Download presentation
Presentation is loading. Please wait.

1
Clinical diagnostic biochemistry - 15 Dr. Maha Al-Sedik 2015 CLS 334

3
The thyroid gland secretes two hormones: T4 thyroxine (3,5,3',5'- L- tetraiodothyronine) T 3 triiodothyronine (3,5,3'-L triiodothyronine) Thyroid hormones T 4T3
 T 3 triiodothyronine (3,5,3 -L triiodothyronine) Thyroid hormones T 4T3")
4
The biosynthesis of thyroid hormones involves the Trapping of circulating iodide by the thyroid gland. Formation of thyoglobulin. Incorporation of iodine into tyrosine. Coupling of iodinated tyrosin. Endocytosis of thyroglobulin in the thyroid follicle cells. Proteolysis of the thyroglobulin to t3, t4 and protein. Releases the t3 and t4 into the circulation. Biosynthesis

8
Di iodotyrosin + Di iodotyrosin = T4 Di iodotyrosin + monoiodotyrosin = T3

9
Metabolism: Free (unbound) T4 (FT4) is the primary secretory product of the normal thyroid gland. T4 undergoes peripheral deiodination to yield T3. This deiodination occurs in a number of tissues but primarily in the liver.

10
T3 is 3 - 8 times more metabolically active than T4 and often considered to be the active form of thyroid hormone, while T4 is prehormone.

11
TSH stimulates: (1)The "iodide pump" (2)Thyroglobulin synthesis. (3)TSH also regulates the rate of proteolysis of thyroglobulin for the liberation of t4 and T3. (4)Induces an increase in the size and number of the thyroid Follicular cells. TSH function
TSH also regulates the rate of proteolysis of thyroglobulin for the liberation of t4 and T3. (4)Induces an increase in the size and number of the thyroid Follicular cells. TSH function.")
12
Almost all laboratory tests for thyroid function are commercially available in either kit form or on automated immunoassay instruments. Analytical methodology

13
Immunoassay is the method of choice for the measurement of serum TSH in the clinical laboratory. Clinically, these assays are capable of measuring TSH at concentrations required to accurately differentiate. Determination of TSH:

14
Immunoassays of total T4 measure both free and protein bound thyroxine. 99.97% of T4 circulates tightly bound to Thyroid Binding Globulin or albumin. ELISA has been developed for serum T4 determinations. These procedures are rapid and simple to use and have been applied to several major automated instruments. Determination of thyroxine:

20
Thyroid function tests: Several thyroid function tests (TFTs) are used to evaluate thyroid status: Thyroid-Stimulating Hormone. T3 and T4 Levels. Antibodies: Autoantibodies of clinical interest in thyroid disease include thyroid-stimulating antibodies (TSAb) and TSH receptor- binding inhibitory immunoglobulins (TBII). Radioactive Iodine Uptake (RAIU).
 and TSH receptor- binding inhibitory immunoglobulins (TBII). Radioactive Iodine Uptake (RAIU)..")
22
Causes of hyperthyroidism Primary ( low or normal TSH) Secondary (high TSH)
 Secondary (high TSH)")
23
Causes of Hyperthyroidism: 1- Primary: autoimmune disorder Graves’ disease: In this disorder, the body makes an antibody called thyroid- stimulating immunoglobulin (TSI) that causes the thyroid gland to make too much thyroid hormone. Graves’ disease is the most common cause.

24
toxic nodular or multinodular goiter: which are lumps or nodules in the thyroid gland that cause the thyroid to produce excessive amounts of thyroid hormones.

25
inflammation of the thyroid gland, called thyroiditis, : resulting from a problem with the immune system may temporarily cause symptoms of hyperthyroidism (thyroiditis causes T4 and T3 to leak out of the gland). Consumption of too much iodine: (either from foods or supplements) or who take medications containing iodine may cause the thyroid gland to overproduce thyroid hormones.
 or who take medications containing iodine may cause the thyroid gland to overproduce thyroid hormones..")
26
2- Secondary: Hypersecretion of thyroid stimulating hormone (TSH), which is caused by a pituitary adenoma.
, which is caused by a pituitary adenoma.")
27
How to differentiate between primary and secondary hyperthyroidism? By measuring TSH : If it is high : it is secondary hypothyroidism. If it is low : It is primary hypothyroidism.

