Download presentation
Presentation is loading. Please wait.

1
Acute Myeloid Leukemia (AML)
Dr. Ravi Kant Assistant Professor Department of General Medicine

2
Introduction The myeloid leukemias are a heterogeneous group of diseases characterized by infiltration of the blood, bone marrow, and other tissues by neoplastic cells of the hematopoietic system. Based on their untreated course, the myeloid leukemias have traditionally been designated acute or chronic.

3
Incidence The incidence of acute myeloid leukemia (AML) is 3.5 per 100,000 people per year, and the age- adjusted incidence is higher in men than in women. AML incidence increases with age. Etiology Heredity, radiation, chemical and other occupational exposures, and drugs have been implicated in the development of AML.
 is 3.5 per 100,000 people per year, and the age- adjusted incidence is higher in men than in women. AML incidence increases with age. Etiology. Heredity, radiation, chemical and other occupational exposures, and drugs have been implicated in the development of AML.")
4
World Health Organization Classification
AML with recurrent genetic abnormalities AML with t(8;21)(q22;q22) AML with inv(16)(pl3.1q22) or t(16;16)(p13.1;q22) Acute promyelocytic leukemia with t(15;17)(q22;q12); AML with t(9;11)(p22;q23); AML with t(6;9)(p23;q34); AML with inv(3)(q21q26.2) or t(3;3)(q21;q26.2); AML (megakaryoblastic) with t(1;22)(p13;q13);
(q22;q22) AML with inv(16)(pl3.1q22) or t(16;16)(p13.1;q22) Acute promyelocytic leukemia with t(15;17)(q22;q12); AML with t(9;11)(p22;q23); AML with t(6;9)(p23;q34); AML with inv(3)(q21q26.2) or t(3;3)(q21;q26.2); AML (megakaryoblastic) with t(1;22)(p13;q13);")
5
AML with myelodysplasia-related changes
Therapy-related myeloid neoplasms AML not otherwise specified AML with minimal differentiation AML without maturation AML with maturation Acute myelomonocytic leukemia Acute monoblastic and monocytic leukemia Acute erythroid leukemia Acute megakaryoblastic leukemia Acute basophilic leukemia Acute panmyelosis with myelofibrosis Myeloid sarcoma

