Download presentation
Presentation is loading. Please wait.

1
Which is the role of post-dilation after DES implantation? Enrico Romagnoli 1,2 M.D., Ph.D. 1 Policlinico Casilino, Roma 2 Opedale San Raffaele, Milano

2
Optimization of stent deployment during percutaneous coronary intervention (PCI) is a key element to obtain most favorable immediate and long-term results. Basic principle of stent-based PCI The bigger = The better

3
Bigger stent expansion = better outcome Intracoronary stenting without anticoagulation accomplished with intravascular ultrasound guidance. Circulation 1995;15;91:1676–88. Colombo A, et al. Intracoronary stenting without anticoagulation accomplished with intravascular ultrasound guidance. Circulation 1995;15;91:1676–88. Conclusions : the Palmaz-Schatz stent can be safely inserted in coronary arteries without subsequent anticoagulation provided that stent expansion is adequate. High-pressure final balloon dilatations (14.9 ± 3.0 atm) and confirmation of adequate stent expansion by intravascular ultrasound provide assurance that anticoagulation therapy can be safely omitted. This technique significantly reduces hospital time and vascular complications and has a low stent thrombosis rate (1.6%).
 and confirmation of adequate stent expansion by intravascular ultrasound provide assurance that anticoagulation therapy can be safely omitted. This technique significantly reduces hospital time and vascular complications and has a low stent thrombosis rate (1.6%)..")
4
Bigger DES expansion = better outcome? After the introduction of drug-eluting stents (DES), the importance of optimal stent deployment was initially underestimated, leading to less use of high pressure deployment and/or balloon post-dilation.
, the importance of optimal stent deployment was initially underestimated, leading to less use of high pressure deployment and/or balloon post-dilation..")
5
Conclusion: SES had a considerably lower optimal MSA threshold compared to BMS Bigger DES expansion = better outcome? Cypher Bx Velocity Sonoda S, et al. J Am Coll Cardiol 2004

6
Hoffmann R,et al. Catheter Cardiovasc Interv 2005 A comparison study between SIRIUS-US (pre- and post- dilation) and E-SIRIUS (direct stenting and non mandatory post-dilation) IVUS results showed that, although the less aggressive stent implantation in E-SIRIUS resulted in a relatively lower stent expansion, no detrimental effects were observed in major adverse cardiac events. Bigger DES expansion = better outcome?
 and E-SIRIUS (direct stenting and non mandatory post-dilation) IVUS results showed that, although the less aggressive stent implantation in E-SIRIUS resulted in a relatively lower stent expansion, no detrimental effects were observed in major adverse cardiac events. Bigger DES expansion = better outcome .")
7
= edge restenosis Sakurai R, et al. Am J Cardiol 2005

8
Bigger DES expansion = better outcome? Sakurai R, et al. Am J Cardiol 2005 = edge restenosis

9
Magnitude of suboptimal stent expansion Because stent under-expansion is poorly recognized by angiography, the real incidence of suboptimal stent deployment is likely to be underestimated.

10
Before post-dilationAfter post-dilation

11
Determinants of Suboptimal Stent Deployment 1. Stent undersizing (balloon to artery ratio <1) : (certainly the first and the most important) (certainly the first and the most important) severe and diffuse target vessel; small vessel; acute coronary syndrome; severe stenosis; direct stenting. In case of undersizing of the stent delivery balloon, high- pressure deployment can compensate for the balloon undersizing only in part!
 : (certainly the first and the most important) (certainly the first and the most important) severe and diffuse target vessel; small vessel; acute coronary syndrome; severe stenosis; direct stenting. In case of undersizing of the stent delivery balloon, high- pressure deployment can compensate for the balloon undersizing only in part!.")
12
Determinants of Suboptimal Stent Deployment 2. : 2. Balloon compliance and pressure deployment : (the most unknown) (the most unknown) Stent manufacturers provide a compliance chart relating balloon deployment pressure and the stent diameter based on in vitro measurement (in air or in water). Several IVUS studies found that the real MSD after stent deployment was 20-26% less than the unconstrained stent size displayed in the compliance chart on the stent box. These differences were independent of stent manufacturer, length, diameter, and deployment pressure and related to the inherent resistance of dilating stent within an atherosclerotic artery.
 (the most unknown) Stent manufacturers provide a compliance chart relating balloon deployment pressure and the stent diameter based on in vitro measurement (in air or in water). Several IVUS studies found that the real MSD after stent deployment was 20-26% less than the unconstrained stent size displayed in the compliance chart on the stent box. These differences were independent of stent manufacturer, length, diameter, and deployment pressure and related to the inherent resistance of dilating stent within an atherosclerotic artery..")
13
Intravascular ultrasound assessment of drug-eluting stent expansion De Ribamar Costa Am Heart J 2007 According to the compliance chart, DES achieved 75% ± 10% of predicted MSD66% ± 17% of predicted MSA 24% of SES and 28% of PES did not achieve a final MSA of 5 mm2

14
Intravascular ultrasound assessment of drug-eluting stent expansion De Ribamar Costa Am Heart J. 2007 no significant difference in stent expansion between DES and their BMS equivalent

