Download presentation
Presentation is loading. Please wait.

1
Approach to Patient with
Chest Pain MPRPC Group 1 Section C

2
General Data Name: E.R. Age/Sex: 53/F Status: Married
Address: 608 Lacson Ave, Sampaloc, Manila Race: Filipino Religion: Roman Catholic Occupation: Housewife Date of Admission: Nov. 17, 2009

3
HISTORY OF PRESENT ILLNESS
2 years PTA Incidentally diagnosed as hypertensive (150/90) Given nifedipine (Calcibloc) not compliant, taken as needed Experienced headache Sought consult at Ospital ng Maynila 3 months PTA
 Given nifedipine (Calcibloc) not compliant, taken as needed. Experienced headache. Sought consult at Ospital ng Maynila. 3 months PTA.")
4
HISTORY OF PRESENT ILLNESS
Experienced first episode of chest pain and heaviness characterized by sharp pain at sternal area, non-radiating and lasting for 10 minutes. (precipitating factor; grade?) Weakness (type?) of both upper extremities but relieved by herbal oil massage Jose Reyes Memorial Hosp. BP 160/90 2 months PTA Experienced body ache (type?) precipitated by stress 1 day PTA
 Weakness (type ) of both upper extremities but relieved by herbal oil massage. Jose Reyes Memorial Hosp. BP 160/90. 2 months PTA. Experienced body ache (type ) precipitated by stress. 1 day PTA.")
5
HISTORY OF PRESENT ILLNESS
A few minutes after waking up, experienced gradual chest tightness and heaviness (describe) USTH ER Chief complain: chest pain BP 200/110 IV nicardipine Oxygen Sublingual nitroglycerin ECG & chest X-ray 5 hours PTA Admission
 USTH ER. Chief complain: chest pain. BP 200/110. IV nicardipine. Oxygen. Sublingual nitroglycerin. ECG & chest X-ray. 5 hours PTA. Admission.")
6
Past Medical History (+) cataract, OD (2008) (+) cataract, OS (2004)
(-) previous hospitalizations (-) DM, heart disease, PTB, asthma, cancer, allergies Unrecalled immunizations
 previous hospitalizations. (-) DM, heart disease, PTB, asthma, cancer, allergies. Unrecalled immunizations.")
7
Family History Father – HPN, colon cancer, Mother - DM
died 63 y/o due to CVA Mother - DM died 62 y/o due to CVA All siblings – HPN, DM (-) TB, asthma, allergies
 TB, asthma, allergies.")
8
Personal and Social History
Preference to sweet and salty foods (-) smoking history (+) exposure to second hand smoke (34 years) (-) alcohol consumption Denies illicit drug use
 smoking history. (+) exposure to second hand smoke (34 years) (-) alcohol consumption. Denies illicit drug use.")
9
Review of Systems General: no significant weight loss; no anorexia; no headache Skin: no itchiness HEENT: blurring of vision L>R; no tinnitus; no aural discharge Thorax: no breast pain Pulmonary: no respiratory distress; no dyspnea; no PND; no orthopnea

10
Review of Systems GIT: no abdominal pain; no diarrhea & vomitting
GUT: no difficulty in urination Endocrine: no polydipsia, polyphagia, polyuria; no heat and cold intolerance MS: No joint pain; no muscle pains; no weakness Neurological: No dizziness

