Download presentation
Presentation is loading. Please wait.

1
Advantages of Laparoscopy for Diverticulitis Steven D. Wexner, M.D., FACS, FRCS, FRCS (Ed) Cleveland Clinic Florida Chairman, Department of Colorectal Surgery Chief of Staff, Cleveland Clinic Florida Professor of Surgery, Ohio State University Health Sciences Center at the Cleveland Clinic Foundation Clinical Professor of Surgery, University of South Florida College of Medicine
 Cleveland Clinic Florida Chairman, Department of Colorectal Surgery Chief of Staff, Cleveland Clinic Florida Professor of Surgery, Ohio State University Health Sciences Center at the Cleveland Clinic Foundation Clinical Professor of Surgery, University of South Florida College of Medicine.")
2
Cleveland Clinic Florida Weston

3
> Advantages –Operative time –Morbidity –Hospital Length of Stay > Special considerations –Presence of complications –Conversion –Advantages for elderly –Advantages for obese –Cost Advantages of Laparoscopy: Diverticulitis

4
Laparoscopy: Diverticulitis

5
Modified Hinchey* Grading System I.Pericolic abscess IIA.Distant abscess amenable to percutaneous drainage drainage IIB.Complex abscess associated with fistula III.Generalized purulent peritonitis IV.Fecal peritonitis *Adv Surg 1978

6
Author/yearnLap/Open Op time (min) Morbidity (%) Hospital stay (days) Kholer/98 27 34 Lap Open 165* 121 16 61.7 7.9* 14.3 Dwivedi/02 66 88 Lap Open 212* 143 18 23.8 4.8* 8.8 Senagore/02 61 71 Lap Open 109 101 1.6* 12.6 3.1* 6.8 Lawrence/03 56 215 Lap Open 170** 140 9* 27 4.1** 9.0 *p<0.05**p<0.001 Case-Controlled Series Advantages of less morbidity and shorter hospitalization
 Morbidity (%) Hospital stay (days) Kholer/ Lap Open 165* * 14.3 Dwivedi/ Lap Open 212* * 8.8 Senagore/ Lap Open * * 6.8 Lawrence/ Lap Open 170** 140 9* ** 9.0 *p<0.05**p<0.001 Case-Controlled Series Advantages of less morbidity and shorter hospitalization")
7
Laparoscopy: Diverticulitis Retrospective/prospective results – Hospital Stay Laparoscopy: Diverticulitis Retrospective/prospective results – Hospital Stay Author/yearn Hospital stay (days) Eijsbouts/97416.5 Carbajo/98225.5 Stevenson/981004 Bokobza/98 (A) 136--- Bouillot/985010 Smadja/99546.4 Sirisier/99657.6 Vargas/99694.2 Berthou/991108.2 Trebuchet/011708.5 Bouilott/021799.3
 Eijsbouts/ Carbajo/ Stevenson/ Bokobza/98 (A) Bouillot/ Smadja/ Sirisier/ Vargas/ Berthou/ Trebuchet/ Bouilott/")
8
Author/yrn Setting surgery Op time Morbidity (%) Hospital stay (days) Sher/97612 Hinchey I Hinchey IIa/b 215213033.356 Kockerling/99 24955Chronic Hinchey I/IV 159 182 14.8 28.9 ------ Schlachta/ 99 807022OtherChronicAcute 165 150 165 12.81818556 Bergamashi/004034Intracorporeal Lap. assisted 180* 244 180* 244 15** 15**14.7------ Eijsbouts/003535 Lap. Assisted Facilitated resec. 195 150 208.6------ Pugliese/04494112 Hinchey I Hinchey II Hinchey III 18719320014<150910.510 *p<0.001 **p<0.05 Laparoscopy: Diverticulitis Retrospective/Prospective Results - Morbidity The more complicated the diverticular disease, the tendency for higher morbidity and longer lengths of hospital stay