6
Myeloid proliferations related to Down syndrome
Transient abnormal myelopoiesis Myeloid leukemia associated with Down syndrome Blastic plasmacytoid dendritic cell neoplasm Acute leukemia of ambiguous lineage Acute undifferentiated leukemia Mixed phenotype acute leukemia with t(9;22)(q34;q11,20) Mixed phenotype acute leukemia with t(v;11q23); Mixed phenotype acute leukemia,
(q34;q11,20) Mixed phenotype acute leukemia with t(v;11q23); Mixed phenotype acute leukemia,")
7
French-American-British (FAB) Classification
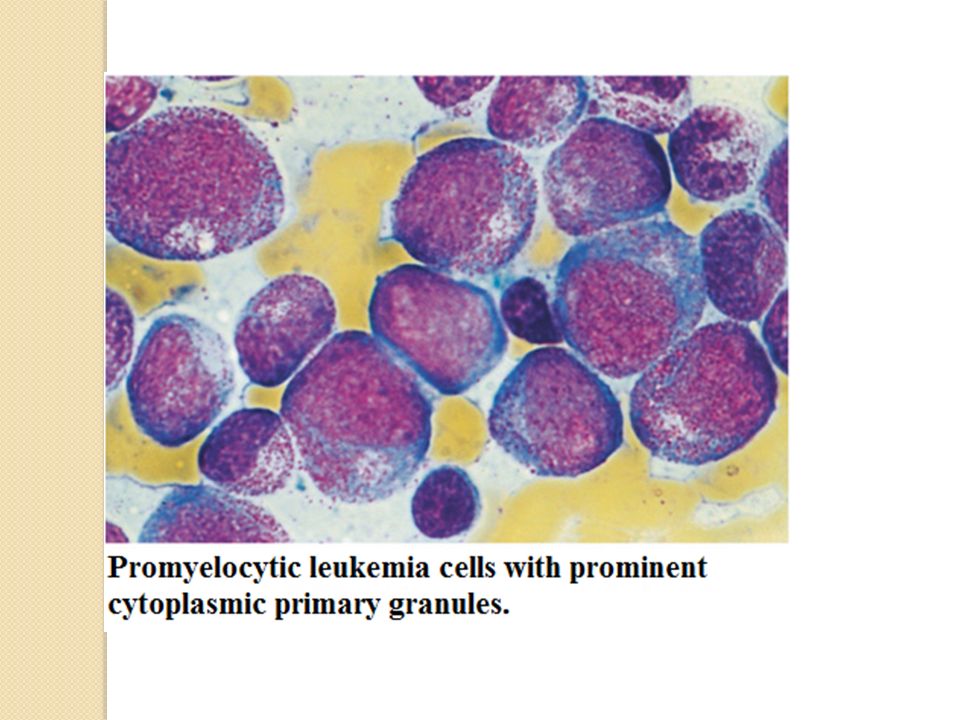
MO: Minimally differentiated leukemia Ml: Myeloblastic leukemia without maturation M2: Myeloblastic leukemia with maturation M3: Hypergranular promyelocytic leukemia M4: Myelomonocytic leukemia M4Eo: Variant: Increase in abnormal marrow eosinophils M5: Monocytic leukemia M6: Erythroleukemia (DiGuglielmo's disease) M7: Megakaryoblastic leukemia
 M7: Megakaryoblastic leukemia.")
8
A major difference between the WHO and FAB systems is the blast cutoff for a diagnosis of AML as opposed to myelodysplastic syndrome (MDS); it is 20% in the WHO classification and 30% in the FAB.
; it is 20% in the WHO classification and 30% in the FAB.")
9
Molecular Prognostic Markers in AML
Marker Location Prognostic Impact NPM1 mutation 5q35 Favorable CEBPA mutation 19q13.1 FLT3-ITD 13q12 Adverse WT1 mutation 11p13 KIT mutation 4q11-q12 BAALC overexpression 8q22.3 ERG overexpression 21q22.3 MN1 overexpression 22q12.1 EVI1 overexpression 3q26

10
Clinical Presentation
Symptoms Patients with AML most often present with nonspecific symptoms that begin gradually or abruptly and are the consequence of anemia, leukocytosis, leukopenia or leukocyte dysfunction, or thrombocytopenia. Nearly half have had symptoms for 3 months before the leukemia was diagnosed. Half mention fatigue as the first symptom, but most complain of fatigue or weakness at the time of diagnosis.

11
Anorexia and weight loss are common
Anorexia and weight loss are common. Fever with or without an identifiable infection is the initial symptom in 10% of patients. Signs of abnormal hemostasis (bleeding, easy bruising) are noted first in 5% of patients. On occasion, bone pain, lymphadenopathy, nonspecific cough, headache, or diaphoresis is the presenting symptom.
 are noted first in 5% of patients. On occasion, bone pain, lymphadenopathy, nonspecific cough, headache, or diaphoresis is the presenting symptom.")
12
Physical Findings Fever, splenomegaly, hepatomegaly, lymphadenopathy, sternal tenderness, and evidence of infection and hemorrhage are often found at diagnosis. Significant gastrointestinal bleeding, intrapulmonary hemorrhage, or intracranial hemorrhage occur most often in APL. Bleeding associated with coagulopathy may also occur in monocytic AML and with extreme degrees of leukocytosis or thrombocytopenia in other morphologic subtypes. Retinal hemorrhages are detected in 15% of patients.

