Download presentation
Presentation is loading. Please wait.

1
Brachytherapy and GYN malignancy

2
Brachytherapy Brachytherapy (brachy, from the Greek for “short distance”) consists of placing sealed radioactive sources close to or contact with the target tissue. Interstitial, intracavity, or transluminal approach. Temporary, or permanent implant. Low or high dose rate.
 consists of placing sealed radioactive sources close to or contact with the target tissue. Interstitial, intracavity, or transluminal approach. Temporary, or permanent implant. Low or high dose rate.")
3
Introduction Discovery in 1898 Short distance (cm)
High radiation dose can be delivered locally to the tumor with rapid dose fall-off in the surrounding normal tissue

5
Radioactive sources

6
Radioactive sources Radium-226
Average energy 0.83Mev (0.5mm of platinum) A filtration of at least 0.5mm platinum is sufficient to absorb all the α particles and most of the β particles emitted by the radium and its daughter products. Half life ~1600 years It was loaded into cells about 1cm long and 1mm in diameter. Radium sources are manufactured as needles or tubes in a variety of lengths and activities
 A filtration of at least 0.5mm platinum is sufficient to absorb all the α particles and most of the β particles emitted by the radium and its daughter products. Half life ~1600 years. It was loaded into cells about 1cm long and 1mm in diameter. Radium sources are manufactured as needles or tubes in a variety of lengths and activities.")
7
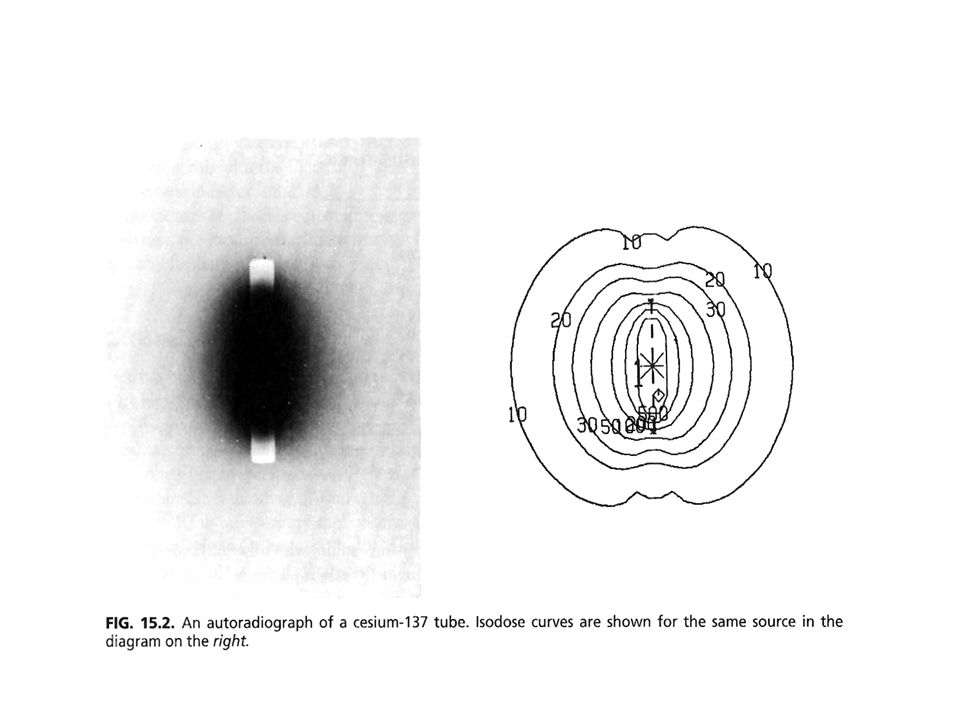
Radioactive sources Cesium-137
Substitute for radium in both interstitial and intracavitary brachytherapy Energy Mev nearly the same penetrating power as radium Half life 30 years (clinically used 7 years without replacement) It was doubly encapsulated in stainless-steel needles and tubes.
 It was doubly encapsulated in stainless-steel needles and tubes.")
9
Radioactive sources Cobalt-60
High specific activity Small sources required for some special applicators More expensive than 137Cs and short half life (5.26 years) The sources can be used to replace 226Ra in intracavitary application
 The sources can be used to replace 226Ra in intracavitary application.")
10
Radioactive sources Iridium-192
It has a complicated γ ray spectrum with an average energy of 0.38 MeV. → It required less shielding for personnel protection. It has the disadvantage of a short half-life (73.8 days) It is fabricated in the form of thin flexible wires which can be cut to desired lengths
 It is fabricated in the form of thin flexible wires which can be cut to desired lengths.")
11
Radioactive sources Iodine-125
Widely used for permanent implants. Longer half-life: 59.4 days (convenient for storage) Low photon energy (0.028MeV) → less shielding. Disadvantages: dosimetry of 125I is much more complex.
 Low photon energy (0.028MeV) → less shielding. Disadvantages: dosimetry of 125I is much more complex.")
12
Brachytherapy Permanently Implanted
Source Energy T1/2 Dose Rate 222Rn 1.2MeV 3.83 0.75G/h 198Au 412keV 2.70 1.07G/h 125I 28keV 59.6 0.07G/h 13Pd 22keV 17 0.19G/h

