Download presentation
Presentation is loading. Please wait.

1
Lymphoscintigraphy and SNLB in
DSNMC

2
Background The seven-point checklist of a pre-existing pigmented lesion: Major features: Change in size Irregular shape Irregular colour Minor features Largest D≥7mm Inflammation Oozing Change is sensation

3
Background Biopsy of a suspected lesion
A full-thickness skin biopsy to include the whole tumor a 2-5 mm clinical margin of normal skin laterally a cuff of subdermal fat

4
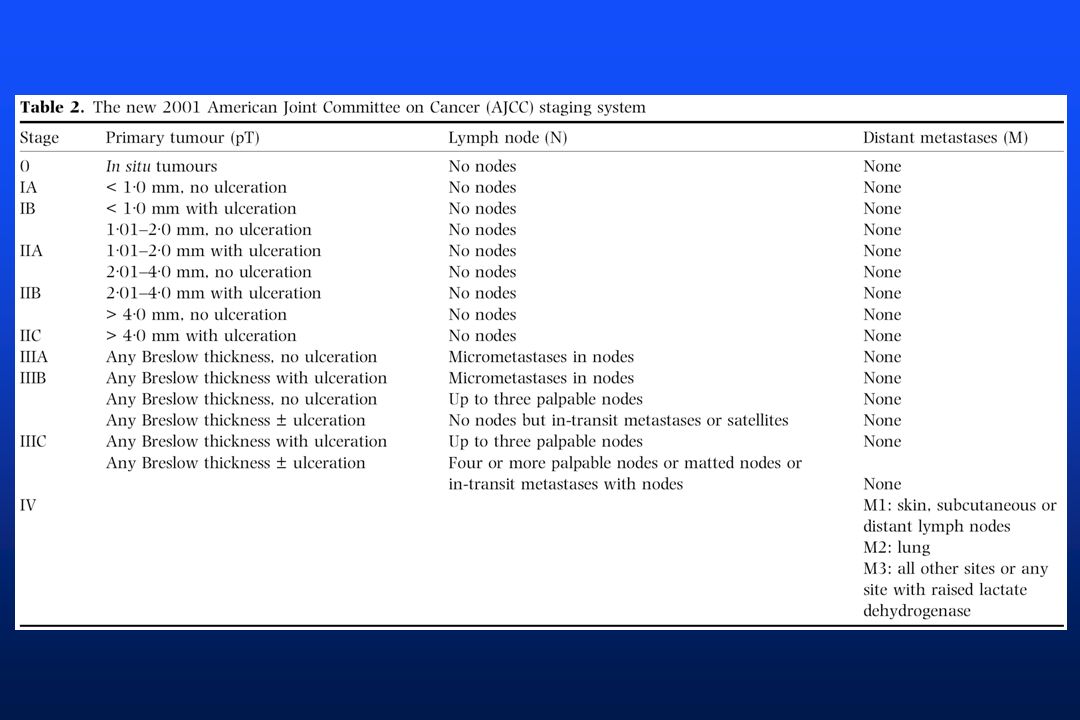
Background The Breslow thickness:
Measured from the granular layer of the epidermis to the base of the tumor, to the nearest 0.1 mm. Clark’s level: The depth of penetration of dermis

6
TREATMENT Surgical excision for primary lesion: margins based on Breslow thickness Adjuvant therapy: No proven benefit Interferon Intermediate or high risk of relapse Stage IIB, IIC, III Lymph node dissection

7
TREATMENT Metastatic disease: Surgical removal of localized metastases
Skin, Solitary brain mets, … Radiotherapy to bone or skins mets: Short-term symptomatic control Palliative value in brain mets Unresectable mets Standard chemotherapy No remarkable benefit in survival

