Download presentation
Presentation is loading. Please wait.

1
Urethral Strictures Causes Diagnosis Assessment Treatment options Prognosis

2
References

3
Curriculum Knowledge of the pelvis, male genitalia and urethra including embryology of urethra including hypospadias and epispadias Neuroanatomy as it relates to normal and abnormal bladder, urethral and pelvic floor function Causes, pathophysiology and complications of urethral strictures Pathophysiology of traumatic urethral injury Assessment of patient with urethral stricture Ability to determine appropriate surgical option for patients with urethral stricture Be able to advise on the surgical options and the appropriateness of surgery Knowledge of endourological techniques relevant to urethral stricture Techniques and complications of urethral reconstruction Management of postoperative consequences of urethral reconstruction Arrange appropriate follow up of patients with urethral reconstruction Liaison with other specialties e.g. radiology, orthopaedics, GI surgeons

4
Definitions The term urethral stricture refers: to anterior urethral disease is a scarring process that involves the epithelium as well as the spongy erectile tissue of the corpus spongiosum. Con- traction of the scar reduces the urethral lumen. In contrast, posterior urethral strictures are more correctly referred to as pelvic fracture urethral injuries; strictures of the prostatic urethra or bladder neck are properly referred to as contrac- tures or stenoses. Chapple et al, BJUI 2004

5
Anatomy

6
Blood supply

7
Neuroanatomy

8
Neuroanatomy of the male urethra and perineum, BJUI 2003

9
Distribution Anterior – 92.2% Posterior – 7.8% Palminteri et al. Contemporary urethral stricture characteristics in the developed world. Urology 2013

10
Aetiology Unknown41.3 Failed hypospadias repair17.0 Catheter9.9 Instrumentation6.2 Radiotherapy0.6 TURP1.3 Trauma15.8 LS6.9 Infection0.8 Congenital0.2 Stein et al. A geographic analysis of male urethral stricture aetiology and location. BJUI, 2013

11
Aetiology Stein et al. A geographic analysis of male urethral stricture aetiology and location. BJUI, 2013

12
Pathology Noxious stimulus (bacterial, chemical, physical) Denuded epithelium Squamous metaplasia Fissures develop in epithelium Urine extravasation Fibrosis develops in the corpus spongiosum Fibrotic plaques coalesce StrictureMundy et al. Urethral strictures, BJUI 2010

13
Pathology of anterior stricture Campbell’s Urology, 2011

14
Pathology of contractures/stenoses Shearing forces transmitted through the perineal membrane and pubo-prostatic ligament Distraction-avulsion most commonly at bulbo- membranous junction Transection by the bony fragments – rare Partial or complete ruptures Fibrosis interposed between the distracted ends

15
Case 1 40 Male 6/12 h/o flow problem presenting at your clinic....

16
Presentation Obstructive LUTS: poor stream, incomplete bladder emptying, hesitancy, dribbling Urinary tract infections Acute urinary retention Haematuria Asymptomatic

17
Investigations The aim is to determine: location, length, depth and density of the stricture/spongiofibrosis. Campbell’s Urology. 2011