13
Radioactive sources ICRU38 LDR sources: 0.4-2 Gy/hr (137Cs)
HDR sources: ≥ 12 Gy/hr (60Co, 192Ir) 226Ra leakage Radon gas. 137Cs better than 226Ra less shielding and microsphere form with leakage gas. 137Cs better than 60Co less shielding and cheap. 192Ir better than 137Cs lower energy require less shielding for personnal protection and higher specific activity. 103Pd better than 198Au and 125I less shielding and biologic advantage .
 226Ra leakage Radon gas. 137Cs better than 226Ra less shielding and microsphere form with leakage gas. 137Cs better than 60Co less shielding and cheap. 192Ir better than 137Cs lower energy require less shielding for personnal protection and higher specific activity. 103Pd better than 198Au and 125I less shielding and biologic advantage .")
14
Radioactive sources Low Dose Rate (LDR) High Dose Rate (HDR) Patient
Long history of use. Ability to predict rate of late complications No long term confinement to bed. No indwelling bladder catheters. Not labeled “radiation risk zone” to relative, visitors, and staff. Avoid several anesthesias. Clinical Improves chances of atching tumors in sensitive phase of cell cycle. Maintain position of the sources during the brief treatment. Patient preparation. No specialized nursing. Ability to treat great patient loads. Physical Longer treatment times allow for leisurely review of and potential modifications to the treatment . Plan prior to the delivery of a significant portion of treatment. Favorable dose-rate effect on repair of normal tissues. Infrequent replacement and calibration of sources because of long isotope half-life. Short treatment times and minimal radiation protection problems. Possibility of optimizing dose distribution by altering the dwell times of the source at different

17
Brachytherapy and GYN Malignancy

18
Reference point from which lymph node position were measured on lymphoangiograms and the range of location Int. J Radiat Oncol Biol Phys 34: , 1996

19
Distribution of pelvic node metastases in patients with Ib-IIa cervical cancer Gynecol Oncol 62:19-24, 1996 Tumor size <=4 cm Local advanced tumor

