Download presentation
Presentation is loading. Please wait.

1
IL BONE-LOSS NELLA CHIRURGIA PROTESICA DI REVISIONE
PATOLOGIA DELL’ARTROSI COXOFEMORALE: IL BONE-LOSS NELLA CHIRURGIA PROTESICA DI REVISIONE Stefano Zanasi Policlinico di Monza IV Unità Operativa di Ortopedia Responsabile: Dr. Stefano Zanasi

2
STEFANO ZANASI

3
REVISION HIP ARTHROPLASTY
NEEDS TO RECOGNIZE BONE LOSS

4
REVISION HIP ARTHROPLASTY OF BONE-LOSS CLASSIFICATION
NEEDS OF BONE-LOSS CLASSIFICATION

5
BONE-LOSS CLASSIFICATION
PRE-OPERATIVE PLANNING COMMON LANGUAGE for REPORTING SURGICAL RESULTS ( A.A.O.S. COMMITEE ON THE HIP, 1993 )
")
6
BONE LOSS CLASSIFICATIONS
Engelbrecht ( 1987 ) Oakeshott et Coll. (1987) Gustilo-Pasternak (1988) Mallory et Coll. (1988) Engh et Coll. ( 1988 ) Schmitt et Coll. (1992) Tanzer et Coll. ( 1992 ) Pipino - Molfetta (1992) Gross et Coll. ( Paprosky et Coll. (1993) ° Chandler et Coll. (1989) D’Antonio et Coll. (1995)
 - Oakeshott et Coll. (1987) Gustilo-Pasternak (1988) - Mallory et Coll. (1988) Engh et Coll. ( 1988 ) - Schmitt et Coll. (1992) Tanzer et Coll. ( 1992 ) - Pipino - Molfetta (1992) Gross et Coll. ( Paprosky et Coll. (1993) ° Chandler et Coll. (1989) - D’Antonio et Coll. (1995)")
7
LIMITS of CLASSIFICATIONS
COMPLEXITY RELATED to IMAGING MANY CASES BORDERLINE INTRAOPERATIVE DEVELOPMENT OF BONE DEFECTS difficulty in application

8
in hip revision surgery
The BONE-LOSS CLASSIFICATION in hip revision surgery Italian Society of Revision Surgery-GIR

9
ACETABULAR BONE-LOSS GRADE I GRADE II GRADE III GRADE IV MASSIVE
° Loosening ° Enlargement and deformation of acetabulum GRADE IV ° Loosening ° Enlargement and deformation of acetabulum NO wall defect ° Loosening ° Enlargement and deformation of acetabulum MASSIVE and OVERALL Periacetab. Defect Defect in TWO- MORE walls Defect in ONE wall

10
FEMORAL BONE-LOSS GRADE I GRADE II GRADE III GRADE IV Defect
Proximal canal enlargement with cortical thinning NO cortical zone defect Proximal canal enlargement with cortical thinning Proximal canal enlargement with cortical thinning PROXIMAL CIRCUMFE- RENTIAL & MASSIVE Defect Defect in TWO or MORE zones Defect in ONE cortical zone

11
(Grade I – cavitary defect)
ACETABULAR BONE-LOSS (Grade I – cavitary defect) Host bone CAN CONTAIN the cup and ensure its stability. C.O.R. is not (or slightly) translated Loosening Enlargement and deformation of acetabulum NO WALL DEFECT
 Host bone CAN CONTAIN. the cup and ensure its. stability. C.O.R. is not (or slightly) translated. Loosening. Enlargement and. deformation of. acetabulum. NO WALL DEFECT.")
12
ACETABULAR BONE-LOSS FILLING of the cavity SURGICAL STRATEGY
(Grade I) FILLING of the cavity SURGICAL STRATEGY (Larger or elliptical cups, Cement, Bone chips, etc.)
 FILLING of the cavity. SURGICAL. STRATEGY. (Larger or elliptical cups, Cement, Bone chips, etc.)")
15
ACETABULAR BONE-LOSS (Grade II )
Loosening Enlargement and deformation of acetabulum Defect in ONE WALL Host bone MAY NOT CONTAIN the Cup C.O.R. always translated