18
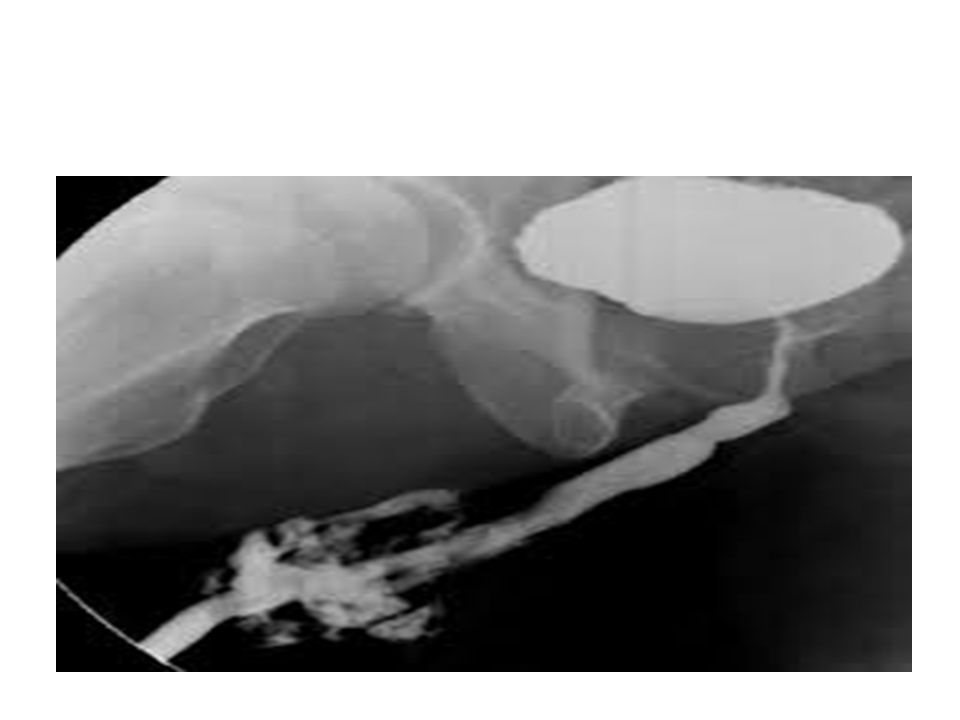
Investigations Flow studies Flexible endoscopy – urethral – suprapubic – Does not show length, proximal urethra Radiology – Contrast studies- retrograde urethrogram, voiding cystogram. – USS useful for bulbar strictures? limited

19
Case 1 Flow studies: Flexible cystoscopy: At 12 cm

20
Urethrogram? ‘there are many urologists who think that a urethrogram is not necessary before deciding upon treatment, mainly because they are going to do a urethrotomy anyway. This is not the authors’ view. Urethrography gives a more complete assessment.’ Mundy et al. Urethral strictures. BJUI 2010

21
Treatment Management Cure Both the patient and the physician must have a good understanding of the goal of treatment before the treatment choice is made. To this end, treatment options should be discussed with the patient, with care taken to emphasize the anticipated outcome with regard to potential cure. Campbell’s Urology, 2011

22
Treatment ‘In the absence of complications, treatment is for symptoms and if the symptoms are not particularly troublesome, treatment is symptoms are not troublesome, treatment is unnecessary’ Mundy et al. Urethral strictures. BJUI 2010

23
Treatment Reconstructive ladder – archaic Dilatation: – oldest/simplest – epithelial stricture without spongiofibrosis – stretch the scar, avoid bleeding – Results equal to optical urethrotomy

24
Treatment Mundy et al. Urethral strictures. BJUI 2010

25
Treatment - Optical urethrotomy -Where to cut? Thinnest portion of corpus spongiosum at 12 o’clock at bulb. Easy to penetrate the corpus cavernosum -Radial cuts better? -If wound contraction occurs before re-epithelisation then the stricture recurs. -Post-op catheter 3 days Desmond et al. Critical evaluation of direct vision urethrotomy by urine flow measurement. Br J Urol 1981 TONKIN et al. Management of distal anterior urethral strictures. Nat Rev Urol. 2009

26
Treatment - Optical urethrotomy Adjuvant modalities to reduce the rate of stricture recurrence include the following: Intermittent self-catheterisation Steroids injected at the site of IU Anti-inflammatory medication by mouth Mitomycin-C injected transurethrally Brachytherapy using an intraurethral balloon filled with radio-active isotope Captopril gel intra-urethrally Heyns. Urethral stricture: should we stop urethrotomies? EAU 2011

27
Treatment - Optical urethrotomy -Complications: 1. urine extravasation 2. pain 3. UTI 4. ED 1 1. McDermott et al. Erectile impotence as complication of direct vision cold knife urethrotomy. Urology 1981