9
Author/yearnLSR/OSR Op time (min) Morbidity(%) Bruce/96 2517LSROSR 397** 115 397** 115121 Liberman/97 1414LSROSR1921831414 Kholer/98 2734LSROSR 165* 121 165* 1211661.7 Dwivedi/02 6688LSROSR 212* 212*1431823.8 Senagore/02 6171LSROSR109101 1.6* 12.6 Lawrence/03 56215LSROSR 170** 170**1409*27 *p<0.05 **p<0.001 Laparoscopy: Diverticulitis - Comparative Studies
 Morbidity(%) Bruce/ LSROSR 397** ** Liberman/ LSROSR Kholer/ LSROSR 165* * Dwivedi/ LSROSR 212* 212* Senagore/ LSROSR * 12.6 Lawrence/ LSROSR 170** 170**1409*27 *p<0.05 **p<0.001 Laparoscopy: Diverticulitis - Comparative Studies")
10
Laparoscopy: Diverticulitis > 1/95-1/98: 1118 patients > Laparoscopic colorectal surgery study group > 509 sigmoid colectomies > 304 diverticulitis > 249 (81.9%) –Peridiverticulitis –Recurrent inflammation –Stenosis > 26 Hinchey I > 9 Hinchey II > 2 Hinchey III Köckerling et al., Surg Endosc 1999
 –Peridiverticulitis –Recurrent inflammation –Stenosis > 26 Hinchey I > 9 Hinchey II > 2 Hinchey III Köckerling et al., Surg Endosc 1999")
11
Laparoscopy: Diverticulitis StageConversion Mean operative time Morbidity (n (%))(min (range)) (%) Total22/304 (7.2)164 (65-410)17 Chronic12/249 (4.8)159 (65-395)14.8 Hinchey I-IV10/55 (18.2)182 (90-410)28.9 I8/26 (30.7)183 (100-410)33.3 II1/9 (11.1)198 (90-320)37.5 III/IV0/2 (0)110 (100-120)50 Köckerling et al., Surg Endosc 1999
)(min (range)) (%) Total22/304 (7.2)164 (65-410)17 Chronic12/249 (4.8)159 (65-395)14.8 Hinchey I-IV10/55 (18.2)182 (90-410)28.9 I8/26 (30.7)183 ( )33.3 II1/9 (11.1)198 (90-320)37.5 III/IV0/2 (0)110 ( )50 Köckerling et al., Surg Endosc 1999")
12
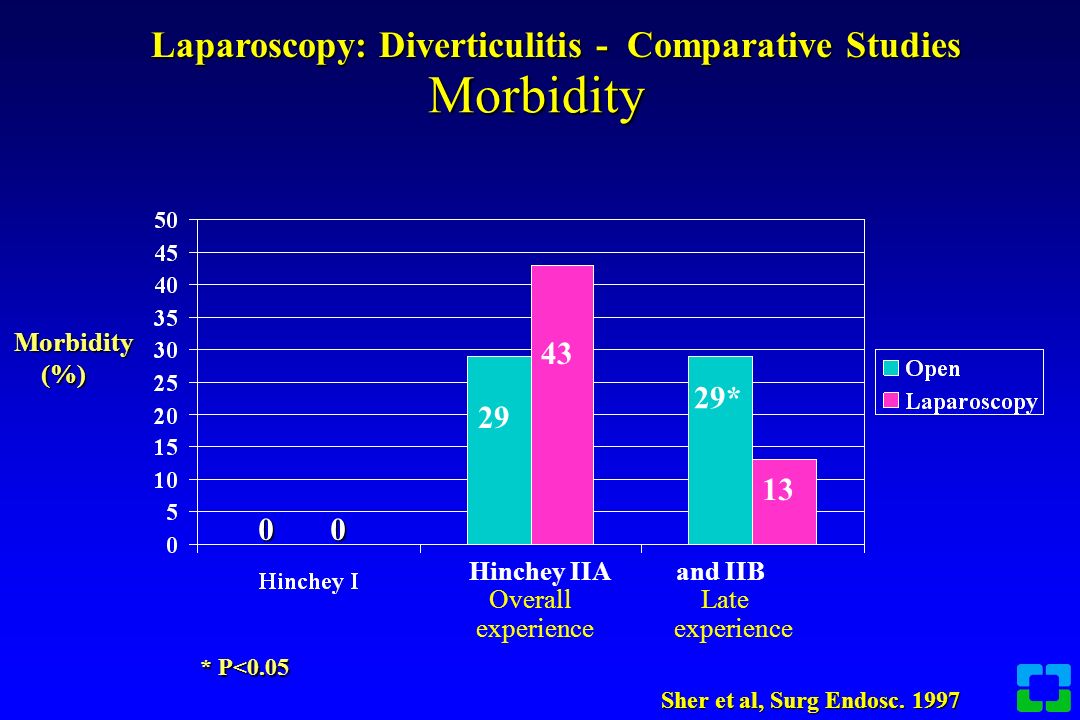
Mean age, 59.5 years Mean age, 69.5 years Mean age, 67.9 years Mean age, 54.3 years Mean age, 65.9 years Mean age, 67.7 years #patients Sher et al, Surg Endosc. 1997 Laparoscopy: Diverticulitis Comparative Study n = 18 Laparoscopy: Diverticulitis Comparative Study n = 18

