Download presentation
Presentation is loading. Please wait.

1
Diagnosis, Management, & Follow-up Care Of CAD/AMI BARRY BERTOLET, MD CARDIOLOGY ASSOCIATES OF NORTH MS

2
What is coronary artery disease? A narrowing of the coronary arteries that prevents adequate blood supply to the heart muscle. Usually caused by atherosclerosis, it may progress to the point where the heart muscle is damaged due to lack of blood supply.

4
Presentations of CAD ▪ Method of diagnosis of the CAD depends on the presentation

5
Stable CAD Asymptomatic / Atypical ▪ CT calcium score ▪ Very sensitive ▪ Predictive of future events The BioImage Study. J Am Coll Cardiol. 2015; 65(11):1065-1074
:")
6
Stable CAD ▪ Symptoms - Angina ▪ Chest discomfort or tightness ▪ Jaw or arm discomfort ▪ Nausea ▪ Dyspnea ▪ Fatigue ▪ Back pain ▪ Severity of symptoms do not correlate with extent of CAD ▪ Usually symptoms denote at least one blockage > 50% ▪ Diagnostic tests ▪ Need a Functional Test FIRST ▪ Exercise Treadmill Stress Test ▪ With Imaging ▪ Echo ▪ Radionuclide ▪ Pharmacologic Stress Test with Imaging

7
Think about Radiation Exposure

8
Stable CAD – What do you do with a negative stress test?

9
▪ If in doubt, confirm dx of CAD with CT calcium score ▪ Begin cardiac risk factor modification ▪ Lower SBP to < 140 mm Hg ▪ Reduce LDL by 50% ▪ Smoking Cessation ▪ Exercise ▪ Weight control ▪ Mediterranean diet ▪ Angina control ▪ Beta-blockers ▪ Calcium channel blockers ▪ Nitrates ▪ Ranexa ▪ BB / amlodipine combo >> diltiazem / nitrate combo ▪ What about Aspirin?

10
Stable CAD – What do you do with a negative stress test? ▪ If in doubt, confirm dx of CAD with CT calcium score ▪ Begin cardiac risk factor modification ▪ Lower SBP to < 140 mm Hg ▪ Reduce LDL by 50% ▪ Smoking Cessation ▪ Exercise ▪ Weight control ▪ Mediterranean diet ▪ Angina control ▪ Beta-blockers ▪ Calcium channel blockers ▪ Nitrates ▪ Ranexa ▪ BB / amlodipine combo >> diltiazem / nitrate combo ▪ What about Aspirin? ▪ Only women who are at high risk for MI or CVA should be prescribed ASA ▪ ASA is recommended in men, especially those > 45 years.

11
New Lipid Guidelines

12
When to Cath in Stable Angina ▪ Symptoms despite therapy ▪ Abnormal functional test ▪ Unsure diagnosis ▪ High probability / high risk ▪ Hx stents, CABG, etc. ▪ Change in ECG Radial Heart Cath / PCI ▪ Lower risk ▪ More convenient for patients

13
PCI for Stable Angina Courage Trial ▪ Everyone got a cath first to exclude left main or serious 3 vessel CAD ▪ Large number of medically only treated patients crossed over to PCI due to inadequate angina control ▪ Once serious CAD is excluded in stable angina patients, ▪ PCI does not prevent MI ▪ PCI does not extend life

14
Unstable CAD ▪ Diagnostic test of choice: ECG ▪ If ECG is negative, check the cardiac troponin level

15
STEMI ▪ Must check ECG within 10 mins of presentation ▪ Dx: Symptoms + ST elevation ▪ Must get into cath lab within 90 mins or 120 mins if a transfer patient ▪ This includes “Inpatients” ▪ Upfront Meds ▪ ASA 325 mg ▪ Heparin ▪ UFH 4000 units ▪ Lovenox 30 mg IV ▪ ? Thienopyridine ▪ ? 2B/3A inhibitor bolus ▪ No clear benefit of routine upfront beta-blockers and nitrates