28
Recurrence post optical urethrotomy ? always?

29
Recurrence post optical urethrotomy – factors Length of the stricture (longer than 2 cm) Extent of spongiofibrosis on ultrasound (or stricture diameter on retrograde urethrography) Previous procedures (UD, IU, UP) Shorter time to stricture recurrence after IU or UD Longer duration of follow-up (although most strictures that recur, do so within 12 months) Heyns. Urethral stricture: should we stop urethrotomies? EAU 2011

30
Case 1 continued 4/12 post urethrotomy pt is back in the clinic saying symptoms re-occurred...

32
Treatment Management Cure Both the patient and the physician must have a good understanding of the goal of treatment before the treatment choice is made. To this end, treatment options should be discussed with the patient, with care taken to emphasize the anticipated outcome with regard to potential cure. Campbell’s Urology, 2011

33
Case 1 continued Options: – 1. Repeat urethrotomy, UD, Laser, Stent Rate of success v. low (6%) 1 – 2. Open surgery (urethroplasty) Rate of success depending on the pathological features of the stricture. 1. Santucci et al. Urethrotomy has a much lower success rate than previously reported. J Urol 2010
 1 – 2. Open surgery (urethroplasty) Rate of success depending on the pathological features of the stricture. 1. Santucci et al. Urethrotomy has a much lower success rate than previously reported. J Urol")
34
Treatment Laser – no evidence – Ideal laser should totally vaporise tissue cause negligible peripheral tissue destruction not absorbed by water suitable fibre – Carbon dioxide ideal, needs gas cystoscope, CO2 embolus – Argon/Nd:Yag causes thermal necrosis can injure peripheral tissues – Holmium YAG

35
Treatment - Stents – Wallstent or UroLume® (Pfizer Inc., UK) which is incorporated into the urethral wall – Memokath® (Engineers & Doctors A/S Ltd., Hornbaek, Denmark) which is not. Results are v. poor- De Vocht et al BJU 2003. Makes reconstruction more difficult.

36
UroLume®

37
Memokath®

38
Repeat urethrotomy 1. A second DVIU/dilation can be indicated for recurrent urethral strictures with favourable characteristics ( 3 months after previous treatment (B). 2. A third DVIU/dilation is not recommended, except if necessitated by patient comorbidities or economic resources (A). 3. Urethral reconstruction over repeat DVIU/dilation should be offered for urethral strictures that recur within 6 months or are refractory to a second DVIU/dilation (A). Heyns et al. SIU/ICUD Consultation on Urethral Strictures: Dilation, Internal Urethrotomy, and Stenting of Male Anterior Urethral Strictures. Urology 2014
. 2. A third DVIU/dilation is not recommended, except if necessitated by patient comorbidities or economic resources (A). 3. Urethral reconstruction over repeat DVIU/dilation should be offered for urethral strictures that recur within 6 months or are refractory to a second DVIU/dilation (A). Heyns et al. SIU/ICUD Consultation on Urethral Strictures: Dilation, Internal Urethrotomy, and Stenting of Male Anterior Urethral Strictures. Urology")
39
Repeat urethrotomy Issue the cost effectiveness of a repeat DVIU vs urethroplasty Greenwell et al. Repeat urethrotomy and dilatation for the treatment of urethral stricture are neither clinically effective not cost effective. J Urol 2004 Rourke et al. Primary urethral reconstruction: the cost minimised approach to the bulbous urethral stricture. J Urol 2005

40
Open Trial in UK Randomised, multicentre trial of open urethroplasty versus endoscopic urethrotomy For men who have got 1 st recurrence of stricture

41
Case 1 continued Pt opts for open surgery...

42
Treatment Bulbar urethroplasty Penile urethroplasty Posterior urethral reconstruction

43
Bulbar urethroplasty Anastomotic or substitution? Ventral or dorsal graft location? One stage or two stage repair? Barbagli. EAU 2008