13
Hematologic Findings The anemia is usually normocytic normochromic. Decreased erythropoiesis often results in a reduced reticulocyte count, and red blood cell (RBC) survival is decreased by accelerated destruction. Active blood loss also contributes to the anemia. The median presenting leukocyte count is about 15,000/L.
 survival is decreased by accelerated destruction. Active blood loss also contributes to the anemia. The median presenting leukocyte count is about 15,000/L.")
14
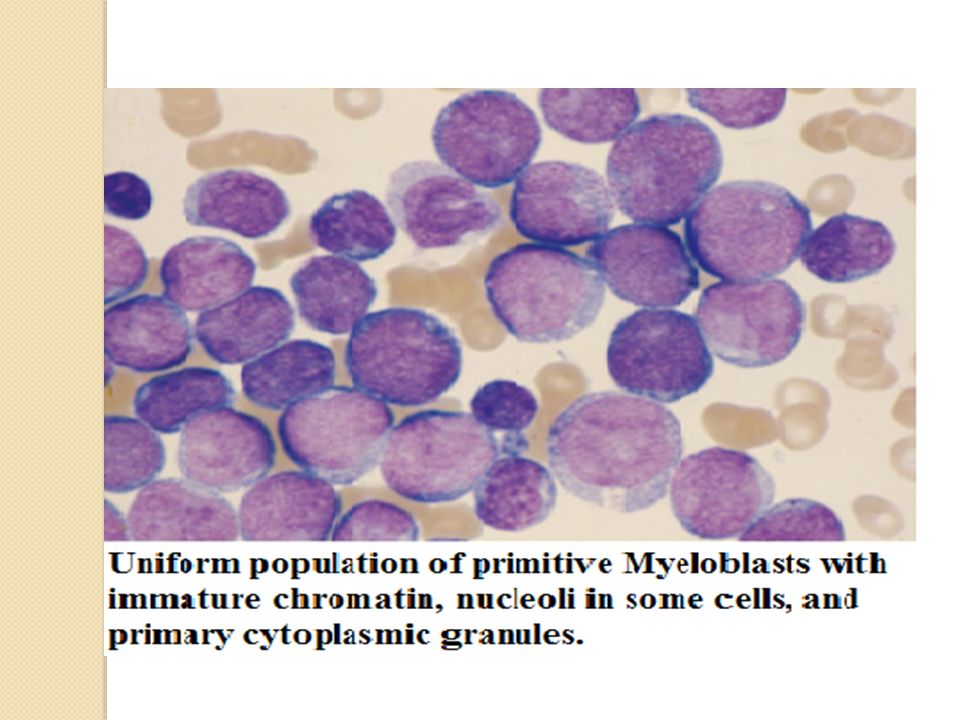
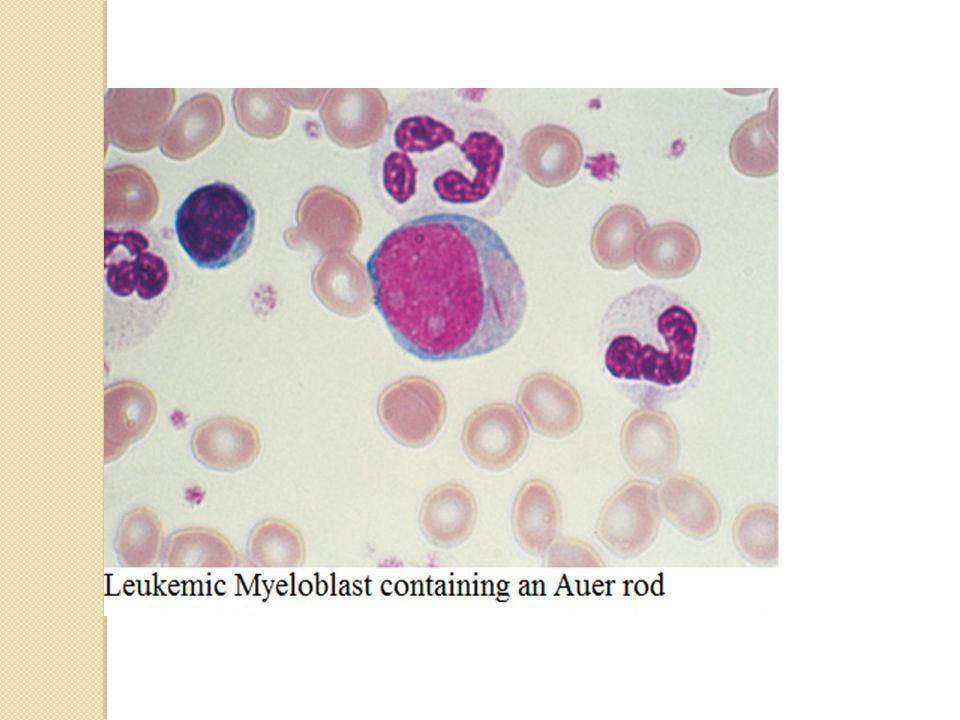
In AML, the cytoplasm often contains primary (nonspecific) granules, and the nucleus shows fine, lacy chromatin with one or more nucleoli characteristic of immature cells. Abnormal rod-shaped granules called Auer rods are not uniformly present, but when they are, myeloid lineage is virtually certain.