13
Morbidity Hinchey IIA and IIB Overall Late experience experience 0 0 29 43 29* 13 * P<0.05 Morbidity (%) (%) Laparoscopy: Diverticulitis - Comparative Studies Sher et al, Surg Endosc. 1997
14
Open vs. Laparoscopy Hospital stay 7* 5 10 † 5 9* Days * p<0.05 † p<0.01 Laparoscopy Laparoscopy: Diverticulitis Sher et al, Surg Endosc. 1997

15
Results Demographics 1996-19981991-1995 n1518 Mean age (yrs)69.7(51-91) 62.8(34.-86) Gender (M:F)10:58:10 Operative time (min)209213 Hospitalization (days)6.97.4 Sher et al, Surg Endosc, 1997
69.7(51-91) 62.8(34.-86) Gender (M:F)10:58:10 Operative time (min) Hospitalization (days) Sher et al, Surg Endosc, 1997")
16
Results Hinchey Classification 1996-19981991-1995Total (%)(%)(%) Hinchey I10 (66.6)6(33)16(48) Hinchey IIA3(20)7(38)10(30) Hinchey IIB2(13)5(27)7(21) Hinchey III000 Hinchey IV000 Sher et al, Surg Endosc, 1997
(%)(%) Hinchey I10 (66.6)6(33)16(48) Hinchey IIA3(20)7(38)10(30) Hinchey IIB2(13)5(27)7(21) Hinchey III000 Hinchey IV000 Sher et al, Surg Endosc, 1997")
17
Results Morbidity 1996-19981991-1995 (%)(%) Intraoperative02(11) colotomy01 enterotomy00 Postoperative 2(13.3)1(5.5) Leak (reoperation)11 Bleeding (converted)10 TOTAL2(13.3)3(16.6) TOTAL2(13.3)3(16.6) Sher et al, Surg Endosc, 1997
(%) Intraoperative02(11) colotomy01 enterotomy00 Postoperative 2(13.3)1(5.5) Leak (reoperation)11 Bleeding (converted)10 TOTAL2(13.3)3(16.6) TOTAL2(13.3)3(16.6) Sher et al, Surg Endosc, 1997")
18
Results Conversion 1996-1998 2 (13.3)* > 1 extensive adhesions (Hinchey IIB) > 1 bleeding (Hinchey I) 1991-1995 7 (38.9)* > 6 intense inflammatory process (all Hinchey II) > 1 inadvertent enterotomy (Hinchey II) *p<0.04 Sher et al, Surg Endosc, 1997
* > 1 extensive adhesions (Hinchey IIB) > 1 bleeding (Hinchey I) (38.9)* > 6 intense inflammatory process (all Hinchey II) > 1 inadvertent enterotomy (Hinchey II) *p<0.04 Sher et al, Surg Endosc, 1997")
19
Laparoscopy: Diverticulitis LaparoscopyLaparotomyp n1414ns Operative time 192182ns (minutes) Blood loss171321<0.04 Postoperative stay6.39.2<0.0001 (days) Day to P.O fluids2.96.1<0.001 Liberman, Surg Endosc 1996
 Blood loss171321<0.04 Postoperative stay6.39.2< (days) Day to P.O fluids2.96.1<0.001 Liberman, Surg Endosc 1996")
20
Laparoscopy: Diverticulitis Retrospective review VariableLaparoscopicOpen n2517 Age (years)5248 Gender (m/f)13/1213/4 Weight (kg)80.683.2 Comorbidity (%)2840 Prior laparotomy (%)5629 Flexure mobilized (%)2424 Left colectomy13 Bruce et al., DCR 1996
5248 Gender (m/f)13/1213/4 Weight (kg) Comorbidity (%)2840 Prior laparotomy (%)5629 Flexure mobilized (%)2424 Left colectomy13 Bruce et al., DCR 1996")
21
Laparoscopy: Diverticulitis VariableLaparoscopicOpen Conversion (%)12--- Operative time (minutes)*397115 Regular diet (days)*3.25.7 Hospital stay (days)*4.26.8 Cost ($)*10,2307,068 Post-discharge817 morbidity Bruce et al., DCR 1996 (* p<0.001)
12--- Operative time (minutes)* Regular diet (days)* Hospital stay (days)* Cost ($)*10,2307,068 Post-discharge817 morbidity Bruce et al., DCR 1996 (* p<0.001)")
22
Laparoscopy: Diverticular disease VariableLaparoscopicOpen Age (years)5952 Weight (pounds)165172 ASA class2.32.1 Perforated75 Abscess1818 Operative time (minutes)*190108 Blood loss (ml)340308 Coogan et al, Surg Endosc 1997 (P<0.001)