20
External beam radiotherapy for GYN Malignancy

21
Pelvic irradiation portal in cervical cancer 4-field box technique

22
Pelvic irradiation portal in cervical cancer 4-field box technique

24
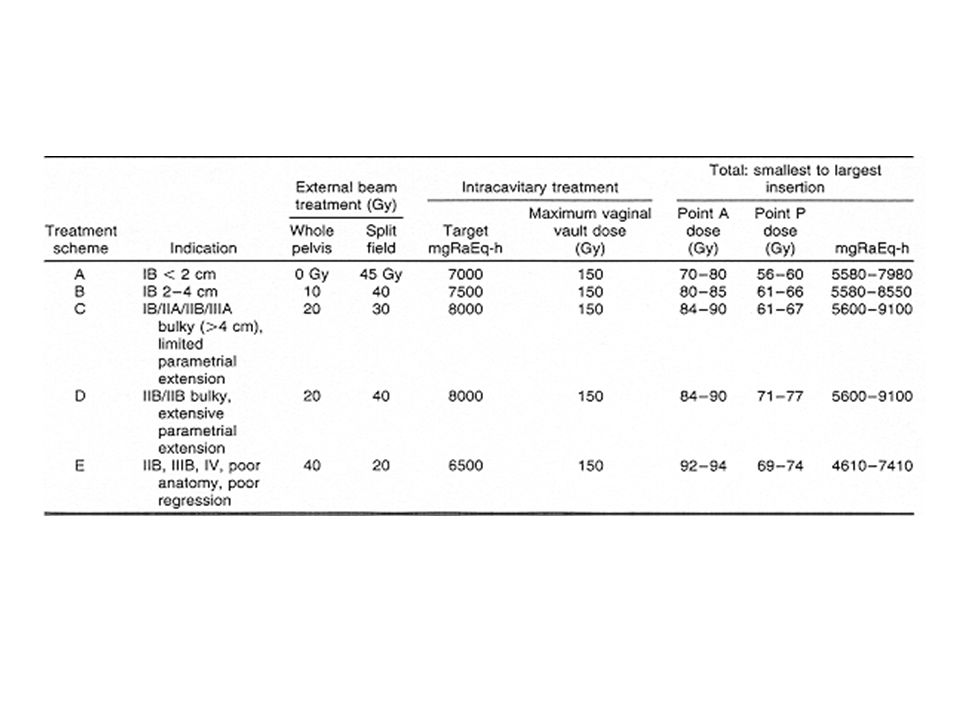
Combination of external beam pelvic irradiation and intracavitary brachytherapy (ICRT)
")
25
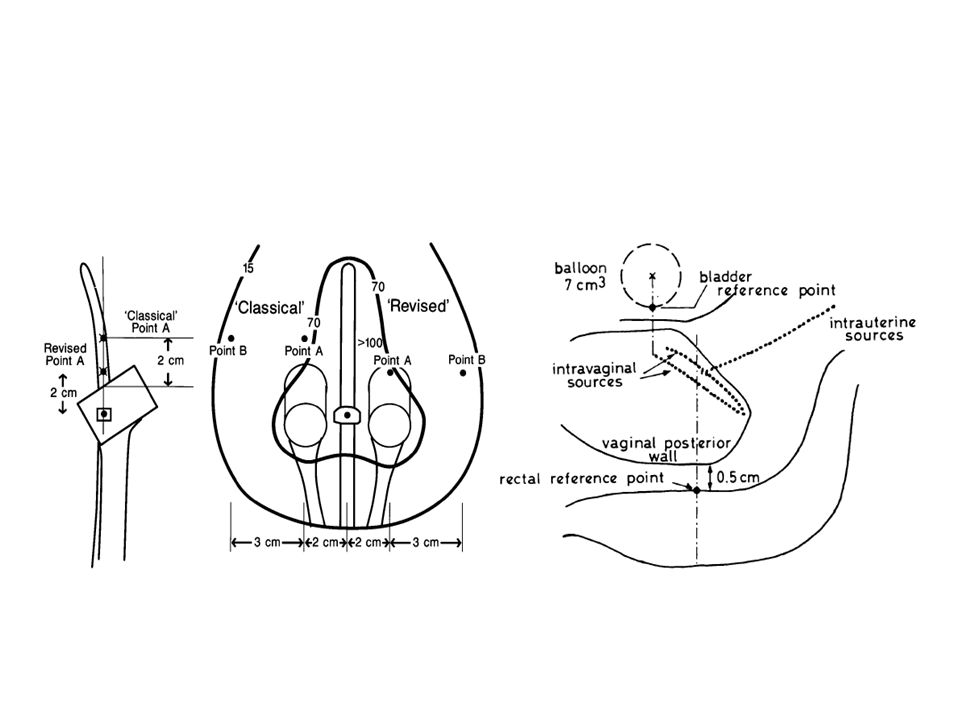