8
Definitions Sentinel lymph node: The first lymph node in a lymph node bed to receive lymphatic drainage from a tumor. Often drainage to more than 1 lymph node group and sentinel node is identified. Lymphoscintigraphy: Imaging pathways of lymphatic flow and lymph nodes Gamma-detecting intraoperative probe: Small, hand-held radiation-detecting device Blue dye technique: Intraoperative injection (usually peritumoral) of isosulfan blue dye for the purpose of staining lymphatic vessels and sentinel lymph nodes
 of isosulfan blue dye for the purpose of staining lymphatic vessels and sentinel lymph nodes.")
9
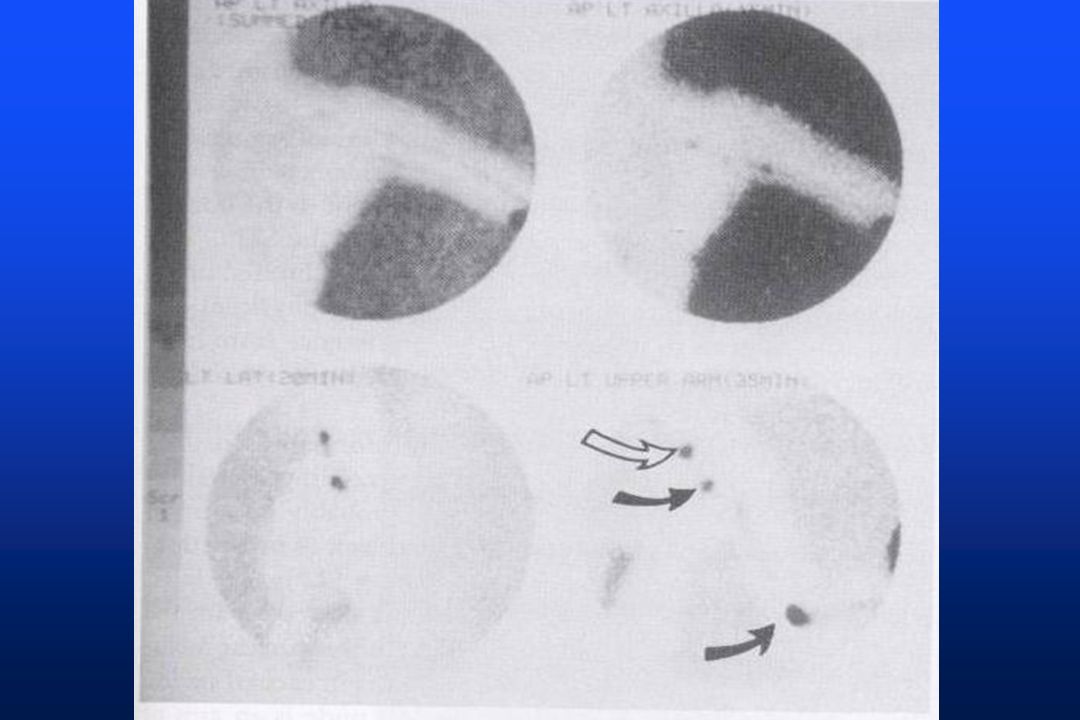
Technique Dynamic and Static Imaging with Gamma camera.
0.1mL : 100 μCi: filtered Tc-99m SC 4–8 peritumoral intradermal injections Within 1 cm from the melanoma An exception: head or neck, Injections inferior to those lesions Dynamic and Static Imaging with Gamma camera.

12
In-transit nodes: For extremity lesions, the knee or elbow regions in the field of view to detect in-transit (intercalated) LNs : SLNs
 LNs : SLNs.")
15
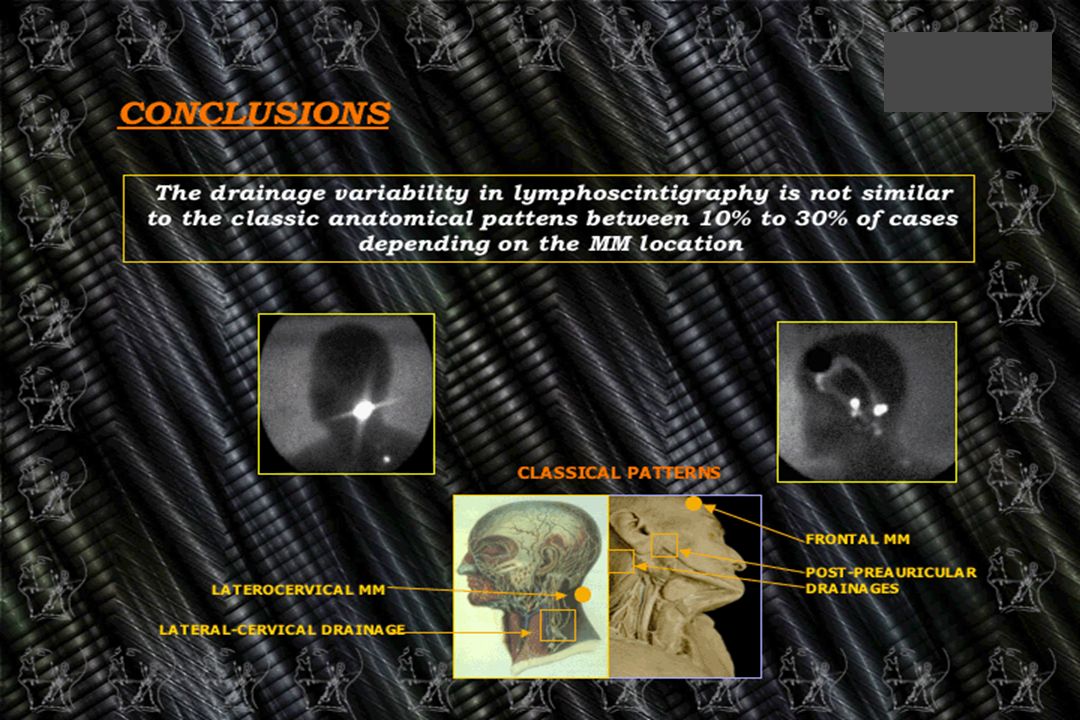
Melanoma In more than 10% of melanoma, lymphatic drainage goes to 2 or 3 node groups Sometimes lymphatic drainage is unpredictable