5952 Weight (pounds) ASA class Perforated75 Abscess1818 Operative time (minutes)* Blood loss (ml) Coogan et al, Surg Endosc 1997 (P<0.001)")
23
Laparoscopy: Diverticular disease VariableLaparoscopicOpen Oral intake (days)*0.85.1 Hospital stay (days)**3.89.3 OR cost ($)15,2007,200 Hospital cost ($)1,7006,800 Total cost ($)17,00015,800 *p<0.0001**p<0.001 Coogan et al, Surg Endosc 1997
* Hospital stay (days)** OR cost ($)15,2007,200 Hospital cost ($)1,7006,800 Total cost ($)17,00015,800 *p<0.0001**p<0.001 Coogan et al, Surg Endosc 1997")
24
Laparoscopy: Diverticulitis VariableLaparoscopyLaparotomyp (n=40)(n=35) Age (mean years)6062ns Gender (m/f)26/1422/13 ns Weight (kg)75 (1.0) 76 (1.1)ns ASA Grade (I:II)22:18 23:12ns Symptoms duration 16 17ns (months) Previous admissions 1.9 1.6ns Bergamaschi and Arnaud, Surg Endosc 1998
(n=35) Age (mean years)6062ns Gender (m/f)26/1422/13 ns Weight (kg)75 (1.0) 76 (1.1)ns ASA Grade (I:II)22:18 23:12ns Symptoms duration 16 17ns (months) Previous admissions ns Bergamaschi and Arnaud, Surg Endosc 1998")
25
Laparoscopy: Diverticulitis VariableLaparoscopyLaparotomyp (n=40)(n=35) Specimen length (cm) 11 18<0.01 Splenic flexure 29:11 17:18 ns mobilized (no:yes) Anastomosis (CS:CR) 1:3924:11<0.01 Inflammatory cells* 112=0.02 Radiographic leak 00ns * Proximal resection margin (CS- colosigmoid, CR- colorectal) Bergamaschi and Arnaud, Surg Endosc 1998
(n=35) Specimen length (cm) 11 18<0.01 Splenic flexure 29:11 17:18 ns mobilized (no:yes) Anastomosis (CS:CR) 1:3924:11<0.01 Inflammatory cells* 112=0.02 Radiographic leak 00ns * Proximal resection margin (CS- colosigmoid, CR- colorectal) Bergamaschi and Arnaud, Surg Endosc 1998")
26
Laparoscopy: Diverticulitis VariableLaparoscopyLaparotomyp Radiographic leak00ns Follow-up (months)46 63 <0.01 Recurrent2.7 9.6 ns diverticulitis (%) Bergamaschi and Arnaud, Surg Endosc 1998
46 63 <0.01 Recurrent ns diverticulitis (%) Bergamaschi and Arnaud, Surg Endosc 1998")
27
Open vs. Laparoscopy Author/yearnLap/OpenOp time (min) Morbidity (%) Hospital stay (days) Bruce/9625 17 Lap Open 397** 115 12 1 4.2 6.8 Liberman/9614 Lap Open 192 18314 6.3** 9.2 Coogan/9759 52 Lap Open 190 108 -3.8 9.3 Kholer/9827 34 Lap Open 165* 121 16 61.7 7.9* 14.3 Dwivedi/0266 88 Lap Open 212* 143 18 23.8 4.8* 8.8 Senagore/0261 71 Lap Open 109 101 1.6* 12.6 3.1* 6.8 Lawrence/0356 215 Lap Open 170** 140 9* 27 4.1** 9.0 *p<0.05**p<0.001
 Morbidity (%) Hospital stay (days) Bruce/ Lap Open 397** Liberman/9614 Lap Open ** 9.2 Coogan/ Lap Open Kholer/ Lap Open 165* * 14.3 Dwivedi/ Lap Open 212* * 8.8 Senagore/ Lap Open * * 6.8 Lawrence/ Lap Open 170** 140 9* ** 9.0 *p<0.05**p<")
28
Laparoscopy: Diverticulitis Obesity BMI No. of patients Age (yr: mean-range) Gender (M:F) Normal weight Group I 18.5-24.9 29 58.4 (37-78) 16:13 Overweight Group 2 25.0-29.927 55.2 (31-83) 14:13 Obese Group 3 30.0-39.921 54.1 (33-86) 14:13 Tuech et al. Surg Endosc 2001
 Gender (M:F) Normal weight Group I (37-78) 16:13 Overweight Group (31-83) 14:13 Obese Group (33-86) 14:13 Tuech et al. Surg Endosc")
29
Group 1 (n=29) Group 2 (n=27) Group 3 (n=21) ASA I 17138 ASA II 111210 ASA III 123 ASA IV 000 Tuech et al. Surg Endosc 2001 Laparoscopy: Diverticulitis Obesity