Brachytherapy in definitive radiotherapy of cervical cancer (Intracavity radiotherapy, ICRT)
")
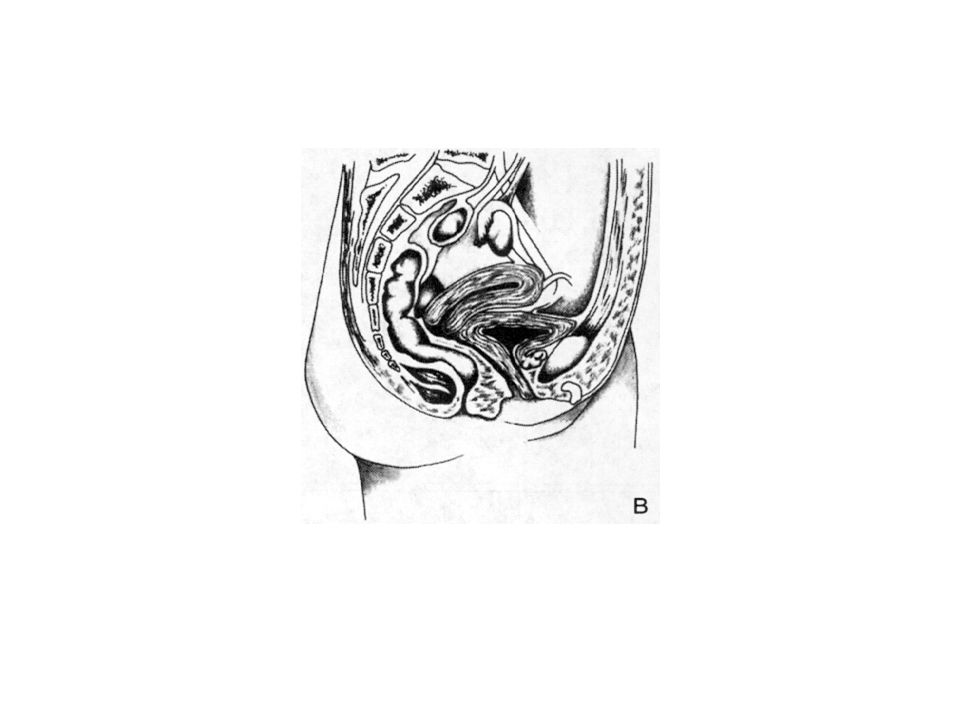
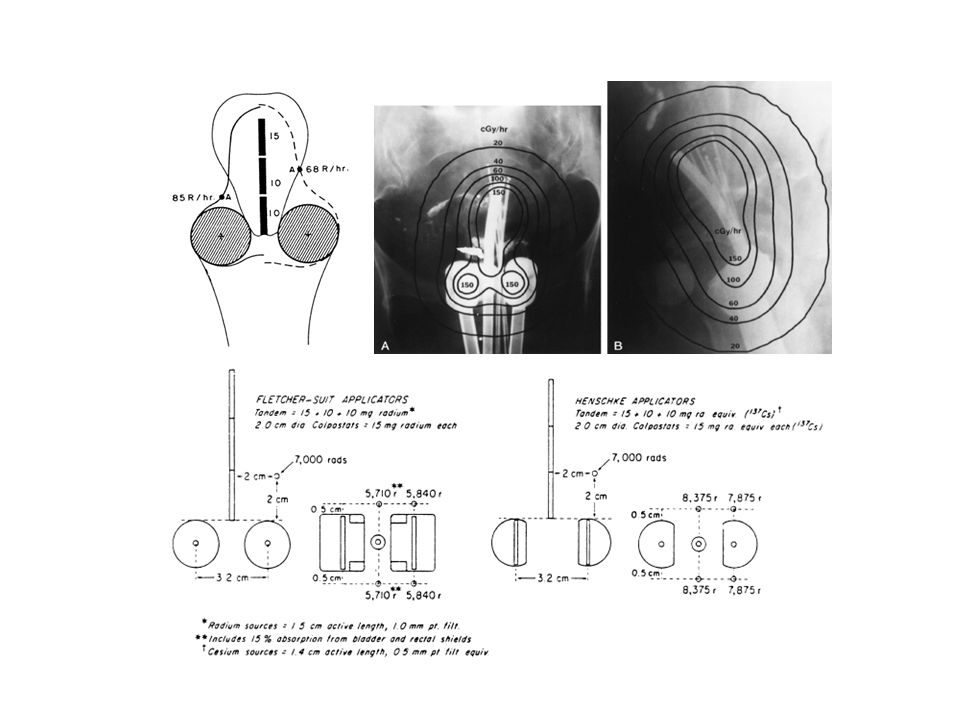
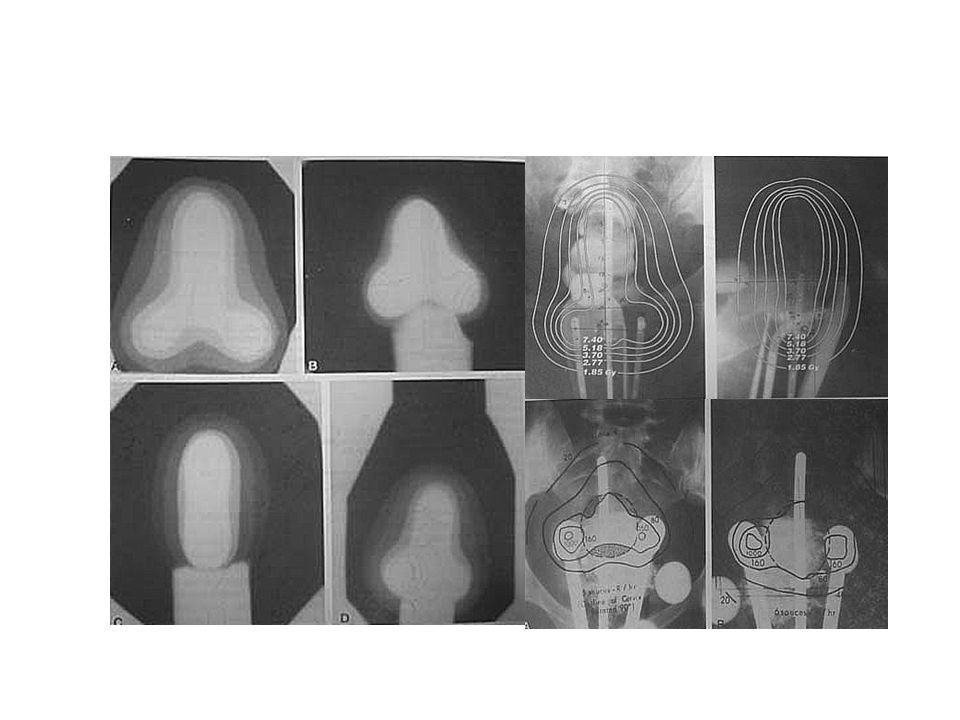