11
Physical Examination On admission (Nov. 17, 2009)
Upon PE (Nov. 18, 2009) General Survey Conscious, coherent, stretcher-borne, in cardiorespiratory distress Vital Signs BP: 200/100, supine LUE; 190/100, RUE, SBP 190, LLE, SBP 190 RLE; PR: 88, regular; HR:88, regular; RR:24; T 36.5 Conscious coherent, ambulatory, not in cardiorespiratory distress BP: 110/70; PR: 76, regular; HR: 76, regular; RR: 20, regular; T 36.0 Anthropometric Measurements: Height: 157cm Weight: 74kg BMI: 30
 General Survey. Conscious, coherent, stretcher-borne, in cardiorespiratory distress. Vital Signs. BP: 200/100, supine LUE; 190/100, RUE, SBP 190, LLE, SBP 190 RLE; PR: 88, regular; HR:88, regular; RR:24; T Conscious coherent, ambulatory, not in cardiorespiratory distress. BP: 110/70; PR: 76, regular; HR: 76, regular; RR: 20, regular; T Anthropometric Measurements: Height: 157cm Weight: 74kg BMI: 30.")
12
Physical Examination On admission Upon PE Skin HEENT
Warm, moist skin, no flushing, no active dermatoses HEENT Pink palpebral conjunctivae, anicteric sclera, (+) ROR, hazy cornea No nasoaural discharge, septum midline, moist buccal mucosa No tragal tenderness AU, non-hyperemic external auditory canal AU, intact tympanic membrane AU Warm, moist skin, no flushing, no active dermatoses Pink palpebral conjunctivae, anicteric sclerae, (+) ROR no nasal or aural discharge, no nasal deformities, midline septum Intact tympanic membrane, no tragal tenderness
 ROR, hazy cornea. No nasoaural discharge, septum midline, moist buccal mucosa. No tragal tenderness AU, non-hyperemic external auditory canal AU, intact tympanic membrane AU. Warm, moist skin, no flushing, no active dermatoses. Pink palpebral conjunctivae, anicteric sclerae, (+) ROR. no nasal or aural discharge, no nasal deformities, midline septum. Intact tympanic membrane, no tragal tenderness.")
13
Physical Examination On admission Upon PE HEENT
Moist buccal mucosa, tongue midline, non-hyperemic PPW, tonsil not enlarged no limitation in motion, Trachea midline, thyroid gland not enlarged, neck veins not distended, no cervical lymphadenopathy, (-) carotid bruits Moist buccal mucosa, no oral ulcers supple neck, thyroid gland not enlarged, no palpable cervical lymphadenopathy, trachea midline, neck veins not distended
 carotid bruits. Moist buccal mucosa, no oral ulcers. supple neck, thyroid gland not enlarged, no palpable cervical lymphadenopathy, trachea midline, neck veins not distended.")
14
Physical Examination On admission Upon PE Cardiovascular
Adynamic precordium, JVP 3cm at 30 degree, AB at 5th LICS 11cm from the midsternal line, tapung, 2cm in diameter, no heaves, no thrills, no lifts S1>S2 apex, S2>S1 base, no murmurs Pulses full and equal, no edema, no cyanosis, no clubbing Adynamic precordium, apex beat at 5th LICS 11cm from the midsternal line, no heaves trills lifts, apex S1>S2, base S2>S1, no murmurs, JVP 4cm at 30 degrees No edema, pulses full and equal on all extremities

15
Cardiac Auscultogram CAP rapid upstroke gradual down stroke
JVP 3 cm at 30° A P T M S1 S2 S1 S2 S1 S2 S1 S2 Precordial Activity: Adynamic precordium No heaves, lifts, or thrills Apex beat: 5th LICS 11 cm from midsternal line

16
Physical Examination On admission Upon PE Pulmonary
Symmetrical chest expansion, no retractions, no lagging, equal tactile and vocal fremiti, resonant on percussion, clear breath sounds No chest retractions, no use of accessory muscles, normal breathing pattern, symmetrical chest expansion, unimpaired transmission of voice and tactile fremiti, resonant on both sides, vesicular breath sounds on both sides

