Download presentation
Presentation is loading. Please wait.

1
Testing children for allergies Journal Club 29 th January 2015 Dr Charles Amobi Paediatric Registrar

2
Testing Children for allergies: why,how,who and when An updated statement of the European Academy of Allergy and clinical Immunology (EAACI) Section on Paediatrics and the EAACI-Clemens von Pirquet Foundation. P. A. Eigenmann etal Paediatric Allergy/Immunology 2013:24:195-209

3
Introduction Allergies are common in childhood Cause significant morbidity and Impaired quality of life in children and families Adequate testing is a prerequisite for optimal care

4
This paper provides an evidence based guidance on when and how to test for allergies in children based on common presenting symptoms suggestive of allergic diseases. A persistent, recurrent or severe symptoms suggestive of allergies needs a work up

5
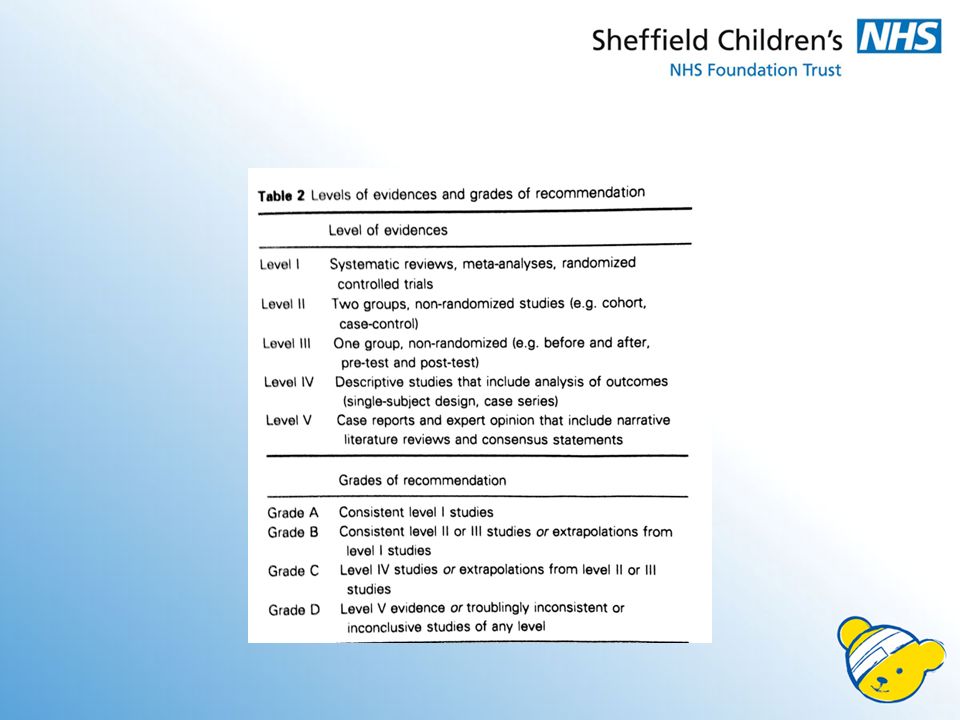
What is allergy? Hypersensitivity reaction to a specific immunogenic trigger initiated by immunologic mechanisms. Its mostly IgE/cell mediated Challenge to physicians is to determine in whom to use diagnostics. Current recommendation is based on published relevant literature

7
Principles Why: In children many common symptoms could be allergy related Who and when: Allergy testing should be initiated according to presenting symptoms and signs. How: Allergy tests should be validated

8
Why allergy testing Allergen avoidance. Logical,allergen-focused avoidance plan to be offered and prevents unwarranted allergen exclusion by negative allergen testing. Food allergies can resolve completely, however strongly positive SPT or elevated spIgE at follow up may predict disease persistence. Monitoring is essential, food e.g. egg and milk can be safely introduced once spIgE levels have fallen sufficiently.