16
(Rings, Cages, Conventional or Jambo cup, Bone grafts, etc.)
ACETABULAR BONE-LOSS (Grade II) RECONSTRUCTION of the DISRUPTED WALL (Rings, Cages, Conventional or Jambo cup, Bone grafts, etc.) SURGICAL STRATEGY
 RECONSTRUCTION. of the. DISRUPTED WALL. (Rings, Cages, Conventional or. Jambo cup, Bone grafts, etc.) SURGICAL. STRATEGY.")
23
b a c

25
ACETABULAR BONE-LOSS (Grade III) - Host bone CAN'T CONTAIN the CUP
- DEFECT of SUPPORTING WALL - ARTICULAR BIOMECHANICS ALTERED Loosening Enlargement and deformation of acetabulum Defect in TWO or MORE WALLS

26
CUP ANCHORAGE in intact bone
ACETABULAR BONE-LOSS (Grade III) CUP ANCHORAGE in intact bone ( Rings, Cages, Conventional or Jumbo cup, Stemmed cup, Oblong or asymetric cups, Morsellized bone grafts, etc. ) SURGICAL STRATEGY
 CUP ANCHORAGE. in intact bone. ( Rings, Cages, Conventional. or Jumbo cup, Stemmed cup, Oblong or asymetric cups, Morsellized bone grafts, etc. ) SURGICAL. STRATEGY.")