16
Time Is Muscle The Wavefront of Necrosis

17
Acute MI Stent Therapy

18
Unstable CAD – Non STEMI Why would NSTEMI be more likely to die? ▪ Treat as aggressive as you do with STEMI!

19
Unstable CAD

20
Unstable CAD – What’s next in unstable angina ▪ TIMI – 0 ▪ Evaluate for non-cardiac chest pain ▪ TIMI – 1 or 2 ▪ Consider stress test ▪ Risk factor modification ▪ Medical therapy for CAD ▪ TIMI – 3 or more ▪ Consider cath ▪ Risk factor modification ▪ Medical therapy for CAD

21
Follow-up Care ▪ Things You Need to Know First ▪ Did the patient have unstable CAD? ▪ Did the patient have a DES? ▪ Is the patient diabetic? ▪ What is the LVEF? ▪ What is the baseline LDL? ▪ Did the patient have unstable CAD – regardless of initial tx? ▪ Needs DAPT for 9 months ▪ Brilinta or Effient preferred over Plavix

22
Follow-up Care ▪ Things You Need to Know First ▪ Did the patient have unstable CAD? ▪ Did the patient have a DES? ▪ Is the patient diabetic? ▪ What is the LVEF? ▪ What is the baseline LDL? ▪ Did the patient have unstable CAD – regardless of initial tx? ▪ Needs beta-blocker therapy for at least 12 months (preferably 24 months)
.")
23
Follow-up Care ▪ Things You Need to Know First ▪ Did the patient have unstable CAD? ▪ Did the patient have a DES? ▪ Is the patient diabetic? ▪ What is the LVEF? ▪ What is the baseline LDL? ▪ Did the patient have a drug- eluting stent? ▪ Needs DAPT for 12 months ▪ Brilinta or Effient preferred in unstable CAD presentations ▪ Plavix is OK in stable presentations ▪ What about bare metal stents? ▪ DAPT is needed for 6 – 12 weeks.

