Download presentation
Presentation is loading. Please wait.

1
Public Health and HAIs Kathryn Turner, PHD MPH Deputy State Epidemiologist and Chief, Bureau of Communicable Disease Prevention October 23, 2015 I-APIC Annual ConferenceBoise, Idaho

2
Topics Public Health and HAI prevention National level activities Idaho HAI Program HAIs in Idaho Antimicrobial Resistance 10/23/2015

3
Public Health Involvement in healthcare-associated infection prevention 10/23/2015

4
Remember this? November 29, 1999 Establish a national focus to create leadership, research, tools, and protocols to enhance the knowledge base about safety. “Center for Patient Safety” Develop a nationwide public mandatory reporting system and by encouraging healthcare organizations and practitioners to develop and participate in voluntary reporting systems 10/23/2015

5
Why HAIs Matter to Public Health Widespread and PREVENTABLE Significantly contributes to morbidity and mortality Importance to public health increasing (economic and human impact): Increasing numbers and crowding of people More frequent impaired immunity (age, illness, treatments) New microorganisms Increasing bacterial resistance to antibiotics 10/23/2015
: Increasing numbers and crowding of people More frequent impaired immunity (age, illness, treatments) New microorganisms Increasing bacterial resistance to antibiotics 10/23/2015")
6
MRSA Experience Hospital Acquired (Most severely ill hospitalized patients) Healthcare Associated (Spreads to other patients in the healthcare environment) Community (Moves from healthcare environments to the community 10/23/2015
 Healthcare Associated (Spreads to other patients in the healthcare environment) Community (Moves from healthcare environments to the community 10/23/2015")
7
HHS Operating Divisions HHS “…has multiple methods to influence hospitals…issuing guidelines…requiring hospitals to comply with certain standards…releasing data to expand information…of the problem, and ….using hospital payment methods to encourage the reduction of HAIs.” PRIORITIZATION & COORDINATION 1,200 Recommended Practices 500 “Strongly” Recommended Practices 6 Divisions 10/23/2015

8
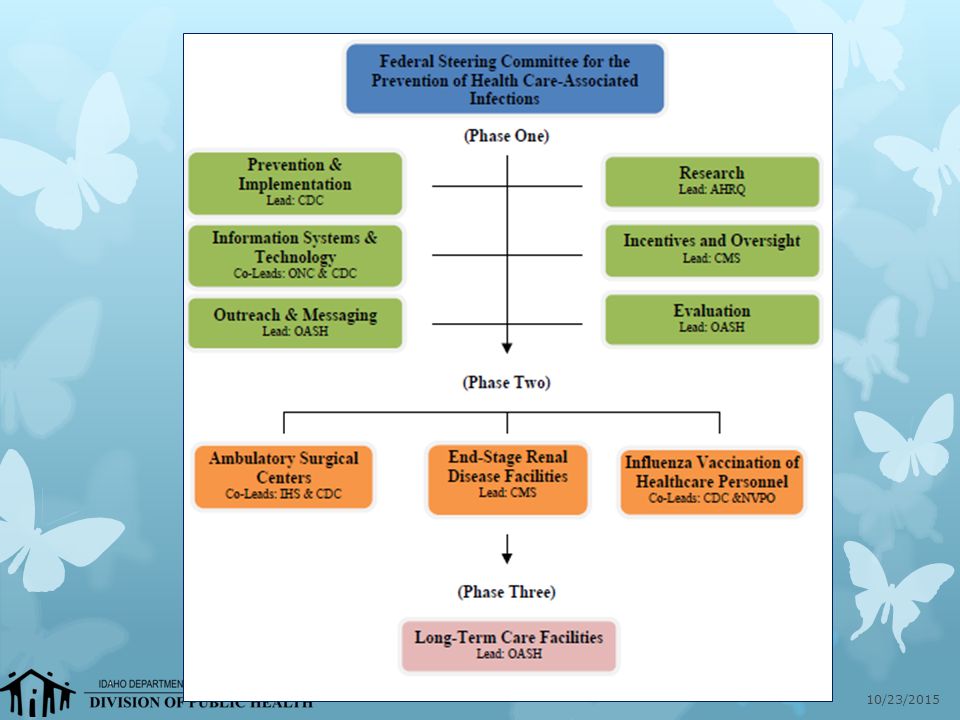
GAO Recommendations HHS Solution HHS Steering Committee for the Prevention of Healthcare Associated Infections 10/23/2015