19
Management of Adult Patients with AML
History Increasing fatigue or decreased exercise tolerance (anemia) Excess bleeding or bleeding from unusual sites (DIC, thrombocytopenia) Fevers or recurrent infections (granulocytopenia) Headache, vision changes, nonfocal neurologic abnormalities (CNS leukemia or bleed) Early satiety (splenomegaly) Family history of AML (Fanconi, Bloom, or Kostmann syndromes or ataxia-telangiectasia)
 Excess bleeding or bleeding from unusual sites (DIC, thrombocytopenia) Fevers or recurrent infections (granulocytopenia) Headache, vision changes, nonfocal neurologic abnormalities (CNS leukemia or bleed) Early satiety (splenomegaly) Family history of AML (Fanconi, Bloom, or Kostmann syndromes or ataxia-telangiectasia)")
20
Physical Examination Performance status (prognostic factor)
Ecchymosis and oozing from IV sites (DIC, possible acute promyelocytic leukemia) Fever and tachycardia (signs of infection) Poor dentition, dental abscesses Skin infiltration or nodules (leukemia infiltration, most common in monocytic leukemia) Lymphadenopathy, splenomegaly, hepatomegaly
 Fever and tachycardia (signs of infection) Poor dentition, dental abscesses. Skin infiltration or nodules (leukemia infiltration, most common in monocytic leukemia) Lymphadenopathy, splenomegaly, hepatomegaly.")
21
Laboratory and Radiologic Studies
CBC with manual differential cell count Chemistry tests (electrolytes, creatinine, BUN, calcium, phosphorus, uric acid, hepatic enzymes, bilirubin, LDH, amylase, lipase) Clotting studies (prothrombin time, partial thromboplastin time, fibrinogen, D-dimer) Viral serologies (CMV, HSV-1, varicella-zoster) RBC type and screen HLA typing for potential allogeneic HSCT Bone marrow aspirate and biopsy (morphology, cytogenetics, flow cytometry.