10
Helps with specific allergy treatment This may involve pharmacotherapy and specific allergy immunotherapy Timing may also be crucial e.g. commencing therapy just before the onset of the local grass pollen season can maximize treatment effectiveness for grass pollen-driven allergic rhinitis

11
hide Specific immunotherapy(SIT) has been demonstrated in many studies to be effective treatment for patients with allergic rhino-conjuctivitis and asthma. SIT in childhood pure seasonal allergy results in fewer such children subsequently developing asthma compared to untreated parallel control. SIT may also prevent the onset of new sensitisation

12
Early identification of infants at increased risk for later development of allergic diseases. Children with early development of IgE sensitization to cows milk, hens egg proteins or to inhalant allergens have increased risk for later development asthma. Children with food allergies may be at risk of further allergies,20-25% of children with egg allergy are sensitised to peanut.

14
Practical Allergy testing Focus on hx/examination Type and severity of reaction Identify eliciting allergens and / or other factors Timing between exposure and reaction. Identify related condition Other features include family hx,maternal smoking, mode of delivery and dietary history.

15
Skin Prick Test(SPT) Proper training of tester Allergen panel dependent on age case history Cautious interpretation if <2yrs Variations in devices, techniques and skin reactivity make standardisation difficult. Weal greater or equal to 3mm larger than negative control is accepted as positive.

16
SPT cont’d Standardised extracts are preferable In food allergies using fresh fruits/vegetables avoids labile substances giving negative results. Avoid areas treated with topical steroids. Tests should be at least 4-6 weeks after acute allergic reactions.

17
IgE Tests Total IgE has no indication in specifically diagnosing allergic diseases. In exceptional uses, in inclusion and dose determining parameter for omalizumab therapy. Diagnoses and monitoring parameter in allergic bronchopulmonary aspergillosis As assessment parameter in algorithms to predict reactivity in food challenge Recommendations from level 2/3 evidence papers

18
Allergen specific IgE Assays Should be a validated method Can be performed at any age. Allergens tested should be defined according to symptoms, age and local sensitization patterns. spIgE levels >0.1KU/ml or 0.35 KU/ml considered positive. Inter assay variations may exists.

19
Allergen specific IgE assays cont’d Multiallergen IgE screening measures IgE binding to a panel of allergens in a single test. The have a high negative Predictive Value for atopic diseases SPT and spIgE are complementary They can enhance diagnostic accuracy in some instances Useful in ruling out IgE mediated food allergies They don’t reflect clinical severity.

20
Allergen specific IgE assays cont’d Absolute values appear proportional to the likelihood of clinical allergy For different foods predictive cut off values have been determined. These may differ between studies and populations. Crude allergen extracts that are not standardised can give false positive results. This is due to cross reactive carbohydrate determinants. Component resolved diagnosis(CRD)utilising highly purified or recombinant allergenic components are available in specialist centres
utilising highly purified or recombinant allergenic components are available in specialist centres.")
21
Other tests Basophil activation tests Lymphocyte activation tests. Serum tryptase measurement-highly specific with limited sensitivity. Used in especially food induced reactions. Useful in diagnosis of anaphylaxis with atypical symptoms. Atopy patch testing—useful in eczema and food allergy. May need confirmation with food challenge. Endoscopy.

22
Food Challenges Positive IgE test indicate sensitivity to the food but do not prove allergy unless ingestion of the food has been linked to allergic symptoms. Clinical history has a limited PPV for clinical allergy. Magnitude of test helps to rule in or rule out clinical allergy and helps to plan follow up. Food challenges may be used in both IgE and non IgE mediated food allergies.

23
Food Challenges cont’d Double blind, placebo controlled food challenges remain gold standard especially in research settings. It’s also useful in investigating delayed or non specific symptoms. Challenges must be by trained professionals. Safety is of prime concern Limiting food challenges to setting where appropriate surveillance and emergency care is available

24
Food challenges allow clear diagnosis and decrease unnecessary elimination diets based on positive IgE tests. It is also used in assessing evolution and resolution These derivations are level B evidenced based. Testing for atopic eczema. Atopic eczema is a common skin condition in children. Pathogenesis is related to dry skin, some patients have skin barrier defects mediated by mutation in filaggrin gene.