10
National Action Plan Developed in 2009 Three phases Revised annually Accompanied by separate roadmap document 10/23/2015

11
“The Elimination of HAI’s will require (1) adherence to evidence-based practices; (2) alignment of incentives; (3) innovation through basic, translational, and epidemiological research; and (4) data to target prevention efforts and measure progress. These efforts must be underpinned by sufficient investments and resources.” -Moving toward Elimination of Healthcare Associated Infections: A Call to Action. ICHE, 11/2010: Vol 31, No 11 Pillars of HAI Elimination 10/23/2015

12
HAI Elimination: One of CDC’s Winnable Battles Promote use of National Healthcare Safety Network (NHS) data to target prevention Expand collaborations and partnerships to promote and implement proven HAI prevention practices Develop innovative approaches to prevent HAIs across the healthcare system Goals: Improve adherence to infection prevention guidelines Improve national surveillance Improve capacity at state and local health departments 10/23/2015
 data to target prevention Expand collaborations and partnerships to promote and implement proven HAI prevention practices Develop innovative approaches to prevent HAIs across the healthcare system Goals: Improve adherence to infection prevention guidelines Improve national surveillance Improve capacity at state and local health departments 10/23/2015")
13
Idaho HAI Program 10/23/2015

14
Idaho HAI Program Started: September 2009 Funding targeted to build Healthcare Associated Infections Prevention Infrastructure in State Public Health Agencies Personnel infrastructure for program Data validation, technical assistance, collaboration, NHSN training/support Infection prevention education Staffing: K. Turner / FTE through contract 10/23/2015

15
Ebola Supplemental Funding State Fiscal Year 2016 (July 1, 2015) Update Idaho’s HAI Prevention Plan Work with Idaho’s Advisory Group and expand to include other members Original: January 2010 Last update: September 2012 Inventory of all healthcare settings IC POC Available HAI-related data Current regulatory / licensing oversight 10/23/2015
 Update Idaho’s HAI Prevention Plan Work with Idaho’s Advisory Group and expand to include other members Original: January 2010 Last update: September 2012 Inventory of all healthcare settings IC POC Available HAI-related data Current regulatory / licensing oversight 10/23/2015")
16
Ebola Supplemental Funding On-site infection control assessments Minimum: all Ebola-designated assessment hospitals Identify gaps in infection control readiness Address gaps through consultation / planning Perform follow-up assessments Assess capacity of HC facilities to detect, report, respond to outbreaks Develop assessment tool as template Provide / fund training on hospital epidemiology Communication, outreach, education 10/23/2015

17
Changes to State HAI Program Idaho Hospital Association HAI “boots on the ground” contract since 2010 Project Director retired in December 2014 February 2015: IHA no longer has capacity to perform SOW Program activities moved in-house IHA Activities + expand to LTCF Programmatic oversight / reporting 10/23/2015

18
Bureau of Communicable Disease Prevention Immunization TB Program Epidemiology Operations State Public Health Vet Food Protection Refugee Health Screening Healthcare Associated Infections 10/23/2015

19
https://labor.idaho.gov/DHR/ATS/StateJobs/jobannouncement.aspx?announ cement_no=07640057044

20
Focus: HAIs and AR/AS Provide overall management of the HAI program Facilitate statewide efforts Oversee and develop program materials Grant application / reporting Evaluate HAI Surveillance TA to facilities Lead/participate in multi-disciplinary teams NHSN Group Administrator 10/23/2015