 Clotting studies (prothrombin time, partial thromboplastin time, fibrinogen, D-dimer) Viral serologies (CMV, HSV-1, varicella-zoster) RBC type and screen. HLA typing for potential allogeneic HSCT. Bone marrow aspirate and biopsy (morphology, cytogenetics, flow cytometry.")
23
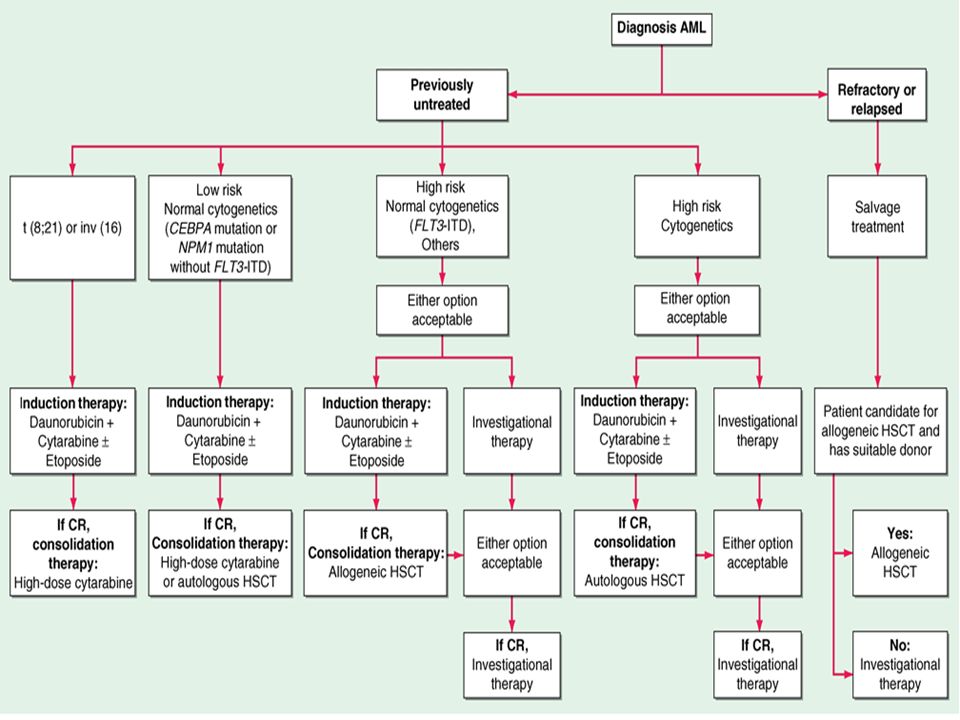
Treatment of Adults with AML
Class of Drugs Examples of Agents in Class Tyrosine kinase inhibitors PKC412, MLN518, SU11248, CHIR-258, imatinib (STI571, Gleevec), dasatinib, AMN107 Demethylating agents Decitabine, 5-azacytidine Histone deacetylase inhibitors Suberoylanilide hydroxamic acid (SAHA), MS275, LBH589, valproic acid Heavy metals Arsenic trioxide Farnesyl transferase inhibitors R115777, SCH66336 HSP-90 antagonists 17-allylaminogeldanamycin (17-AAG), DMAG, or derivatives Cell cycle inhibitors Flavopiridol, CYC202 (R-Roscovitine), SNS-032 Nucleoside analogues Clofarabine, troxacitabine Humanized antibodies Anti-CD33 (SGN33), anti-KIR Toxin-conjugated antibodies Gemtuzumab ozogamicin Proteasome inhibitors Bortezomib Aurora inhibitors AZD1152, MLN-8237, AT9283 Immunomodulatory Lenalidomide, IL-2, histamine dihydrochloride
, dasatinib, AMN107. Demethylating agents. Decitabine, 5-azacytidine. Histone deacetylase inhibitors. Suberoylanilide hydroxamic acid (SAHA), MS275, LBH589, valproic acid. Heavy metals. Arsenic trioxide. Farnesyl transferase inhibitors. R115777, SCH HSP-90 antagonists. 17-allylaminogeldanamycin (17-AAG), DMAG, or derivatives. Cell cycle inhibitors. Flavopiridol, CYC202 (R-Roscovitine), SNS-032. Nucleoside analogues. Clofarabine, troxacitabine. Humanized antibodies. Anti-CD33 (SGN33), anti-KIR. Toxin-conjugated antibodies. Gemtuzumab ozogamicin. Proteasome inhibitors. Bortezomib. Aurora inhibitors. AZD1152, MLN-8237, AT9283. Immunomodulatory. Lenalidomide, IL-2, histamine dihydrochloride.")
24
THE END

Similar presentations
1 CHILDHOOD LEUKAEMIA. TA OGUNLESI (FWACP)2 LEUKAEMIA Heterogenous group of malignant disorders Characterised by uncontrolled clonal.>")


















:>")