25
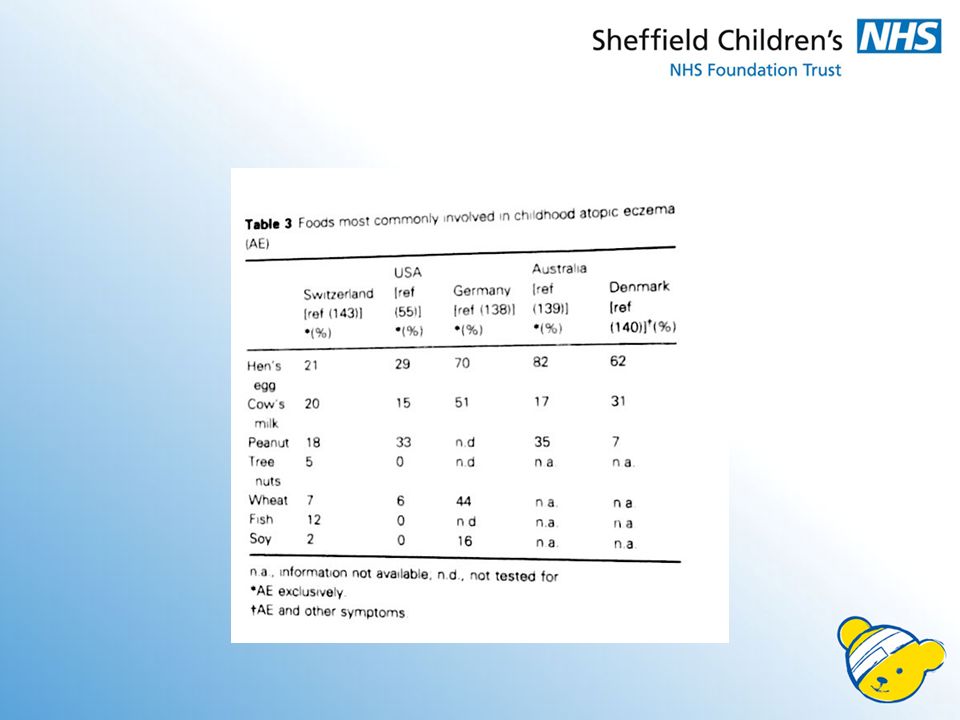
Atopic eczema cont’d Allergens in particular foods in up to 30% of young children may act as triggers. Children with moderate, severe or persistent eczema should have SPT Also children whose disease requires corticosteroids or calcineurin inhibitors. In children greater than three years focus should be on mites, animal danda and pollen as food allergies are less common.

26
Atopic eczema cont’d A negative test has a high NPV Food challenge may be necessary Older children may develop contact dermatitis. This level B evidence guidelines is based on 4 published papers including EAACI position paper on eczematous reaction to food in atopic eczema in 2007

27
Acute Urticaria/Angioedema Both are common presentation of IgE mediated allergy. Other causes include viral infection,drugs,histamine,physical(cold) and vasculitis Angioedema may be hereditary or due to drugs. Allergy tests is indicated when acute urticaria /angioedema occurs within 2 hrs of contact with a possible allergic triggering factor. Allergy related urticaria and angioedema typically lasts up to 24hrs.
 and vasculitis Angioedema may be hereditary or due to drugs. Allergy tests is indicated when acute urticaria /angioedema occurs within 2 hrs of contact with a possible allergic triggering factor. Allergy related urticaria and angioedema typically lasts up to 24hrs..")
28
Acute Urticaria/Angioedema cont’d Type 1 hypersensitivity reaction may be evident e.g. rhinitis,conjuctivitis and wheeze. Lesions lasting more than 24hrs is indicative of viral or drug induced origin. Coexisting signs such as bruising or joint involvement suggests underlying vasculitis. Common causal allergens are egg,milk,peanut and tree nut and other foods.