21
Healthcare Associated Infections How Idaho Compares 10/23/2015

22
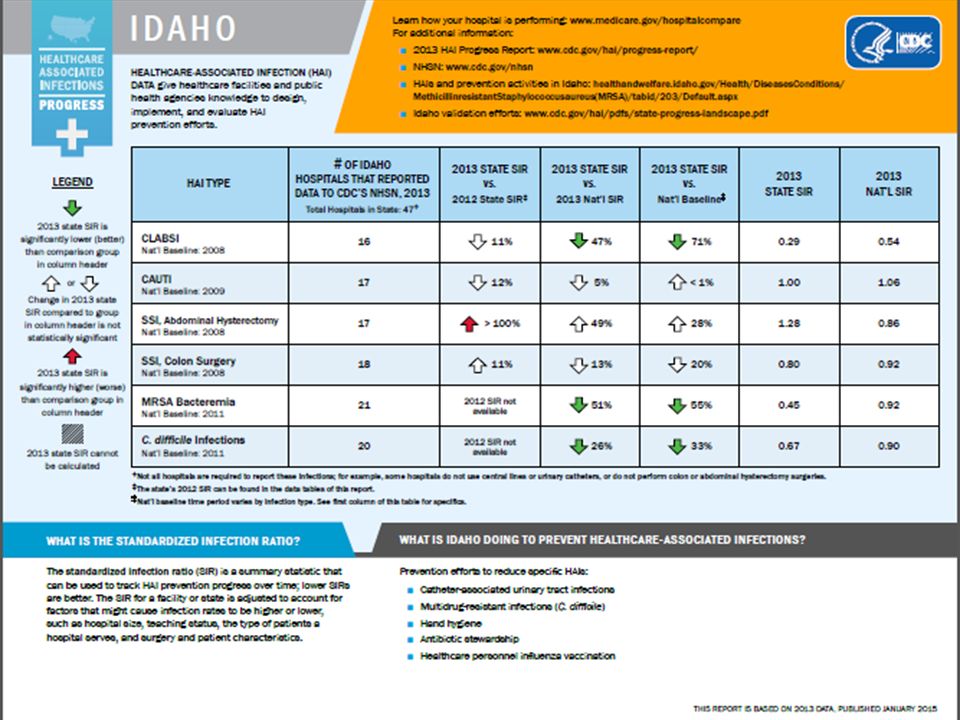
CLABSI and CAUTI rates - 2013 CENTRAL LINE ASSOCIATED BLOOD STREAM INFECTIONS (CLABSI) All Location CLABSI rates are very low compared with national rates No Idaho facilities had SIRs higher than national (0.54) Idaho SIR = 0.29 (Idaho rank: 5 th lowest) CATHETER-ASSOCIATED URINARY TRACT INFECTION (CAUTI) All Location CAUTI rates could be improved One ID facility’s SIR higher (1.270) than national (1.057) Idaho SIR = 1.003 (Idaho rank: 21 st lowest) 10/23/2015
 All Location CLABSI rates are very low compared with national rates No Idaho facilities had SIRs higher than national (0.54) Idaho SIR = 0.29 (Idaho rank: 5 th lowest) CATHETER-ASSOCIATED URINARY TRACT INFECTION (CAUTI) All Location CAUTI rates could be improved One ID facility’s SIR higher (1.270) than national (1.057) Idaho SIR = (Idaho rank: 21 st lowest) 10/23/2015")
23
Table 9. Changes in state-specific standardized infection ratios (SIRs), 2012 compared to 2013 9a. Central line-associated bloodstream infections (CLABSI), all locations 1 State 2012 SIR 2013 SIR % Change Direction of Changep-value South Dakota0.2750.19429%Decrease0.3155 Oregon0.3900.30123%Decrease0.1211 New Mexico0.6130.48621%Decrease0.1473 New Hampshire0.4330.34520%Decrease0.4769 Oklahoma0.4800.39418%Decrease0.0761 Virginia0.5780.50113%Decrease0.0540 Idaho0.3220.28711%Decrease0.7357 10/23/2015
, all locations 1 State 2012 SIR 2013 SIR % Change Direction of Changep-value South Dakota %Decrease Oregon %Decrease New Mexico %Decrease New Hampshire %Decrease Oklahoma %Decrease Virginia %Decrease Idaho %Decrease /23/2015.")
24
5/19/2015 Table 9. Changes in state-specific standardized infection ratios (SIRs), 2012 compared to 2013 9b. Catheter-associated urinary tract infections (CAUTI), all locations 1 State2012 SIR2013 SIR Percent Change Direction of Changep-value Louisiana0.8160.8091%Decrease0.8897 New Hampshire0.9560.9184%Decrease0.7976 Nebraska0.9750.9255%Decrease0.5998 Arkansas1.0991.0405%Decrease0.4579 Washington1.0741.0126%Decrease0.3658 Rhode Island1.3491.2696%Decrease0.5914 Arizona1.0921.0246%Decrease0.2732 Iowa0.9430.8846%Decrease0.5377 Illinois1.0390.9677%Decrease0.0794 Mississippi1.1921.07810%Decrease0.1458 Maine1.9061.71810%Decrease0.3609 Utah1.8391.64011%Decrease0.2204 Connecticut1.8681.65411%Decrease0.0637 Idaho1.1451.00312%Decrease0.4421