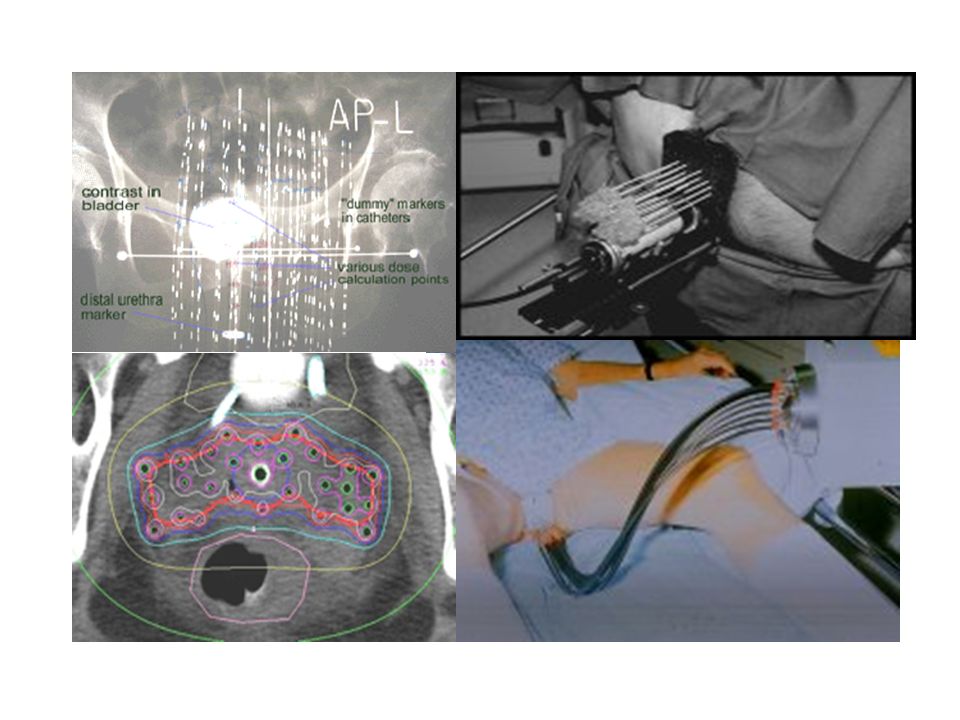
26
Intracavitary Radiotherapy (ICRT)
")
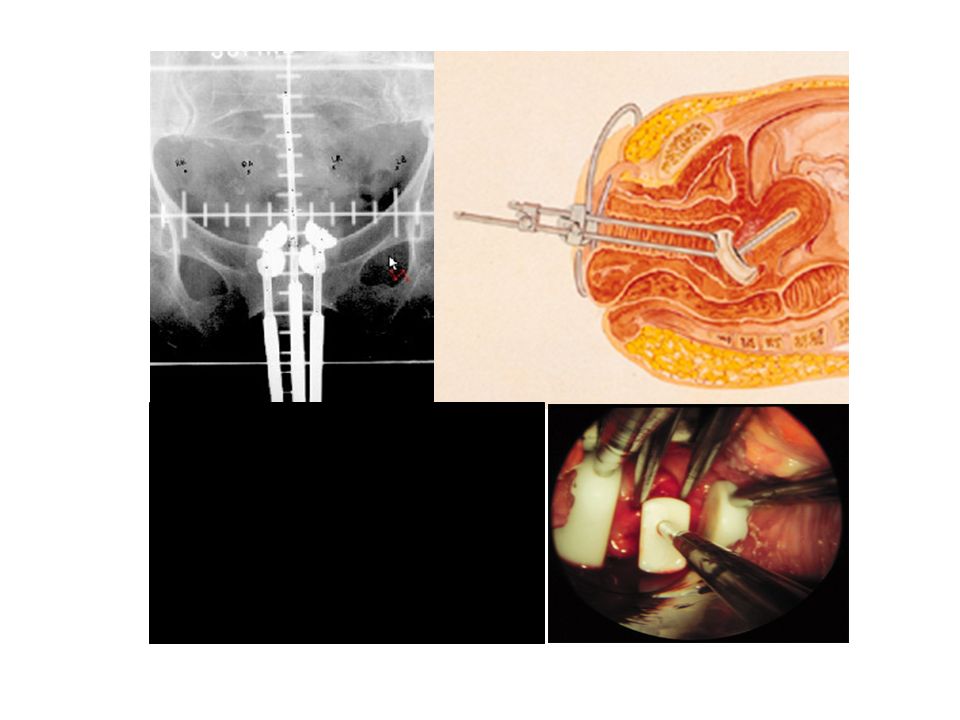
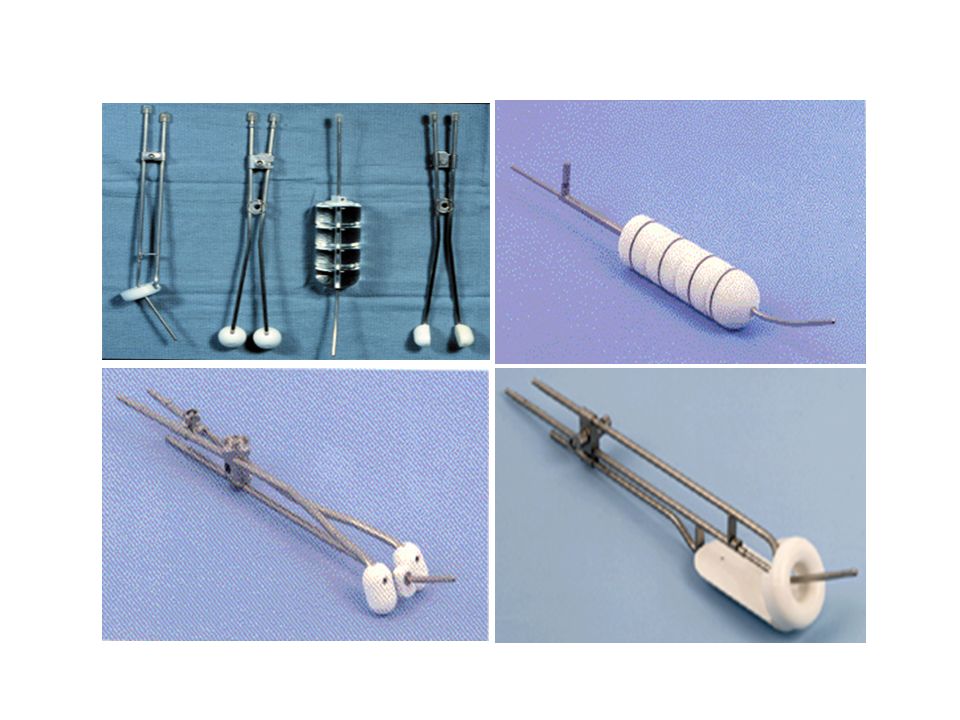
30
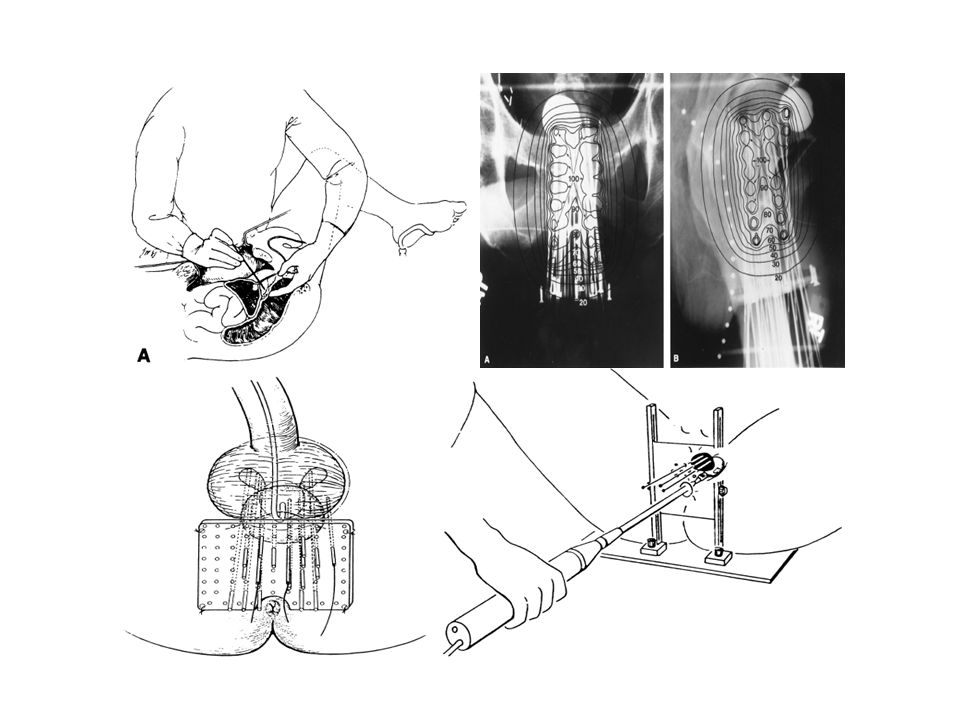
