treatment had a trend towards an increased risk of recurrence (HR 1.48, 95% CI")
24
CORONARY HEART DISEASE
Tamoxifen has favorable effects on the lipid profile that may influence coronary heart disease

25
Tamoxifen has been associated with an increased risk of endometrial cancer, and the risk increases further if treatment is extended beyond five years. (See 'Endometrial malignancies' above.). There are no evidence-based recommendations for uterine cancer screening in women taking tamoxifen. The American College of Obstetricians and Gynecologists recommend the following for monitoring women on tamoxifen
. There are no evidence-based recommendations for uterine cancer screening in women taking tamoxifen. The American College of Obstetricians and Gynecologists recommend the following for monitoring women on tamoxifen.")
26
Premenopausal women have no known increased risk of uterine cancer with tamoxifen and require no additional monitoring beyond routine gynecologic care. •For postmenopausal women, perform an annual gynecologic examination. •Monitor for symptoms of endometrial hyperplasia or cancer. Women should be educated to report any abnormal vaginal symptoms (eg, bloody discharge, spotting, staining, leukorrhea). •Investigate any abnormal vaginal symptoms. •Limit tamoxifen use to five years duration; benefit beyond this time has not been proven, and may be harmful. .
. •Investigate any abnormal vaginal symptoms. •Limit tamoxifen use to five years duration; benefit beyond this time has not been proven, and may be harmful. .")
27
If atypical endometrial hyperplasia develops, the use of tamoxifen should be reassessed and appropriate gynecologic management should be initiated. Hysterectomy should be considered for women with atypical endometrial hyperplasia in whom tamoxifen therapy must be continued American College of Obstetricians and Gynecologists. Tamoxifen and endometrial cancer. ACOG Committee Opinion 336. ACOG June 2006; Washington, DC.

28
Summary women receiving tamoxifen should discontinue use for several days prior to prolonged immobilization from anticipated surgery or travel sertraline and duloxetine are moderate inhibitors of hot flushes

Similar presentations

:886-904 Key points from the 2013 Position Statement of The North American Menopause Society.>")


: Department.>")






>")








 Recommendations of the International Society of Geriatric Oncology Surgical.>")