28
Hypothyroidism

30
Causes of hypothyroidism: Diseases of the: I- Thyroid (primary hypothyroidism) : 95 % II- Pituitary (secondary hypothyroidism) : 4 % Pituitary tumor III- Hypothalamus (tertiary hypothyroidism) : < 1 %
 : 95 % II- Pituitary (secondary hypothyroidism) : 4 % Pituitary tumor III- Hypothalamus (tertiary hypothyroidism) : < 1 %")
31
Etiologies of Primary Hypothyroidism: Autoimmune : most common. Post thyroidectomy. External radiation. Antithyroid drugs (including lithium). Inherited enzymatic defect.
. Inherited enzymatic defect..")
32
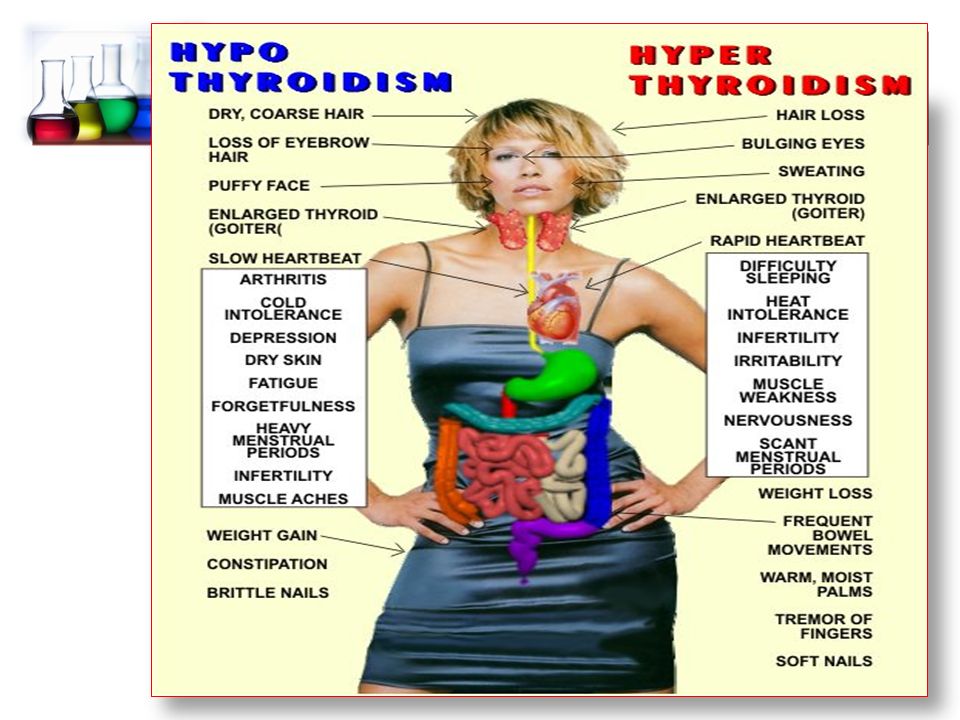
Symptoms of Hypothyroidism: Cold intolerance. Anorexia. Constipation. Amenorrhea. Fatigue. Depression. Decreased attention +/- memory. Paresthesias.

33
Dry, yellow skin. Weight gain (41% of cases). Thinning, coarse hair. "Myxedema signs“ : – Puffy eyelids – Hoarse voice – edema Signs Related to Hypothyroidism:

34
Myxedema coma

35
How to differentiate between primary and secondary hypothyroidism? By measuring TSH : If it is high : it is primary hypothyroidism. If it is low : It is secondary hypothyroidism.

36
How to differentiate between secondary and tertiary hypothyroidism? By measuring ---------------- : If it is high : it is ---------------- hypothyroidism. If it is low : It is ------------------- hypothyroidism.

Similar presentations














 pages pp. 43-50 before Metabolism of thyroid hormones section; (2) pages 56 (Regulation.>")



 Triiodothyronine (T3) Calcitonin Energy & Growth Control.>")








. Its size depends on: 1. age … age size. 2. sex … female > male. 3.>")