18
The Evolution of the Management of Regional LNs in MM
In The past ELND :of the lymphatic bed believed most likely to drain the primary tumor site (based on Sappey’s classic anatomic description of cutaneous lymphatic flow) was used as part of the staging procedure for melanoma. ELND has been a controversial staging procedure for patients with intermediate (I and II) stage melanoma, Approximately 80% have tumor-negative lymph nodes Do not need ELND No benefit Associated with significant morbidity and cost. Newer methods of managing regional LNs : SLN
 was used as part of the staging procedure for melanoma. ELND has been a controversial staging procedure for patients with intermediate (I and II) stage melanoma, Approximately 80% have tumor-negative lymph nodes. Do not need ELND. No benefit. Associated with significant morbidity and cost. Newer methods of managing regional LNs : SLN.")
19
Controversy about ELND
Multiple Trials: No significant difference in survival between ? * WHO melanoma group: Trunk MM at least 1.5 mm in thickness, After wide excision of the tumor, patients were randomized to receive either ELND or Observation (underwent lymphadenectomy if they subsequently developed clinical evidence of nodal metastasis) There was no difference in survival between the ‘‘delayed’’ and the immediate nodal dissection Others have documented no survival benefit for patients treated with ELND versus nodal observation The lack of benefit for ELND may be due, in part, to the relatively low percentage of patients with nodal metastases at the time of diagnosis. About 20% of patients with intermediate thickness or thick melanomas are expected to harbor nodal metastasis These studies formed the framework for nodal management for several decades, leading to the era of the SLN concept. *Lancet 1998;351:
 There was no difference in survival between the ‘‘delayed’’ and the immediate nodal dissection. Others have documented no survival benefit for patients treated with ELND versus nodal observation. The lack of benefit for ELND may be due, in part, to. the relatively low percentage of patients with nodal metastases at the time of diagnosis. About 20% of patients with intermediate thickness or thick melanomas are expected to harbor nodal metastasis. These studies formed the framework for nodal management for several decades, leading to the era of the SLN concept. *Lancet 1998;351:")
20
Sentinel Lymph Node Excisional Biopsy
SLNB Simple Not significant morbidity Accurate information about lymphatic drainage patterns Allows the surgeon to make a smaller incision directly over the node based on the image and probe counts. Demonstrate the unpredictability of lymphatic drainage patterns. More accurate histopathological and molecular analysis and detection of micrometastasis as compared to the large number of LNs in ELND

21
SLNB * 612 patients with early stage melanoma who underwent lymphatic mapping and SLN biopsy They were able to identify a SLN in 95% of the patients, found that 15% of SLN contained evidence of metastasis SLN status was the most significant prognostic factor influencing survival Further refinements in mapping techniques have improved the ability to detect the SLN. * * One such method involves the use of both Tc99-labeled sulfur colloid and isosulfan blue dye mapping technique allows for correct identification and biopsy of the SLN in 99% of patients *J Clin Oncology 1999; 17: * *Surgery 1998;124:

