Download presentation
Presentation is loading. Please wait.

1
Opioids plus adjuvants for cancer pain: systematic review Mike Bennett Professor of Palliative Medicine Lancaster University, UK

2
Introduction

3
Rationale Cancer pain mechanisms – Often mixed – Neuropathic mechanisms present in 35-39% Adjuvant drugs often needed – Target specific neuropathic mechanisms – Evidence supports antidepressants and antiepileptics in non-cancer pain

4
Pharmacology Antidepressants (TCAs) – Inhibit presynaptic uptake of 5HT and NA – Block voltage dependent sodium channels – Nortriptyline more active at NA Antiepileptics – Gabapentinoids Block α 2 δ subunit of calcium channels and reduce excitatory neurotransmitters – Older drugs Block voltage dependent sodium channels
 – Inhibit presynaptic uptake of 5HT and NA – Block voltage dependent sodium channels – Nortriptyline more active at NA Antiepileptics – Gabapentinoids Block α 2 δ subunit of calcium channels and reduce excitatory neurotransmitters – Older drugs Block voltage dependent sodium channels")
5
Pain scores at end of each arm (5.7 at baseline): – placebo 4.5 – gabapentin 4.2 – morphine 3.7 – M + GP 3.1
: – placebo 4.5 – gabapentin 4.2 – morphine 3.7 – M + GP 3.1")
6
European Neurology 2009

7
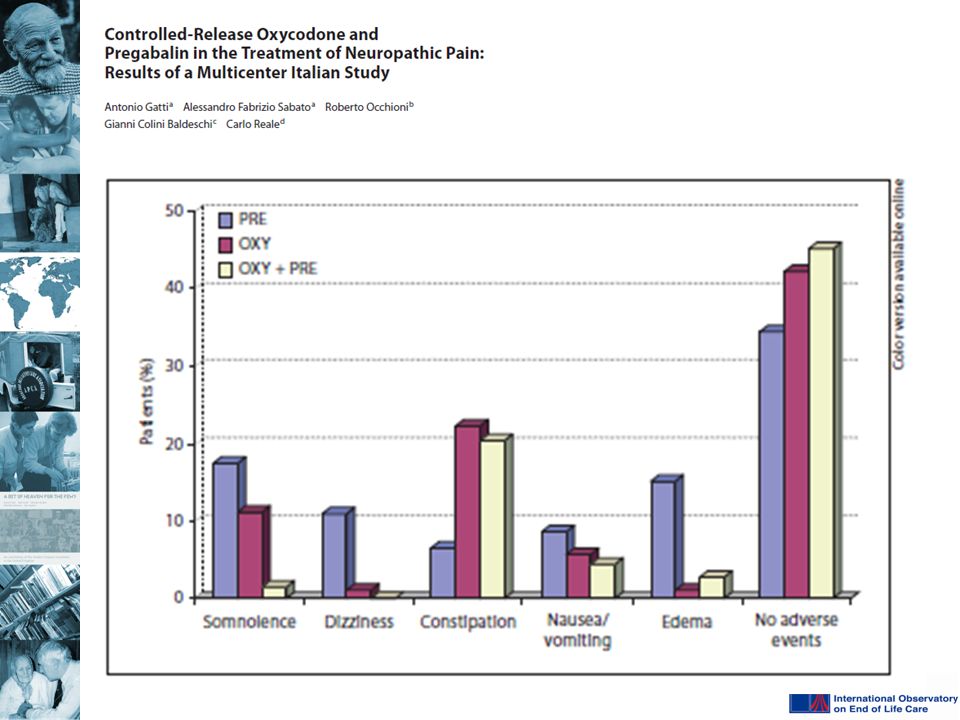
In non-cancer pain – Opioids plus adjuvants are more effective than monotherapy Morphine plus gabapentin (Gilron 2005) Oxycodone plus gabapentin (Hanna 2008) Oxycodone plus pregabalin (Gatti 2009) – Effect size At least moderate relief – G=61%, M=80%, MG=78%, P=31% Good or very good relief – G=41%, OG=56% – Adverse effects of combinations Generally similar to opioid alone
 Oxycodone plus gabapentin (Hanna 2008) Oxycodone plus pregabalin (Gatti 2009) – Effect size At least moderate relief – G=61%, M=80%, MG=78%, P=31% Good or very good relief – G=41%, OG=56% – Adverse effects of combinations Generally similar to opioid alone")
8
What is the effectiveness of adjuvants and opioids compared to opioids alone for cancer pain?

