Download presentation
Presentation is loading. Please wait.

1
Journal Club 埼玉医科大学 総合医療センター 内分泌・糖尿病内科 Department of Endocrinology and Diabetes, Saitama Medical Center, Saitama Medical University 松田 昌文 Matsuda, Masafumi 2014 年 4 月 17 日 8:30-8:55 8階 医局 Tripathy D, Clement SC, Schwenke DC, Banerji M, Bray GA, Buchanan TA, Gastaldelli A, Henry RR, Kitabchi AE, Mudaliar S, Ratner RE, Stentz FB, Musi N, Reaven PD, Defronzo RA. Baseline Adiponectin Levels Do Not Influence the Response to Pioglitazone in ACT NOW. Diabetes Care. 2014 Apr 4. doi: 10.2337/dc13-1745

2
Matsuda M.;GEKKAN TOUNYOUBYOU;2,16-22,2010 2:16-22, 2010. Prevention of Diabetes Mellitus Trialpublication follow-up, year drug No. of new on-set of DM No.(total) event per 1000 person-years control No. of new on-set of DM No.(total) event per 1000 person-years Thiazolidine *DPP20050.9Troglitazone1038728.7 Placebo Metformin ILS 37 21 16 391 397 393 105.1 58.8 45.2 TRIPOD20022.5Troglitazone1711459.6Placebo37122121.3 PIPOD20063.0Pioglitazone118642.6- *DREAM20063.0Rosiglitazone306236543.1Placebo686263486.8 *ACTNOW20084.0Pioglitazone103038.3Placebo4529937.6 *CANOE20103.9Met+Rosi1410334.9Placebo41104101.1 Other (α-GI, statin, fibrate, glinide) WOSCOP20015Pravastation5729993.8Placebo8239755.5 *STOP- NIDDM20023.3Acarbose22168298.2Placebo285686125.9 BIP20046.2Bezafibrate6615668.2Placebo8014787.8 *VICTORY20094Voglibose5089713.9Placebo10688130.0 *NAVIGATOR20106.5Nateglinide1674372669.1Placebo1580374764.9
 event per 1000 person-years control No. of new on-set of DM No.(total) event per 1000 person-years Thiazolidine *DPP Troglitazone Placebo Metformin ILS TRIPOD Troglitazone Placebo PIPOD Pioglitazone *DREAM Rosiglitazone Placebo *ACTNOW Pioglitazone Placebo *CANOE Met+Rosi Placebo Other (α-GI, statin, fibrate, glinide) WOSCOP20015Pravastation Placebo *STOP- NIDDM Acarbose Placebo BIP Bezafibrate Placebo *VICTORY20094Voglibose Placebo *NAVIGATOR Nateglinide Placebo")
3
N Engl J Med 2011;364:1104-15. 72 % reduction!

4
1 Texas Diabetes Institute and University of Texas Health Science Center and Audie L. Murphy Hospital, South Texas VA Health Care System, San Antonio, TX 2 Division of Endocrinology and Metabolism, Georgetown University, Washington, DC 3 Phoenix VA Health Care System, Phoenix, AZ 4 College of Nursing and Health Innovation, Arizona State University, Phoenix, AZ 5 State University of New York Health Science Center at Brooklyn, Brooklyn, NY 6 Pennington Biomedical Research Center/Louisiana State University, Baton Rouge, LA 7 University of Southern California Keck School of Medicine, Los Angeles, CA 8 University of Texas Health Science Center, San Antonio, TX, and Cardiometabolic Risk Unit, Institute of Clinical Physiology, Pisa, Italy 9 VA San Diego Healthcare System and University of California, San Diego, San Diego, CA 10 Division of Endocrinology, Diabetes and Metabolism, University of Tennessee, Memphis, TN 11 Medstar Research Institute, Hyattsville, MD DOI: 10.2337/dc13-1745 Diabetes Care. 2014 Apr 4

5
OBJECTIVE Plasma adiponectin levels are reduced in type 2 diabetes mellitus (T2DM) and other insulin-resistant states. We examined whether plasma adiponectin levels at baseline and after pioglitazone treatment in impaired glucose tolerance (IGT) subjects were associated with improved insulin sensitivity (SI) and glucose tolerance status.
 subjects were associated with improved insulin sensitivity (SI) and glucose tolerance status..")
6
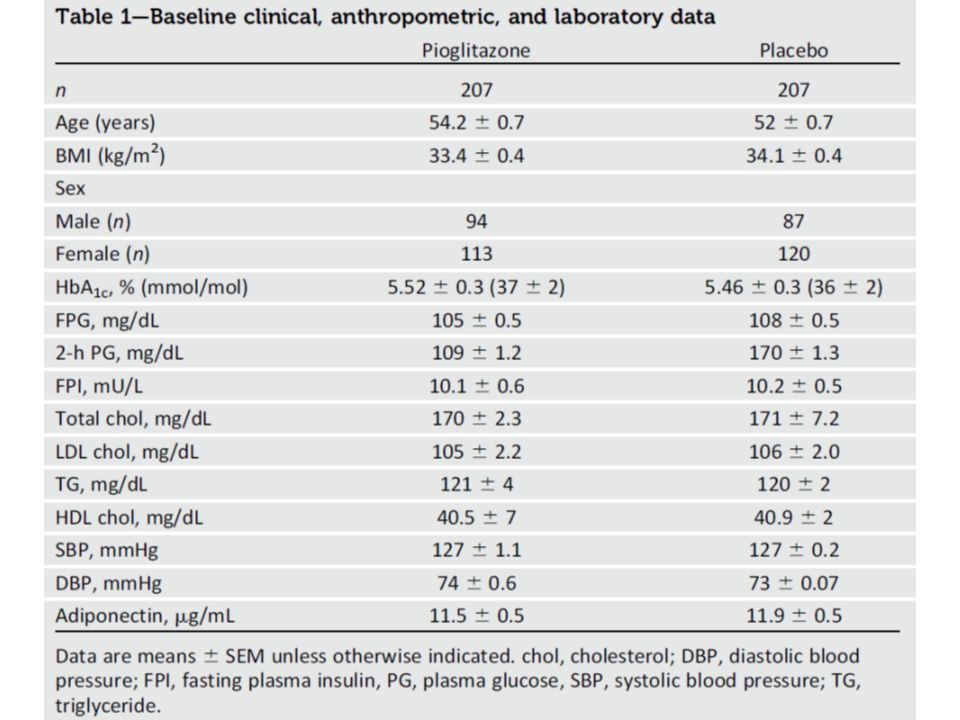
RESEARCH DESIGN AND METHODS A total of 602 high-risk IGT subjects in ACT NOW were randomized to receive pioglitazone or placebo with a median follow-up of 2.4 years.