29
Acute Urticaria/Angioedema cont’d Others are cat, dog and house dust mites Food diary may be informative. Activities and environment features in the last few hours prior to episode may be instructive,. Avoid screening with panel not guided with a clear clinical history. Provocation test may be used to exclude or confirm a particular trigger. Photographs may be helpful.

30
Chronic Urticaria Defined as urticaria present for greater than 6wks Life time prevalence 20% Chronic urticaria is less prevalent than acute urticaria and less common in children compared to adult Its time limited in most children. Related to mast cell degranulation Allergy testing is not indicated Rarely due to hidden or environmental allergy

31
Chronic Urticaria cont’d Avoid SPT. Exclude parasites, autoimmune diseases coeliac disease,C1Inh,drug reaction and mastocytosis. These recommendations(level B evidence) are based on RCPCH care pathway for children with urticaria,angioedema or mastocytosis: an evidence and consensus based national approach and BSACI guidelines for the management of chronic urticarial and angioedema.
 are based on RCPCH care pathway for children with urticaria,angioedema or mastocytosis: an evidence and consensus based national approach and BSACI guidelines for the management of chronic urticarial and angioedema..")
32
Drug induced skin rash Mostly within the first hour,IgE mediated May be non immediate(>1hr),T cell mediated Other features of anaphylaxis— urticaria,angioedema,rhinitis,bronchospasm Maculo papular/mobiliform rash and delayed appearing urticaria/angioedema common with non immediate. Common culprits are antibiotics,Nsaids,anaesthetic agents and antiepileptics

33
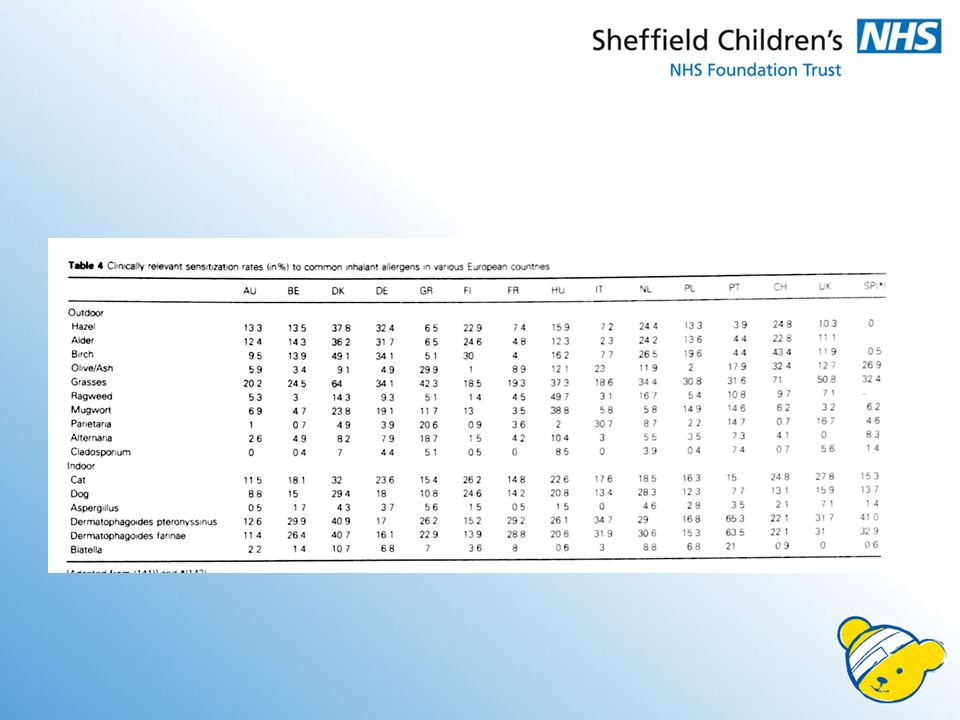
Recurrent rhinitis/conjunctivitis High prevalence in the last 20yrs-more tests Associated snuffling,sneezing,pruritus,congestion, Conjunctivitis with itchy watery eyes. May be seasonal or perennial The former responds well to pharmacotherapy and allergy tests only in resistant cases. The later always needs allergy tests. Allergy to outdoor moulds always seasonal.