9
Methods

10
Search for studies that: – Had adult patients with pain from active cancer – Prospectively compared adjuvant and opioid to opioid alone – Used before-after, or RCT design – Assessed pain, pain relief and adverse effects

11
8 eligible studies – 5 were RCTs – 3 ‘before-after’ designs Patients recruited – 465 in total, 370 (79.5%) completed study – 6 studies specified neuropathic pain – 2 had chronic cancer pain Drugs – Gabapentin (4) – Valproate (1), phenytoin (1) – Amitriptyline (1), imipramine (1)
 completed study – 6 studies specified neuropathic pain – 2 had chronic cancer pain Drugs – Gabapentin (4) – Valproate (1), phenytoin (1) – Amitriptyline (1), imipramine (1)")
12
Study duration – Median 14 days (range 7 - 28 days) – 7 studies collected outcomes within 4-8 days Dosing – Adjuvant added to fixed opioid dose (5) – Adjuvant added to variable opioid dose (2) – Combination arm had 50% of both drugs (1)
 – 7 studies collected outcomes within 4-8 days Dosing – Adjuvant added to fixed opioid dose (5) – Adjuvant added to variable opioid dose (2) – Combination arm had 50% of both drugs (1)")
13
Results

14
Pain Mean additional benefit on average pain Significant differences Gabapentin – RCTs 0.8 points (Caraceni 2004) 1.6 burning pain, 2.1 shooting pain (Keskinbora 2007) – no overall pain assessment – Observational 1.8 points (Ross 2005) 3.2 points (Caraceni 1999)
 1.6 burning pain, 2.1 shooting pain (Keskinbora 2007) – no overall pain assessment – Observational 1.8 points (Ross 2005) 3.2 points (Caraceni 1999)")
15
Amitriptyline (RCT, Mercadante 2002) – 0.9 points (worst pain) Imipramine (RCT, Walsh 1986) – ‘pain scores similar’ but no details significantly lower opioid doses in combination arm No data for valproate or phenytoin
 – 0.9 points (worst pain) Imipramine (RCT, Walsh 1986) – ‘pain scores similar’ but no details significantly lower opioid doses in combination arm No data for valproate or phenytoin")
16
Pain relief Proportion with 30% pain relief Gabapentin – Intervention 62%, Control 64% (Caraceni 2004) – 45% (Ross 2005) Amitriptyline – ‘No differences’ on 0-10 scale
 – 45% (Ross 2005) Amitriptyline – ‘No differences’ on 0-10 scale")
17
Proportion with 50% pain relief – Vaproate (Hardy 2001, observational) 27.8%, no analysis – Phenytoin (Yajnik 1992, RCT) Combination = 88% Opioid alone = 84%, no sig diff
 27.8%, no analysis – Phenytoin (Yajnik 1992, RCT) Combination = 88% Opioid alone = 84%, no sig diff")
18
Adverse effects Gabapentin – Intervention 36% (1 death and 1 resp dep), Control 17% (Caraceni 2004) – Intervention 29%, Control 59% (Keskinbora 2007) constipation in control arm, but most switched to oral morphine after randomisation while intervention arm continued on fentanyl Phenytoin – Fewer events in intervention arm 50% dose reduction in combination arm Amitriptyline – More adverse events (drowsy and confused)
, Control 17% (Caraceni 2004) – Intervention 29%, Control 59% (Keskinbora 2007) constipation in control arm, but most switched to oral morphine after randomisation while intervention arm continued on fentanyl Phenytoin – Fewer events in intervention arm 50% dose reduction in combination arm Amitriptyline – More adverse events (drowsy and confused)")
19
Discussion

20
Main findings Addition of adjuvant: – Significant but modest benefit on pain Unlikely to be greater than 1 point difference – Increase in adverse events – Strongest evidence supports gabapentin

21
But…. 3 studies reported: – Reduced opioid +/- adjuvant doses in combination arm – Same or better pain control – Fewer adverse events in combination arm 5 studies reported: – Fixed doses of opioids when adjuvant added – Modest improvements in pain – More adverse events in combination arm

24
Also…. Benefits apparent within 4-8 days for cancer patients – Little or no additional benefit after this period

25
Summary Opioids plus adjuvants in cancer pain: – Modest additional benefit 1 point on 0-10 scale In this context, NNT higher for adjuvants, NNH lower Opioids alone are effective – Any benefits of combination apparent within a week increase dose or switch if no effect at this point – Reducing dose of opioid when adding adjuvant Probably results in fewer adverse events for same or better pain control

26
Thank you m.i.bennett@lancaster.ac.uk

Similar presentations