22
SLNB is a safe, accurate procedure with low morbidity
5-year disease-free survival rate of 78.3%(SLNB) vs 73.1%(Observe) (P=0.009) 5-year survival rate was higher for the patients who underwent completion lymphadenectomy for a positive SLN compared to the observed patients who underwent nodal dissection at the time of nodal recurrence (72.3% vs. 52.4%, respectively, P=.004) Validate the SLN approach: early nodal evaluation provides valuable prognostic information and permits both accurate nodal basin staging and early lymphadenectomy. The status of SLN : single most accurate prognostic indicator of metastatic disease *Ann Surg 2005;242: * *N Engl J Med 2006;355:
 vs 73.1%(Observe) (P=0.009) 5-year survival rate was higher for the patients who underwent completion lymphadenectomy for a positive SLN compared to the observed patients who underwent nodal dissection at the time of nodal recurrence (72.3% vs. 52.4%, respectively, P=.004) Validate the SLN approach: early nodal evaluation provides valuable prognostic information and permits both accurate nodal basin staging and early lymphadenectomy. The status of SLN : single most accurate prognostic indicator of metastatic disease. *Ann Surg 2005;242: * *N Engl J Med 2006;355:")
23
Common Indications Sentinel node localization and excision using radionuclide methods are performed in the care of patients with Intermediate stage primary melanoma (Breslow 0.76 mm–4.0 mm). No clinical evidence of nodal involvement. No clinical evidence of distant tumor spread. Exclusions may include patients with: 1. Extensive previous surgery in the region of the primary tumor site or targeted lymph node bed. 2. Patients with known metastases.
. No clinical evidence of nodal involvement. No clinical evidence of distant tumor spread. Exclusions may include patients with: 1. Extensive previous surgery in the region of the primary tumor site or targeted lymph node bed. 2. Patients with known metastases.")
24
SLNB approach Guideline: entails removing all
Blue stained lymph nodes, All palpable lymph nodes nodes greater than 10% of the radioactivity of the hottest node By following these recommendations, it is unlikely that the SLN will be missed. *Sunbelt Melanoma Trial. J Surg Oncol 2004; 86:

25
SLNB approach Now that we can identify patients with occult nodal metastasis with a minimally invasive test The next great challenge is to develop more effective and less toxic adjuvant therapy options.

26
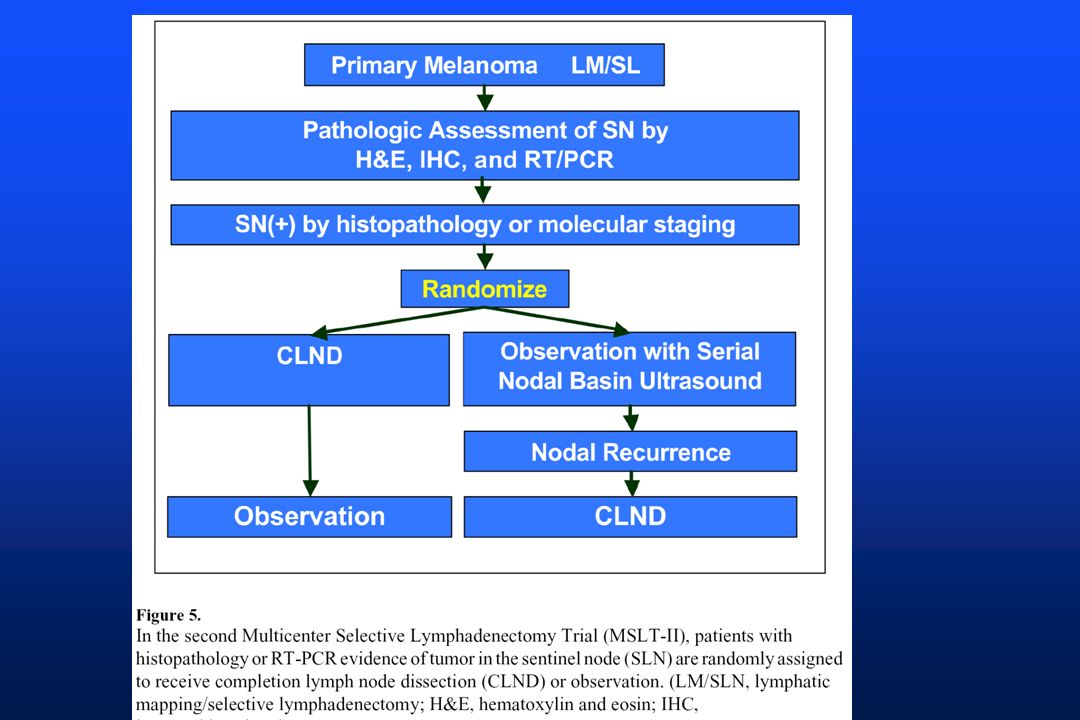
If SLN was + Need for lymph node dissection for positive SLNs?
16% of patients treated with completion lymphadenectomy following a positive SLN biopsy will harbor metastatic disease in the non-SLN Which patients with a positive SLN may safely avoid completion LND.

29
در مرکز پزشکی هسته ای دکتر دباغ – دکتر صادقی
در خدمت شما هستیم V.R.Dabbagh; DSNMC;

Similar presentations