30
Reasons for conversion to laparotomy Group 1 (n=29) Group 2 (n=27) Group 3 (n=21) Severe adhesions 221 Unclear anatomy 021 Failure to liberate the splenic flexure 100 Obesity --- 1 Hemorrhage 100 Total n (%)4 (13.8)4 (14.8)3 (14.3) Tuech et al. Surg Endosc 2001

31
Laparoscopy: Diverticulitis Group 1 (n=29) Group 2 (n=27) Group 3 (n=21) Anastomotic leak (a) 101 Wound infection 223 Pulmonary infection 010 Postoperative ileus 100 Urinary infection 110 TOTAL (%) 5 (17.2) 4 (14.8) (b) 4 (19) (c) Tuech et al. Surg Endosc 2001 a. a.Anastomotic leak resolved with conservative drainage b. b.Group 1 vs. Group 2 – p=0.54 c. c.Group 1 vs. Group 3 – p=0.57

32
Laparoscopy: Diverticulitis Group 1 (n=29) Group 2 (n=27) Group 3 (n=21) Mean hospital stay (d) 8.2 8.5 (a) 9.8 (b) Inpatient rehabilitation 4/29 3/27 (c) 3/21 Tuech et al. Surg Endosc 2001 a. a.Hospital stay Group 1 vs. Group 2: p=0.31 b. b.Hospital stay Group 1 vs. Group 3: p=0.14 c. c.Inpatient rehabilitation Group 1 vs Group 2: p=0.54 d. d.Inpatient rehabilitation Group 1 vs Group 3: p=0.63