, 2012 compared to b. Catheter-associated urinary tract infections (CAUTI), all locations 1 State2012 SIR2013 SIR Percent Change Direction of Changep-value Louisiana %Decrease New Hampshire %Decrease Nebraska %Decrease Arkansas %Decrease Washington %Decrease Rhode Island %Decrease Arizona %Decrease Iowa %Decrease Illinois %Decrease Mississippi %Decrease Maine %Decrease Utah %Decrease Connecticut %Decrease Idaho %Decrease")
25
SSI and HO-MRSA BSI LabID SURGICAL SITE INFECTION (SSI) SSI following colon surgery: One ID facility’s SIR higher (1.130) than national (0.919) Idaho SIR = 0.797 (Idaho rank: 12th lowest) HOSPITAL ONSET (HO) MRSA BSI HO-MRSA BSI rates are very low compared with national rates No Idaho facilities’ SIRs higher than national (0.917) Idaho SIR = 0.452 (Idaho rank: 5 th lowest) 10/23/2015
 SSI following colon surgery: One ID facility’s SIR higher (1.130) than national (0.919) Idaho SIR = (Idaho rank: 12th lowest) HOSPITAL ONSET (HO) MRSA BSI HO-MRSA BSI rates are very low compared with national rates No Idaho facilities’ SIRs higher than national (0.917) Idaho SIR = (Idaho rank: 5 th lowest) 10/23/2015")
26
HO-C.diff LabID HOSPITAL ONSET (HO) CLOSTRIDIUM DIFFICILE HO-C. diff infection rates are very low compared with national rates No Idaho facilities’ SIRs higher than national (0.904) Idaho SIR = 0.666 (Idaho rank: 9 th lowest) 10/23/2015
 Idaho SIR = (Idaho rank: 9 th lowest) 10/23/2015.")
27
5/19/2015

29
Antimicrobial Resistance The Next Big Thing 5/19/2015

30
FOUR CORE ACTIONS Prevent infections and prevent the spread of resistance Track resistant bacteria Improve use of antibiotics Promote the development of new antibiotics and new diagnostic tests for resistant bacteria 5/19/2015

31
AR and the President’s Budget Nearly Double: >$1 billion investment in FY 2016 10/23/2015

32
Discussion – New HAI Program Manager What would you like to see happen now that the Division of Public Health will have increased HAI Program Capacity? Surveillance / data validation? Guidelines / assessments? Communication? Email me! turnerk@dhw.idaho.gov 10/23/2015

Similar presentations










 National Center for Emerging and Zoonotic Infectious Diseases Division of Healthcare.>")


 Prevention>")