17
Physical Examination On admission Upon PE Gastrointestinal
Flabby abdomen, no striaes, no visible peristalsis, NABS, (-) bruits, tympanitic on percussion, no tenderness, liver edge not palpable, Traube’s space not obliterated Flabby abdomen, normoactive bowel sounds, tympanitic, non-tender, liver dullness 10 cm, Traube’s space not obliterated
 bruits, tympanitic on percussion, no tenderness, liver edge not palpable, Traube’s space not obliterated. Flabby abdomen, normoactive bowel sounds, tympanitic, non-tender, liver dullness 10 cm, Traube’s space not obliterated.")
18
Physical Examination On admission Upon PE Neurologic
Awake, alert, conscious, oriented to 3 spheres CN: no anosmia, pupils 2-3mm ERTL, EOMs intact, V1V2V3 intact and equal, can clench teeth, can smile, can frown, intact hearing, (+) gag reflex, can raise both shoulders against resistance, uvula midline on phonation, can shrug shoulders, tongue midline on protrusion Conscious, awake, oriented to person, place and time, can follow commands Cranial nerves intact, pupils equally responsive to light, extraocular muscles intact, no facial asymmetry, can smile, frown, clench teeth, puff cheeks, normal gross hearing, uvula midline, (+) gag reflex, able to shrug shoulders, turn face against resistance
 gag reflex, can raise both shoulders against resistance, uvula midline on phonation, can shrug shoulders, tongue midline on protrusion. Conscious, awake, oriented to person, place and time, can follow commands. Cranial nerves intact, pupils equally responsive to light, extraocular muscles intact, no facial asymmetry, can smile, frown, clench teeth, puff cheeks, normal gross hearing, uvula midline, (+) gag reflex, able to shrug shoulders, turn face against resistance.")
19
Physical Examination On admission Upon PE Neurologic
Motor: 5/5 on the lower extremities, 5/5 on the upper extremities, no fasciculations, atrophy No babinski, bilateral No sensory deficit No nuchal rigidity, Kernig’s, Brudzinski’s Motor 5/5 over all extremities, good tone, no atrophy, no fasciculation No sensory deficits (-) Babinski , Kernig, Brudzinski No nuchal rigidity
 Babinski , Kernig, Brudzinski. No nuchal rigidity.")
20
Salient Features Pertinent Positive Age: 53 Sex: F
BP on admission: 200/100, known hypertensive since ____ RR 24 bpm (tachypnea) BMI = 30 (obese) (+) family history Lifestyle Hazy cornea (?)
 BMI = 30 (obese) (+) family history. Lifestyle. Hazy cornea ( )")
21
Salient Features Pertinent Negative (make bullets brief!)
Neck veins not distended No heaves, no thrills, no lifts, S1>S2 apex, S2>S1 base, no murmurs Apex beat at 5th LICS 11cm from the midsternal line Pulses full and equal, no edema, no cyanosis, no clubbing No pertinent respiratory findings No epigastric pain

22
Chest Pain Cardiovascular Pulmonary Gastrointestinal Musculoskeletal

23
DIAGNOSIS: Hypertension
Definition: The elevation of blood pressure above normal range expected of a particular age group - The Bantam Medical Dictionary

24
Blood Pressure Classification
Systolic, mmHg Diastolic, mmHg Normal <120 <80 Prehypertension 80-89 Stage 1 hypertension 90-99 Stage 2 hypertension ≥160 ≥100 Isolated systolic hypertension ≥140 <90 On Admission LUE 200/110 RUE 190/100 LLE 190 systolic RLE 190 systolic Upon PE 110/70 Harrison’s Internal Medicine, 17th Ed

25
Primary hypertension vs. Secondary hypertension
Familial Environmental + genetic Secondary Due to another medical condition

26
Target Organ Damage Heart disease Stroke or TIA Nephropathy
Peripheral arterial disease Retinopathy

27
Risk Factors for Hypertension (summarized)
Old age (M>45; F>55) Obesity Gender – female Lifestyle – diet, drinking alcohol, smoking, amount of exercise Positive family history Chronic stress Prehypertension – blood pressure in 120–139/80–89 mmHg range
 Obesity. Gender – female. Lifestyle – diet, drinking alcohol, smoking, amount of exercise. Positive family history. Chronic stress. Prehypertension – blood pressure in 120–139/80–89 mmHg range.")
28
Pathology