33
Laparoscopy: Diverticulitis > 54 patients- elective after > 2.2 (1-4) attacks > 5 (9.2%) converted > 3/5 (60%) for obesity > Surgery: 298 (180-480) minutes > 348 minutes in obese group versus 236 minutes in non-obese group (p 348 minutes in obese group versus 236 minutes in non-obese group (p<0.001) Smadja et al., Surg Endosc 1999
 attacks > 5 (9.2%) converted > 3/5 (60%) for obesity > Surgery: 298 ( ) minutes > 348 minutes in obese group versus 236 minutes in non-obese group (p 348 minutes in obese group versus 236 minutes in non-obese group (p<0.001) Smadja et al., Surg Endosc 1999")
34
Laparoscopy: Diverticulitis > Ileus: 2.3 (1-6) days > Hospitalization: 6.4 (4-15) days –2 (4.1%) early abdominal complications –4 (8.2%) abdominal wall complications –1 (2%) anastomotic stricture –1.8 (1-3) days use of Morphine Smadja et al., Surg Endosc 1999
 days > Hospitalization: 6.4 (4-15) days –2 (4.1%) early abdominal complications –4 (8.2%) abdominal wall complications –1 (2%) anastomotic stricture –1.8 (1-3) days use of Morphine Smadja et al., Surg Endosc 1999")
35
> 75 yrs < 75 yrs n= 22n = 63 Mean age (yrs)77.2 (75-82) 53.7 (38-74) Gender (M:F)10:1228:35 Operative time (min)234183 IV analgesia(days)5.45.2 Morbidity (%)1814 Mortality 00 Conversion (%)96 Hospitalization (days)*13.18.8 Teuch et al. Hepatogast 2001 * p=0.003 Laparoscopy: Elderly

36
Laparoscopic Open p value n= 22 n = 24 Mean age (yrs)77.2 (75-82) 78 (76-84) NS Gender (M:F)10:12 10:14 NS Operative time (min)234 136 NS IV analgesia(days)5.4 8.2 0.001 Morbidity (%)18 50 0.02 Mortality 0 0 NS Inpatient rehabilitation6 15 0.01 Hospitalization (days)13.1 20.2 0.003 Teuch et al. Surg Endosc 2000 Laparoscopy: Elderly

37
Laparoscopy: Diverticulitis > 65 patients - single surgeon > 60.1 (28-80) years old > 72.1 (53-97) kg weight > 2.4 (0-15) prior acute attacks > > 2 attacks in 41 (63.1%) patients > 1 attack in 20 patients > 3 patients - chronic disabling pain > 1 colovesicle fistula Siriser F, Surg Endosc 1999
 years old > 72.1 (53-97) kg weight > 2.4 (0-15) prior acute attacks > > 2 attacks in 41 (63.1%) patients > 1 attack in 20 patients > 3 patients - chronic disabling pain > 1 colovesicle fistula Siriser F, Surg Endosc 1999")
38
Laparoscopy: Diverticulitis > 179 (95-285) minutes surgery > 26 (40%) pericolic abscesses > 3 (4.6%) conversion - dense inflammatory adhesions in obesity > 9 (17.7%) morbidity - 2 (3.2%) reoperation > No deaths, No leaks > 7.6 (5-19) days in hospital > 11.8 days (+) complications vs. 6.7 days (-) > 2 reoperations for anastomotic stricture at 4 months > (+) 1 asymptomatic (endoscopic) stenosis Siriser F, Surg Endosc 1999
 > 2 reoperations for anastomotic stricture at 4 months > (+) 1 asymptomatic (endoscopic) stenosis Siriser F, Surg Endosc")
39
Laparoscopy: Diverticulitis 136 patients - 5 centers - 5 years > 71 females + 65 males > 61+11 (32-83) years old > 95% had acute infectious diverticulitis > 1 colovesical fistula > 18 (13%) conversions > 12 (67%) 2 o inflammatory adhesions > 173 (80-360) minutes Bokobza et al., Surg Endosc 1998
 years old > 95% had acute infectious diverticulitis > 1 colovesical fistula > 18 (13%) conversions > 12 (67%) 2 o inflammatory adhesions > 173 (80-360) minutes Bokobza et al., Surg Endosc 1998")
40
Laparoscopy: Diverticulitis > 2 (1.5%) postoperative adhesions > 27 (20%) complications > 1 (0.7%) anastomotic fistula > 13 (9.5%) abdominal wall hematoma or abscess > Successful –170+47 minutes –17% morbidity –0.58% mortality > Conversion –192+54 minutes –37% morbidity –5.6% mortality Bokobza et al., Surg Endosc 1998
 postoperative adhesions > 27 (20%) complications > 1 (0.7%) anastomotic fistula > 13 (9.5%) abdominal wall hematoma or abscess > Successful – minutes –17% morbidity –0.58% mortality > Conversion – minutes –37% morbidity –5.6% mortality Bokobza et al., Surg Endosc 1998")
41
Laparoscopy: Diverticulitis Factors predictive of conversion > Tumoral aspect 66% versus 41% > Tumoral aspect and chronic pain 44% versus 18% Conclusion: Need to preselect good candidates and convert early Bokobza et al., Surg Endosc 1998