31
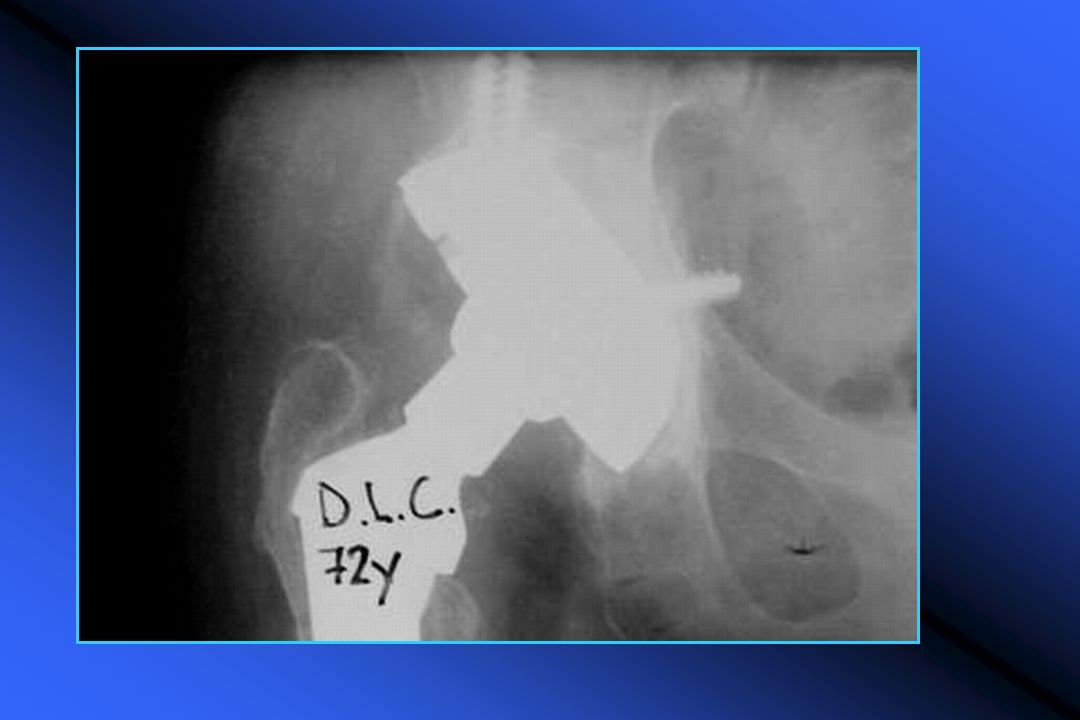
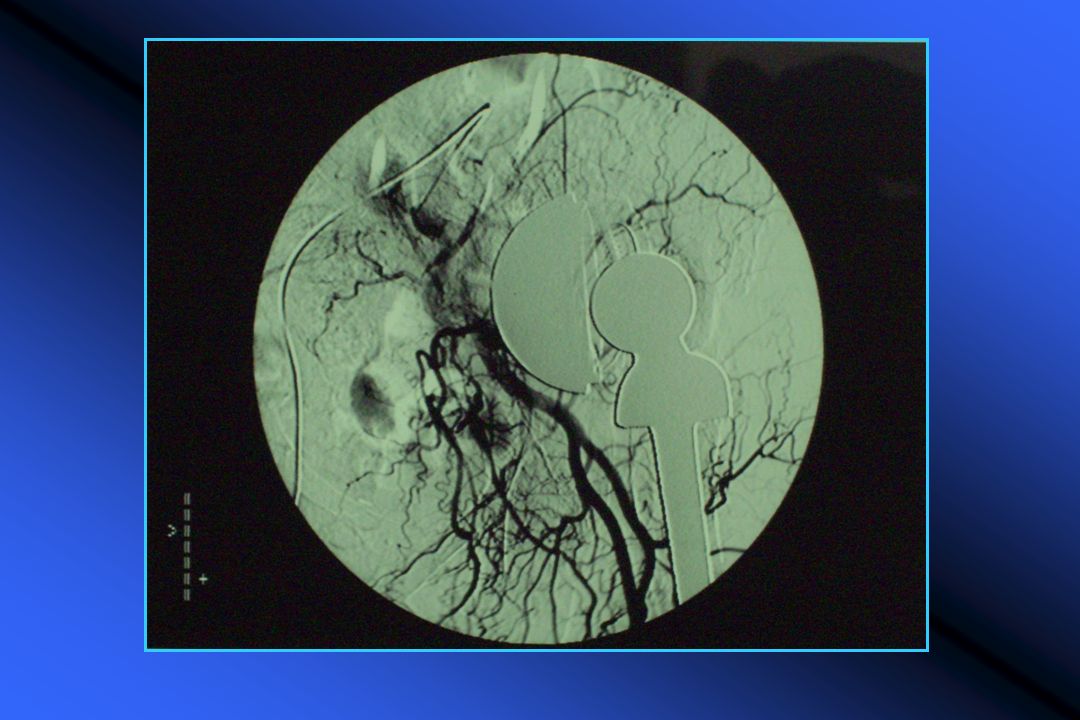
ACETABULAR BONE-LOSS Host bone CAN’T CONTAIN the cup Biomechanics is
(Grade IV) Host bone CAN’T CONTAIN the cup MASSIVE and OVERALL PERIACETABULAR Defects (hemipelvis fracture) Biomechanics is deeply altered
 Host bone. CAN’T CONTAIN. the cup. MASSIVE. and. OVERALL. PERIACETABULAR. Defects. (hemipelvis fracture) Biomechanics is. deeply altered.")
32
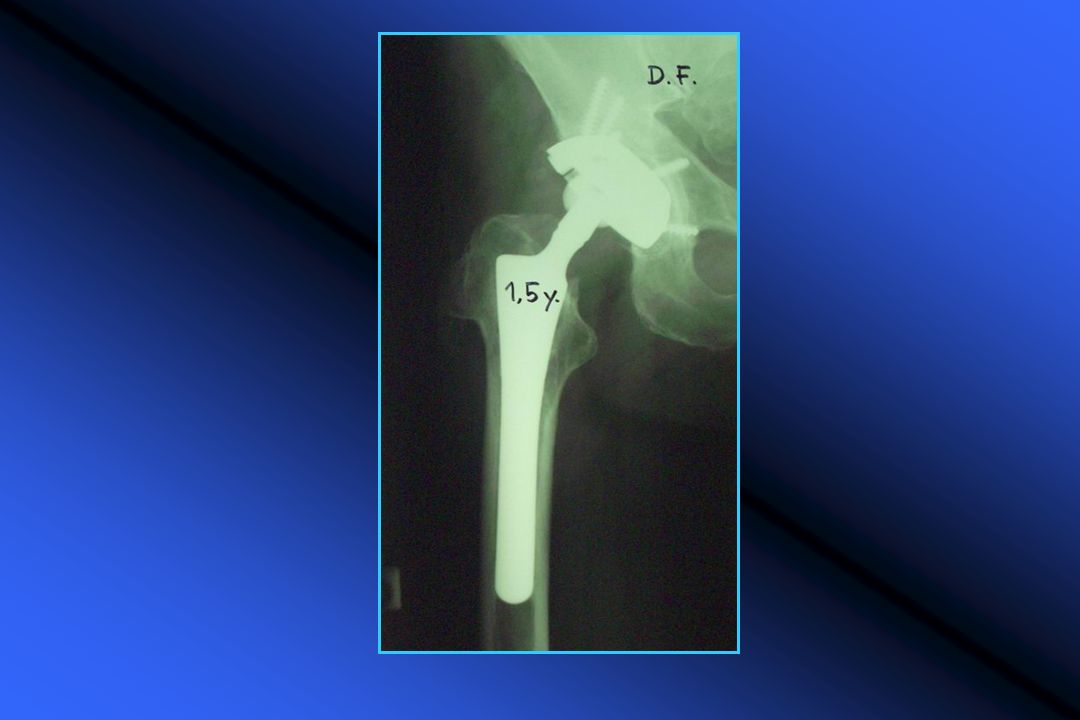
ANCHORAGE in the superior wall ACETABULAR BONE-LOSS (Grade IV)
SURGICAL STRATEGY (Rings, Cages, Stemmed cups, Allografts, etc. )
")
39
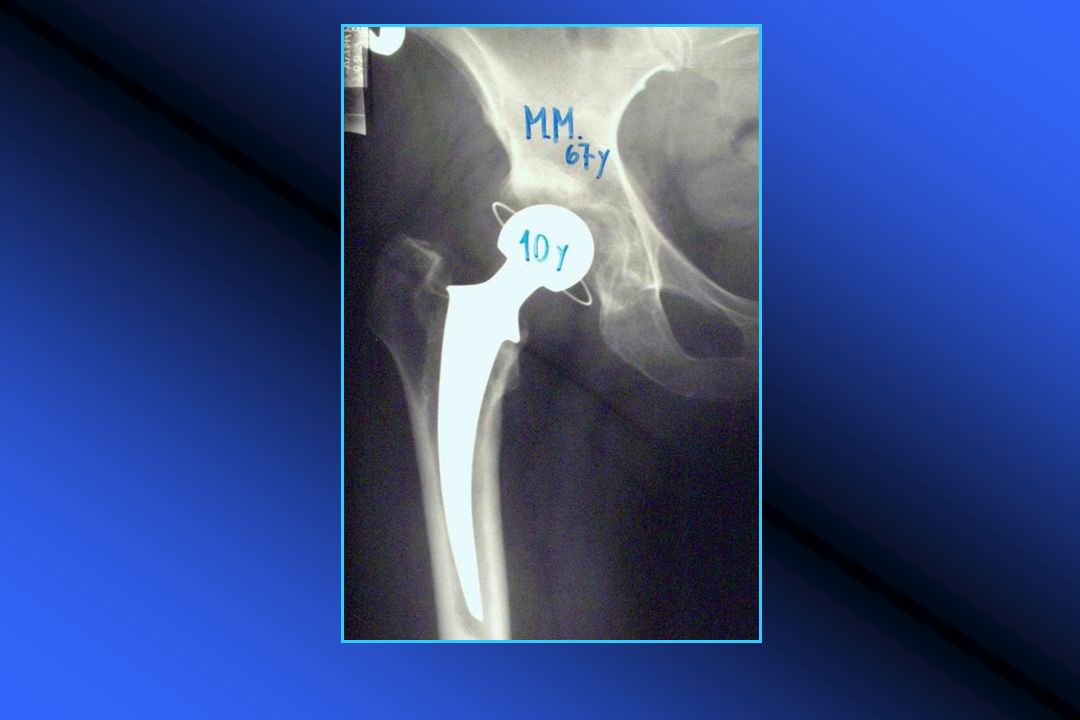
(Grade I – cavitay defect)
FEMORAL BONE-LOSS (Grade I – cavitay defect) Proximal canal enlargement with cortical thinning NO CORTICAL ZONE Defect PROXIMAL FEMUR CAN’T CONTAIN the stem Biomechanics is not altered ( leg length, muscle balance, head/neck offset )