9
Figure 1—Relationship between the mean change in plasma adiponectin concentration and final glucose tolerance status in pioglitazone-treated and placebo IGT subjects. DM, diabetes mellitus; POST, posttreatment; PRE, pretreatment.

10
Figure 2—Number of IGT subjects who developed diabetes (A) or who reverted to NGT (B) after pioglitazone (PIO) treatment or placebo based upon the tertile of plasma adiponectin concentration at baseline. Tertile 3 represents IGT subjects with the highest plasma adiponectin concentration.

11
Figure 3—MI of SI and insulin secretion/insulin resistance index in pioglitazone- treated (PIO) and placebo IGT subjects pretreatment (Pre) and posttreatment (Post).
 and placebo IGT subjects pretreatment (Pre) and posttreatment (Post).")
12
Figure 4—Cumulative hazard ratio for the development of diabetes in IGT subjects stratified according to tertile of plasma adiponectin concentration at baseline. All subjects with pretreatment and posttreatment measurements of plasma adiponectin are included in the analysis. Tertile 3 represents IGT subjects with the highest plasma adiponectin concentration.

13
Supplementary Figure 1. Relationship between the change in plasma adiponectin concentration and change in glucose AUC (0-120 min) during the OGTT (left panel) and the change in Matsuda Index of insulin sensitivity (right panel) in IGT subjects treated with pioglitazone. Supplementary Table 1. Relationship between the change in plasma adiponectin concentration and measures of insulin sensitivity, beta cell function and glucose tolerance in PIO-treated subjects.
 during the OGTT (left panel) and the change in Matsuda Index of insulin sensitivity (right panel) in IGT subjects treated with pioglitazone. Supplementary Table 1. Relationship between the change in plasma adiponectin concentration and measures of insulin sensitivity, beta cell function and glucose tolerance in PIO-treated subjects..")
14
RESULTS Pioglitazone reduced IGT conversion to diabetes by 72% in association with improved -cell function by 64% (insulin secretion/insulin resistance index) and increased tissue sensitivity by 88% (Matsuda index). In pioglitazone-treated subjects, plasma adiponectin concentration increased threefold from1360.5 to 386 2.5 mg/mL (P < 0.001) and was strongly correlated with the improvement in SI (r = 0.436, P < 0.001) and modestly correlated with glucose area under the curve during oral glucose tolerance test (r = 0.238, P < 0.005) and insulin secretion/ insulin resistance index (r = 0.306, P < 0.005). The increase in adiponectin was a strong predictor of reversion to normal glucose tolerance and prevention of T2DM. In the placebo group, plasma adiponectin did not change and was not correlated with changes in glucose levels. There was an inverse association between baseline plasma adiponectin concentration and progression to diabetes in the placebo group but not in the pioglitazone group.
 and was strongly correlated with the improvement in SI (r = 0.436, P < 0.001) and modestly correlated with glucose area under the curve during oral glucose tolerance test (r = 0.238, P < 0.005) and insulin secretion/ insulin resistance index (r = 0.306, P < 0.005). The increase in adiponectin was a strong predictor of reversion to normal glucose tolerance and prevention of T2DM. In the placebo group, plasma adiponectin did not change and was not correlated with changes in glucose levels. There was an inverse association between baseline plasma adiponectin concentration and progression to diabetes in the placebo group but not in the pioglitazone group..")
15
CONCLUSIONS Baseline adiponectin does not predict the response to pioglitazone. The increase in plasma adiponectin concentration after pioglitazone therapy in IGT subjects is strongly related to improved glucose tolerance status and enhanced tissue sensitivity to insulin.

16
Message ACTNOW はかなり以前に実施された研究である が、未だにサブ解析で論文が出されている。 Pioglitazone はアディポネクチンを上昇させる。 糖尿病になった症例では介入によるアディポネク チン上昇は低かった。正常耐糖能に戻った症例で はアディポネクチンは高い。最初のアディポネク チン濃度の高低はプラセボでは糖尿病に将来なる かどうかの指標とはなっていたが、 pioglitazone 介入では関係はなかった。

Similar presentations




















: Conversation and Composition 文句 ( もんく ) を言う.>")