42
Laparoscopy: Diverticulitis > 178 sigmoid colectomies > 70 chronic diverticulitis > 22 acute diverticulitis > 86 nondiverticular disease –77 neoplasia –5 rectal prolapse –4 other Schlacta et al., Surg Endosc 1999

43
Laparoscopy: Diverticulitis VariableAcuteChronicOther n227086 Conversions n (%)3(14)3 (4)17 (20) Median operative time (min)165150165 Morbidity n (%)1 (5)6 (9) 1 (1.5) Median full diet (days)334 Median discharge (days)655 Median normal activity (days)171517 (* p<0.05 other vs. chronic) Schlacta et al., Surg Endosc 1999
 Schlacta et al., Surg Endosc")
44
Laparoscopy: Complications > Prolonged operative time –150 to 255 minutes (p = 0.013) > Increased time to full diet –3.0 to 4.0 days (p < 0.001) > Delayed time to discharge –5.0 days to 9.0 days (p < 0.001) > But not time to normal activity –15 to 16 days Schlacta et al., Surg Endosc 1999
 > Increased time to full diet –3.0 to 4.0 days (p < 0.001) > Delayed time to discharge –5.0 days to 9.0 days (p < 0.001) > But not time to normal activity –15 to 16 days Schlacta et al., Surg Endosc 1999")
45
Laparoscopy: Diverticulitis > 110 patients - elective > 63 (36-83) years old > 9 (8.2%) conversion –adhesions, inflammation, obesity > 167 minutes mean operative time Berthou and Charboneau, Surg Endosc 1999
 years old > 9 (8.2%) conversion –adhesions, inflammation, obesity > 167 minutes mean operative time Berthou and Charboneau, Surg Endosc 1999")
46
Laparoscopy: Diverticulitis > 2.3 days ileus > 8.2 days hospitalization > No deaths > 7.3% morbidity including trocar site bowel incarceration and small bowel fistula Berthou and Charboneau, Surg Endosc 1999

47
Laparoscopy: Diverticulitis > Laparoscopic – facilitated feasible for “all forms” of “complicated” diverticular disease > Yields “marked” reductions in: –Operating time –Conversion rate –Operative and general costs Eijsbouts, et al. Surg Endosc 2000

48
Laparoscopy: Diverticulitis > Facilitated –Mobilization of sigmoid laparoscopically but “practically” no dissection of the “difficult” inflammatory process > Then through a Pfannenstiel incision: –Dissection of inflammatory process –Takedown fistula –Resection –Manual anastomosis Eijsbouts, et al. Surg Endosc 2000