 Proximal canal. enlargement. with cortical. thinning. NO CORTICAL. ZONE Defect. PROXIMAL FEMUR. CAN’T CONTAIN. the stem. Biomechanics is not altered. ( leg length, muscle balance, head/neck offset )")
40
FILLING of the femoral canal SURGICAL STRATEGY
FEMORAL BONE-LOSS (Grade I) FILLING of the femoral canal (larger and longer stem, cement, morsellized grafts, etc. Restoring the appropriate head-neck offset SURGICAL STRATEGY
 FILLING of the femoral canal. (larger and longer stem, cement, morsellized grafts, etc. Restoring the appropriate. head-neck offset. SURGICAL. STRATEGY.")
49
(Grade II – segmental defect)
FEMORAL BONE-LOSS (Grade II – segmental defect) Proximal femur MAY CONTAIN the stem and ensure its stability. Biomechanics is partially compromised Defect in ONE CORTICAL ZONE (Lesser trochanter, reabsorption, osteolysis, perforation, window, etc.)
 Proximal femur MAY. CONTAIN the stem. and ensure its stability. Biomechanics is. partially compromised. Defect in ONE. CORTICAL. ZONE. (Lesser trochanter, reabsorption, osteolysis, perforation, window, etc.)")
50
FEMORAL BONE-LOSS SURGICAL STRATEGY
(Grade II) RECONSTRUCTION of cortical defect (bone grafts, proximal anchorage with long stem, ev. cerclages ) Restoring the appropriate head/neck offset SURGICAL STRATEGY
 RECONSTRUCTION. of cortical defect. (bone grafts, proximal anchorage. with long stem, ev. cerclages ) Restoring the appropriate. head/neck offset. SURGICAL. STRATEGY.")
60
Proximal femur FEMORAL BONE-LOSS (Grade III) CAN'T CONTAIN and
STABILIZE the stem Biomechanical ability is significantly compromised Defect of TWO or MORE ZONES total PROXIMAL CIRCUNFERENTIAL defect