29
Hypertensive Emergency VS. Hypertensive Urgency
Hypertensive Emergency - severe BP elevation (> 180/120 mm Hg) - progressive target-organ dysfunction Hypertensive Urgency - severe BP elevation - NO target-organ dysfunction Rate of change of BP is directly related to the likelihood that an acute hypertensive syndrome will develop
 - progressive target-organ dysfunction. Hypertensive Urgency - severe BP elevation. - NO target-organ dysfunction. Rate of change of BP is directly related to the likelihood that an acute hypertensive syndrome will develop.")
30
Critical level or rapid rate of rise and increased vascular resistance Endothelial damage Spontaneous natriuresis Inc, Endothelial permeability Intravascular volume depletion Decrease in vasodilators, nitric oxide, prostacyclin Platelet and fibrin deposition Increase in vasoconstrictors (renin–angiotensin, catecholamines Fibrinoid necrosis and intimal proliferation Further increase in blood pressure

31
Severe blood pressure elevation Tissue ischemia End-organ dysfunction

32
Pathologic Consequences of Hypertension
Heart- most common cause of death in hypertensive patients - left ventricular hypertrophy diastolic dysfunction, CHF - Inc. risk of CHD, stroke, arrhythmias Brain – brain infarction and hemorrhage (intracerebral or subarachnoid) - encephalopathy- vasodilation and hyperperfusion - related to autoregulation failure Signs and symptoms: severe headache nausea vomiting
 - encephalopathy- vasodilation and hyperperfusion. - related to autoregulation failure. Signs and symptoms: severe headache. nausea. vomiting.")
33
Kidney- direct damage to glomerular capillaries due to hyperperfusion
- may progress to glomerulosclerosis - renal tubules will eventually become ischemic and atrophic Blood Vessels – atherosclerosis secondary to long-standing elevated pressure Eye - retinal hemorrhages, exudates

34
Ischemia Blood supply – important for oxygenation and elimination of waste products Ischemia refers to a lack of oxygen due to inadequate perfusion of the myocardium Imbalance between oxygen demand and supply

35
Factors affecting oxygen supply and demand:

36
Atherosclerosis The most common cause of myocardial ischemia is obstructive atherosclerotic disease of the coronary arteries

37
Macrophage and T lymphocytes Redeposition of oxidized LDL Inflammation
Damage to artery wall Macrophage and T lymphocytes Redeposition of oxidized LDL Inflammation Migration and enlargement of muscle cells Narrowing of lumen

38
Major risk factors for atherosclerosis
Cigarette smoking Hypertension (BP>/= 140/90mmHg) DM Family history of premature CHD Age (men >/= 45 years, women>/=55 years) Lifestyle: obesity(BMI>/= 30kg/m2, physical inactivity, atherogenic diet)
 DM. Family history of premature CHD. Age (men >/= 45 years, women>/=55 years) Lifestyle: obesity(BMI>/= 30kg/m2, physical inactivity, atherogenic diet)")
39
Concentric Hypertrophy

40
Ancillary Procedures

41
Blood Tests Results Normal values FBS 100 mg/dL 70.9-110 Cholesterol
Triglycrides 106 mg/dL 0-210 HDL 46.2 mg/dL 30-90 LDL 145 mg/dL 66-178 SGPT 34.2 U/L 0-31 Creatinine 0.80 mg/dL Sodium 141 mmol/L Potassium 3.5 mmol/L 3.8-5

42
CBC Hgb 113 g/L RBC 3.62 x 10^12/L Hct 0.34 MCV 92.70 U^3 87 +-5 MCH 31.20 pg 29 +-2 MCHC 33.70 g/dL 34 +-2 RDW 11.90 MPV 8.30 fL Platelet 298 x 10^9/L WBC 5.70 x 10^9/L Differential Count Neutrophils 0.49 Lymphocytes 0.47 Monocytes 0.03 Eosinophils 0.01 Basophils