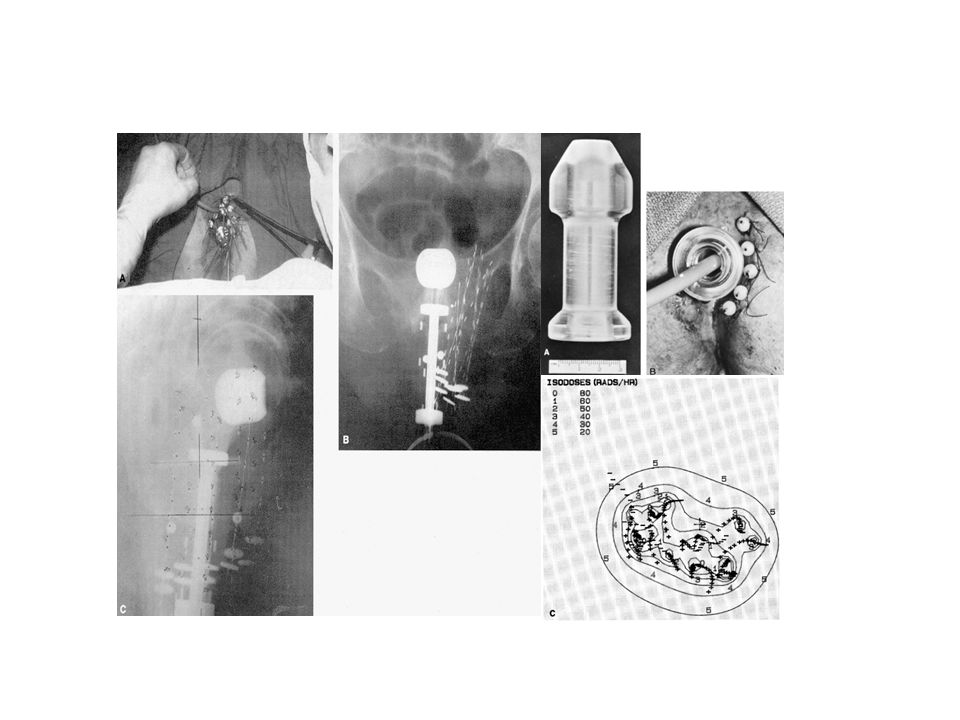
Applicator of ICRT

33
Intracavitary insertion (ICRT)
")
40
Postoperative brachytherapy (Intravaginal radiotherapy)
")
41
Intravaginal radiotherapy (IVRT)
")
44
Female urethral cancer

46
Endometrial cancer

Similar presentations






















: Brachytherapy Techniques IAEA Training Material on Radiation Protection in.>")