61
FEMORAL BONE-LOSS SURGICAL STRATEGY
(Grade III) ANCHORAGE in INTACT BONE (Below the defect) Modular or Custom-made stems Distal anchorage stems Massive allografts, SURGICAL STRATEGY
 ANCHORAGE in INTACT BONE. (Below the defect) Modular or Custom-made stems. Distal anchorage stems. Massive allografts, SURGICAL. STRATEGY.")
68
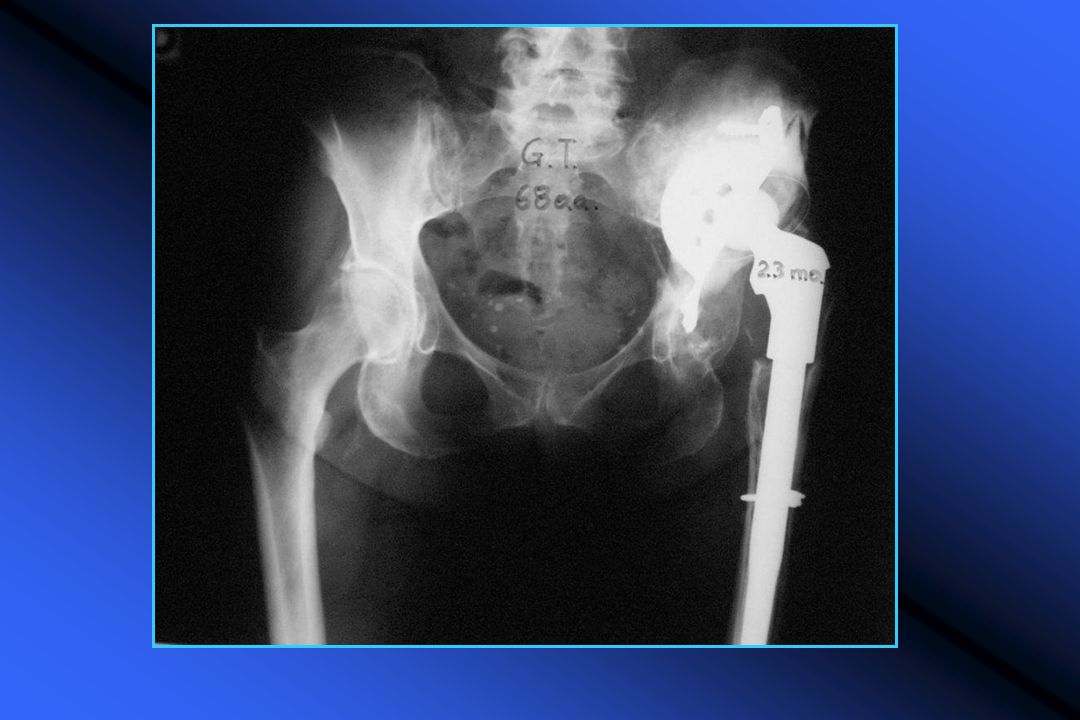
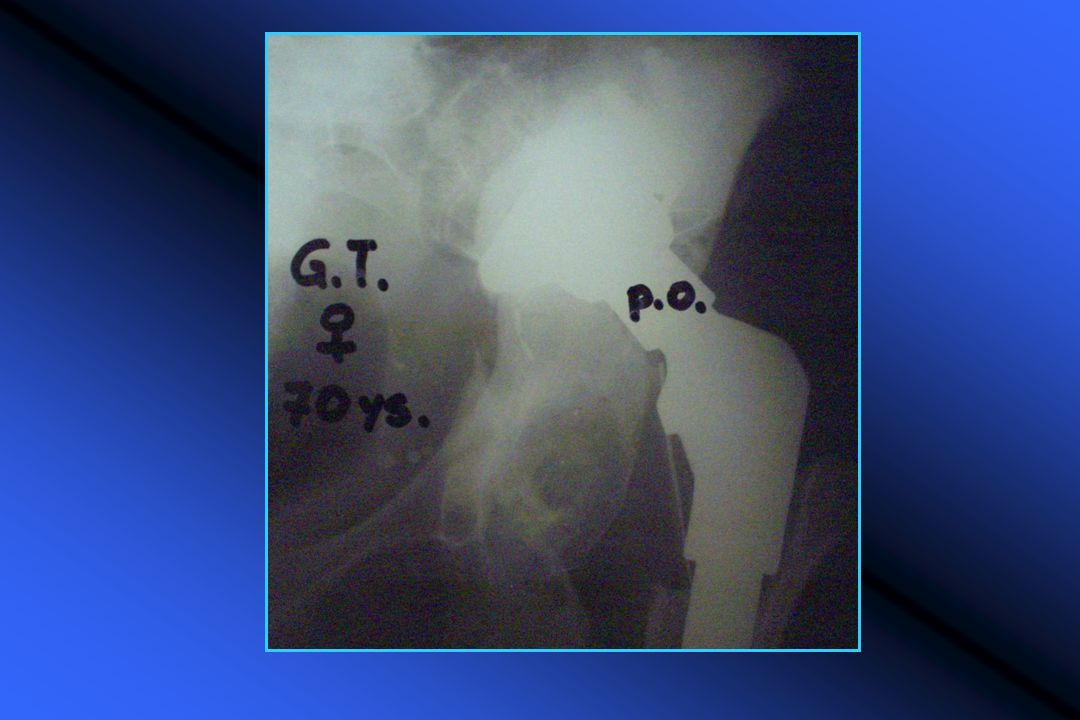
FEMORAL BONE-LOSS (Grade IV)
Proximal bone CAN’ T CONTAIN the stem Biomechanical ability is significantly compromized PROXIMAL CIRCUNFERENTIAL MASSIVE defect

69
FEMORAL BONE-LOSS (Grade IV) SURGICAL STRATEGY
ANCHORAGE the stem in distal bone SURGICAL STRATEGY Massive allografts, Distal anchorage stems, Modular stems (tumor prosth.)
")
74
Grazie

Similar presentations





















































 Trauma and post-traumatic arthritis Congenital deformities Bone tumors Avascular.>")


:1981-1987 November.>")