43
Urinalysis Color – Light yellow Transparency – Slightly Turbid pH 6.5
Specific Gravity 1.015 Albumin and Sugar – Negative Pus cells 2-4/ hpf Squamous cells + Renal Cell – few Bacteria – few Amorphous urate + Calcium oxalate ++

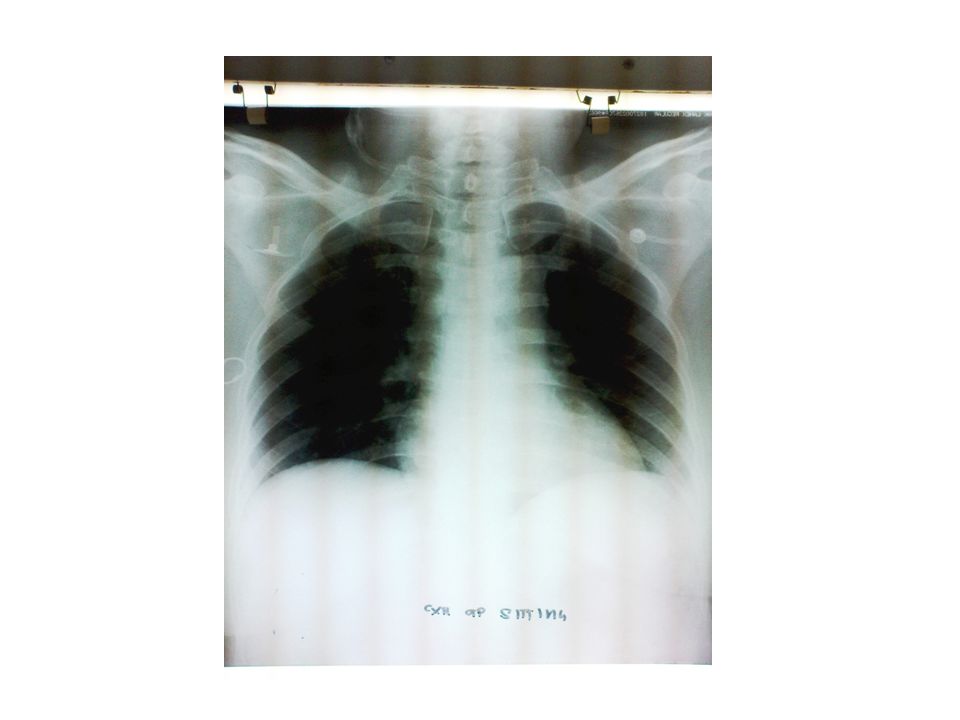
45
Radiology

47
PHARMACOLOGY

48
Identify Problems Chest pain Hypertension Diet

49
Set therapeutic goals To gradually decrease systolic blood pressure
To prevent recurrence of chest pain To prevent progression of symptoms To promote and develop a healthy lifestyle

50
Pharmacologic Therapies
Dihydropyridine calcium channel blocker – nicardipine Angiotensin receptor blocker – irbesartan Diuretic – hydrochlorothiazide β blocker – metoprolol Nitrate – isosorbide mononitrite Antihyperlipidemic - simvastatin Aspirin

51
Non-pharmacologic Approaches
Lifestyle change/modifications Lose extra weight Diet: less salt Exercise Follow DASH (Dietary Approach to Stop Hypertension) which includes diet rich in fruits, vegetables, and low-fat dairy products and is low in fat.
 which includes diet rich in fruits, vegetables, and low-fat dairy products and is low in fat.")
Similar presentations






 Male Filipino Roman Catholic Sampaloc, Manila Informant: Mother Reliability: Good.>")



>")