34
Cough/recurrent wheeze/Asthma Could be sole or most overwhelming symptom of allergy in child. Allergy tests are warranted in difficult to control cough- persistent or recurrent cough Need to rule out common causes of cough in children. Prevalence of asthma associated atopy is on the increase In these children asthma symptoms ca be triggered by the respective allergens---allergy induced asthma.

35
Cough/recurrent wheeze/Asthma cont’d Allergy tests help in supporting the diagnosis, informing prognosis,phenotyping and indicating avoidable disease triggers Children with recurrent wheeze(> 3 per year) not triggered by upper airway infection, chronic wheeze should be tested for IgE sensitization. Increasing age, positive family history and presence of additional allergic symptoms makes allergy testing increasingly desirable.

36
Diagnosis of asthma is based on history, lung function tests, evaluation of bronchial hyper responsiveness and well designed therapeutic trial SPT/spIgE may be used Age/regional consideration in selection of allergens. Early in life +ve IgE tests do not necessarily imply disease triggering.

37
Gastrointestinal symptoms This could be IgE mediated,IgE associated/cell mediated pathologies, cell mediated pathologies. IgE mediated GI symptoms are mostly associated with other symptoms, frequently within the context of anaphylactic reaction. Common non IgE mediated GI symptoms of allergy include abdominal pain, vomiting,diarrhea,gastroesophageal reflux, poor weight gain, irritability and poor sleep.

38
Gastrointestinal symptoms cont’d These are associated with specific syndromes e.g. eosinophilic oesophagitis and food protein induced enterocolitis syndrome(FPIES) Diarrhoea and vomiting as a result of allergy should be a diagnosis of exclusion Exclusion/re-exposure diet with resolution and recurrence of symptoms identifies the trigger. Endoscopy may be needed
 Diarrhoea and vomiting as a result of allergy should be a diagnosis of exclusion Exclusion/re-exposure diet with resolution and recurrence of symptoms identifies the trigger. Endoscopy may be needed.")
39
Colic 5-10% incidence in children,3h/day,>3days/wk,>3wks Crying as a result of allergy is a diagnosis of exclusion Indication for allergy tests is in context of other existing allergy symptoms –skin,GIT or airway. Or if symptom is recurrent with ingestion of specific foods Cows milk protein allergy could present with colic in 30- 40% of cases. Elimination and challenge confirms the diagnosis in exclusively breastfed babies.

40
Insect stings Children with systemic reaction are at risk of further severe reaction and will need allergy testing SIT is the only treatment option. Large local reaction is not an indication Allergy testing assess venom specific IgE sensitization SPT or spIgE is commonly used. Size of weal or flare not indicative of severity of systemic reaction Tests like serum tryptase rules out mastocytosis The later may cause increased reaction or treatment failure.

41
All siblings of an index case who have symptoms should be offered allergy testing. Sibling of food allergenic children should also be considered for testing. Most relevant allergenic foods should be tested. Foods with negative IgE tests can be introduced at home and those with positive IgE tests should be introduced in formal challenge tests in appropriate setting.

42
Conclusion Allergy tests should be interpreted bearing in mind the limitations. Test results may be age and total serum IgE- dependent Further studies needed to investigate relationship between IgE and disease activity. In trained hands allergy tests can provide a definite answer, thus reducing unnecessary avoidance of food and medication.

43
Thank you

Similar presentations









 Royal Liverpool and Broadgreen University Hospitals NHS Trust, Liverpool, United Kingdom.>")

 type I.>")
 Institute of Pediatry, Obstetrics and Gynaecology, Kiev, Ukraine 2) Royal Liverpool and Broadgreen.>")

 Diagnosis and management of chronic asthma in line with current BTS guidelines (Dr Lowery) 3 x Case.>")