44
Treatment – anastomotic urethroplasty Indications – < 2cm- historically – bulbar urethra – relies on mobilisation of corpus spongiosum Best results – excise stricture – spatulated anastomosis – overlaping ends Outcomes – long term success over 90 – 95% 1-2 1. R.A. Santucci et al. Anastomotic urethroplasty for bulbar urethral stricture: analysis of 168 patients. J Urol. 2002 2. G. Barbagli et al. One-stage bulbar urethroplasty: retrospective analysis of the results in 375 patients. Eur Urol. 2008

45
Treatment – anastomotic urethroplasty

46
Complications Ejaculatory dysfunction 20% Decreasedd glans sensitivity 18% Poor glans erection 11% Cold glans 1.6% Barbagli. EAU 2008

47
Augmented anastomosis with graft onlay

48
Grafts/Flaps Graft ‘tissue excised from a donor site which re-establishes its blood supply by revascularisation’ Process by which revascularisation occurs = ‘take’ Take = 3 to 4 days 2 processes – imbibition and inosculation

49
Imbibition 48 hours Graft survives by ‘drinking’ nutrients from host bed Graft temperature lower than host temperature

50
Inosculation 48 hours Development of true circulation Graft temperature rises to that of host Features affecting ‘take’: -Graft type -Donor site vascularity (tendon, smoking) -Infection -Movement
 -Infection -Movement")
51
Grafts examples Skin (full thickness, split thickness) Buccal mucosa Bladder mucosa Rectal mucosa
 Buccal mucosa Bladder mucosa Rectal mucosa")
52
Skin vs Buccal mucosa Cornified layer Epidermis Papillary dermis Reticular dermis Oral epithelium Superficial lamina (submucosa) Deep lamina (submucosa) Muscle and minor salivary glands
 Deep lamina (submucosa) Muscle and minor salivary glands")
53
Buccal Mucosa Graft Easy to harvest Easy to handle Thick Panlaminar vascular plexus – good take Waterproof Antibacterial Resists skin diseases

54
Harvesting buccal mucosa Normal intubation OK vs. nasal intubation Avoid Stensen’s duct opposite second upper molar Mark excision site 0.5% lignocaine and adrenaline Tenotomy scissors (superficial vs. deep) 2cm wide, at least 1cm from vermillion border Side effects worse for closure vs. secondary intention Lignocaine lozenges
 2cm wide, at least 1cm from vermillion border Side effects worse for closure vs. secondary intention Lignocaine lozenges.")
56
Flaps Penile/preputial Based on Dartos Useful when infection or extensive fibrosos present Transverse, Longitudinal, Circumferencial

59
Onlay urethroplasty methods

60
Augmented urethroplasty Barbagli dorsal onlay BMG

61
Bulbar urethroplasty - outcomes Ventral OMG – 90% Lateral OMG – 83% Dorsal OMG - 77 Barbagli. EAU 2008

63
Penile urethroplasty One stage or two stage repair? Flap or graft urethroplasty? Barbagli. EAU 2008

65
Penile urethroplasty

66
Special circumstances BXO – avoid skin flaps/grafts as it is a skin condition – buccal mucosa is better

67
Special circumstances Options – Dilatation – Holmium laser stricturotomy – Urethrotomy (avoid 6 o’clock) – Urethrotomy + AMS sphincter – Open reconstruction – Urinary diversion
 – Urethrotomy + AMS sphincter – Open reconstruction – Urinary diversion")
68
Post TURP stricture Tend to be at bladder neck (incise) More difficult at membranous urethra since incision here will compromise continence as bladder neck mechanism lost Gentle ISD Anastomotic urethroplasty + sphincter (problems with erosion) Multistage scrotal flap technique
 More difficult at membranous urethra since incision here will compromise continence as bladder neck mechanism lost Gentle ISD Anastomotic urethroplasty + sphincter (problems with erosion) Multistage scrotal flap technique")
69
Thank you

Similar presentations








,>")