49
Laparoscopy: Diverticulitis Costs Author/yearnSetting OR ($) Hospital ($) Hospital ($) Eijsbouts/00 Eijsbouts/003535 Lap assist Facilitated resection 1,6251,2508,1456,095 Bergamashi/004034 Intracoroporeal procedure (total) Lap assisted 3,0402,8209,25010,050
 Hospital ($) Hospital ($) Eijsbouts/00 Eijsbouts/ Lap assist Facilitated resection 1,6251,2508,1456,095 Bergamashi/ Intracoroporeal procedure (total) Lap assisted 3,0402,8209,25010,050")
50
Laparoscopy: Diverticulitis LaparoscopyLaparotomyp O.R charges ($) 10,5898,2070.05 Hospital cost ($) 11,50013,4000.29 Hospital charges ($) 29,98136,7450.11 Morbidity (%) 14140.11 Mortality 00 Liberman, Surg Endosc 1996
 10,5898, Hospital cost ($) 11,50013, Hospital charges ($) 29,98136, Morbidity (%) Mortality 00 Liberman, Surg Endosc 1996")
51
Costs: o pen vs. Laparoscopy Costs: o pen vs. Laparoscopy Author/yearnLap/OpenOR ($)Hospital ($) Bruce/9625 17 Lap Open ---10,230* 7,068 Liberman/9714 Lap Open 10,589* 8,207 11,528 13,426 Coogan/9727 34 Lap Open 15,200 7,200 17,000 15,800 Dwivedi/0266 88 Lap Open 9,566* 7,306 13,953 14,863 Senagore/0261 71 Lap Open 1,694* 1,426 3,458* a 4,321* Lawrence/0356 215 Lap Open ---17,414 25,700 *p<0.05 a = Total direct cost/case
Hospital ($) Bruce/ Lap Open ---10,230* 7,068 Liberman/9714 Lap Open 10,589* 8,207 11,528 13,426 Coogan/ Lap Open 15,200 7,200 17,000 15,800 Dwivedi/ Lap Open 9,566* 7,306 13,953 14,863 Senagore/ Lap Open 1,694* 1,426 3,458* a 4,321* Lawrence/ Lap Open ---17,414 25,700 *p<0.05 a = Total direct cost/case.")
52
Laparoscopy: Diverticulitis 18 patients- acute perforation Laparoscopic lavage and suction > + Omental patch closure > 7.5 days in hospital > 4-34 month follow-up > Subsequent elective resection with primary anastomosis possible Franklin et al., Surg Endosc 1997

53
Laparoscopy: Diverticulitis > 90% Success > Elective resection- 4-5 days in hospital > 5% Morbidity > Better than Laparotomy > Applicable in complex cases as well (Fistula, Abscess, Perforation) Franklin et al., Surg Endosc 1997
 Franklin et al., Surg Endosc 1997")
54
Laparoscopy: Diverticulitis > 8 patients - Generalized peritonitis > Laparoscopy + Lavage + Antibiotics > 5-8 days in hospital > 12-48 month follow-up > No recurrences > No resections O’Sullivan et al, Am J Surg 1996

55
Laparoscopy: Diverticulitis > 15 patients- Emergency > Generalized peritonitis > 2 o Perforated diverticulitis > Exploration + 10 litre lavage + “biological glue” + drainage > No stoma > 10 days antibiotics Montorsi et al, Surg Endosc 1998A

56
Laparoscopy: Diverticulitis > Zero mortality > 2 morbidity (lymphangitis, pulmonary) > 8 days hospitalization > 11 elective sigmoid colectomy at 3.5 months (10 successful laparoscopically) Montorsi et al, Surg Endosc 1998A
 > 8 days hospitalization > 11 elective sigmoid colectomy at 3.5 months (10 successful laparoscopically) Montorsi et al, Surg Endosc 1998A")
57
Laparoscopy: Diverticulitis > There is good evidence (Level 2) that laparoscopy for diverticulitis results in earlier discharge
 that laparoscopy for diverticulitis results in earlier discharge")
58
Laparoscopy: Diverticulitis > Despite longer operative time, the morbidity rate for the laparoscopic approach to diverticulitis in the most recent studies is equivalent or better than the open approach (Level 2 evidence)
")
59
Laparoscopy: Diverticulitis Conclusion > Elective laparoscopy for diverticular disease confers many advantages over the traditional approach > Based upon these data, laparoscopy is our preferred approach to the treatment of sigmoid diverticulitis

60
Rafferty et al, DCR 2006 Practice Parameters for Sigmoid Diverticulitis The Standards Committee of The American Society of Colon and Rectal Surgeons The laparoscopic approach is appropriate in selected patients. Level of Evidence III, Grade of Recommendation A Laparoscopic colectomy may have advantages over open laparotomy, including less pain, smaller scar, and shorter recovery. There is no increase in early or late complications. Cost and outcome are comparable to open resection. Laparoscopic surgery is acceptable in the elderly and seems to be safe in selected patients with complicated disease

Similar presentations





 NEJM,>")