24
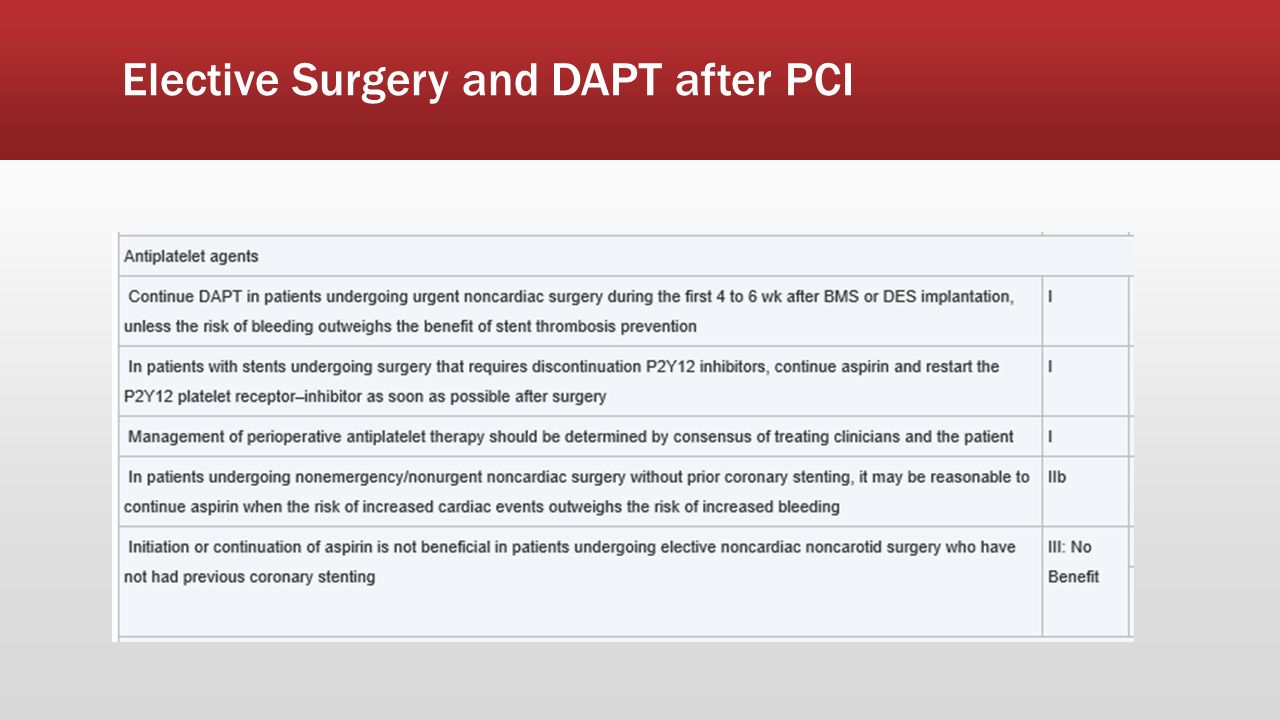
Elective Surgery and DAPT after PCI

26
Follow-up Care ▪ Things You Need to Know First ▪ Did the patient have unstable CAD? ▪ Did the patient have a DES? ▪ Is the patient diabetic? ▪ What is the LVEF? ▪ What is the baseline LDL? ▪ Is the patient diabetic? ▪ If unstable presentation, requires aldactone 12.5 mg – 25 mg daily ▪ Can raise potassium levels and cause sore breasts in men

27
Follow-up Care ▪ Things You Need to Know First ▪ Did the patient have unstable CAD? ▪ Did the patient have a DES? ▪ Is the patient diabetic? ▪ What is the LVEF? ▪ What is the baseline LDL? ▪ What is the LVEF? ▪ < 35% ▪ CHF approved beta-blocker ▪ Carvedilol ▪ Toprol XL ▪ Bisoprolol ▪ ACE or ARB ▪ Aldactone

28
Follow-up Care ▪ Things You Need to Know First ▪ Did the patient have unstable CAD? ▪ Did the patient have a DES? ▪ Is the patient diabetic? ▪ What is the LVEF? ▪ What is the baseline LDL? ▪ With CAD, need a > 50% reduction in LDL

29
PCSK9 -- What is it?

30
What do PCSK9 inhibitors do…

31
How do you give it?

32
Follow-Up Studies ▪ ECG ▪ LBBB ▪ Arrhythmias ▪ BMP within 2-4 weeks of aldactone start ▪ VerifyNow in Plavix users ▪ LDL in 8 weeks to confirm > 50% reduction from baseline; repeat again for med changes ▪ For newly recognized LVEF < 35%, repeat echo in 90 days, and then annually ▪ For LVEF < 35% after 90 days, consider ICD ▪ For “high risk” patients post stent implantation, consider stress test at year one

33
Follow-Up Studies - Symptoms ▪ ECG ▪ Is there a change? ▪ Echo ▪ Is there a new WMA? ▪ Is there a change in LVEF? ▪ Stress test ▪ Lab ▪ Hemogram ▪ BMP ▪ ? TSH ▪ When to order CTA… ▪ Early symptoms after CABG ▪ Inconclusive stress test ▪ Negative stress test and persistent symptoms ▪ Suspicion for coronary anomaly

34
Follow-Up Studies - Symptoms ▪ When to order cardiac cath… ▪ Early symptoms after CABG or stent implantation ▪ Abnormal or Inconclusive stress test ▪ Negative stress test and persistent symptoms ▪ Concern for unstable angina

35
Thanks for listening!

Similar presentations












 Why myocardial ischaemia occurs? Myocardial Ischaemia occurs when there is less supply of oxygen to the.>")



 CAD is most common form of heart disease and causes premature death. In UK, 1 in 3 men and.>")