15
Determinants of Suboptimal Stent Deployment 3. Plaque and vessel compliance : (the most unpredictable) (the most unpredictable) In IVUS studies, arterial expansion seemed to be the primary mechanism of lumen enlargement after stenting, accounting for approximately 70% of luminal gain, whereas the relative contribution of plaque reduction ranged between 6% and 34%. Causes of impaired compliance: vessel fibrosis calcium high plaque burden previous stent implantation Boschat J et al. Int J Cardiovasc Imaging 2002
 (the most unpredictable) In IVUS studies, arterial expansion seemed to be the primary mechanism of lumen enlargement after stenting, accounting for approximately 70% of luminal gain, whereas the relative contribution of plaque reduction ranged between 6% and 34%. Causes of impaired compliance: vessel fibrosis calcium high plaque burden previous stent implantation Boschat J et al. Int J Cardiovasc Imaging")
16
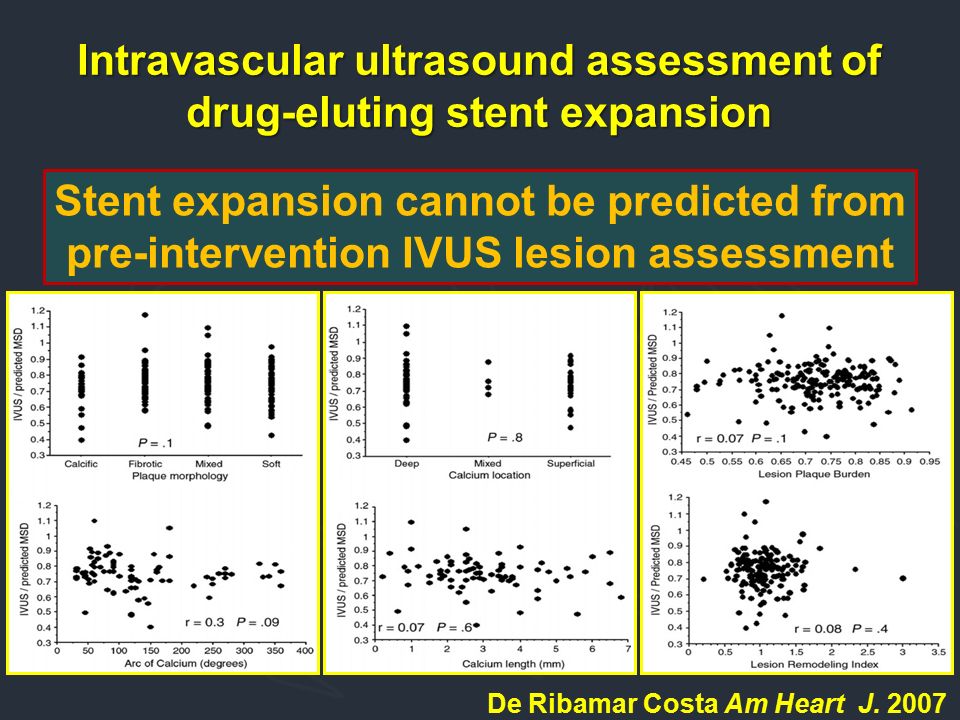
Intravascular ultrasound assessment of drug-eluting stent expansion Stent expansion cannot be predicted from pre-intervention IVUS lesion assessment De Ribamar Costa Am Heart J. 2007
17
Determinants of Suboptimal Stent Deployment 3. Plaque and vessel compliance : high plaque burden Yoon Sc, et al. Catheter Cardiovasc Interv. 2002 IVUS success rate % 67.6% 45.7%

18
Determinants of Suboptimal Stent Deployment 3. Plaque and vessel compliance : Calcium Calcium Stent symmetry index P = 0.001 Albrecht D, et al. Cathet Cardiovasc Diagn 1996 minimal/maximal stent diameter

19
Determinants of Suboptimal Stent Deployment 3. Plaque and vessel compliance : Calcium Calcium Vavuranakis M, et al. Cathet Cardiovasc Intervent 2001 Baseline Stent 16 atm Stent at 20 atm

20
Determinants of Suboptimal Stent Deployment 4. Lesion characteristics : (certainly the most predictable) (certainly the most predictable) Specific lesion subsets are associated with a lower success rate and required more care and tools to obtain an optimal stent deployment Specific lesion subsets are associated with a lower success rate and required more care and tools to obtain an optimal stent deployment: bifurcation lesion (side branch ostium, kissing balloon); ostial lesion (fibrosis) long lesion (proximal-distal vessel size mismatch, overlap) small vessel (vessel overstretch) in stent restenosis
 (certainly the most predictable) Specific lesion subsets are associated with a lower success rate and required more care and tools to obtain an optimal stent deployment Specific lesion subsets are associated with a lower success rate and required more care and tools to obtain an optimal stent deployment: bifurcation lesion (side branch ostium, kissing balloon); ostial lesion (fibrosis) long lesion (proximal-distal vessel size mismatch, overlap) small vessel (vessel overstretch) in stent restenosis.")
21
For these causes, the use of a noncompliant balloon post-dilation represents a good compromise to achieve good stent expansion and symmetry without increasing risk of dissection or rupture of the vessel. Determinants of Suboptimal Stent Deployment 1. Stent undersizing (balloon to artery ratio <1) 2. Balloon compliance and pressure deployment 3. Plaque and vessel compliance 4. Lesion characteristics
 2. Balloon compliance and pressure deployment 3. Plaque and vessel compliance 4. Lesion characteristics.")
22
High pressure stent deployment vs. non-compliant balloon postdilation High pressure stent deployment vs. non-compliant balloon postdilation Bermejo J, et al. Circulation 1998 Despite high-pressure deployment, lumen dimensions after stenting are only 57% of maximal achievable. Inadequate balloon expansion and elastic recoil are responsible for residual lumen stenosis

23
High pressure stent deployment vs. non-compliant balloon postdilation High pressure stent deployment vs. non-compliant balloon postdilation Jose de Ribamar Costa et al, American Heart Journal 2007 Post-dilation with the stent balloon is not sufficient

24
Mean Minimum Stent CSA According to Post-dilation Balloon Size Mean Minimum Stent CSA According to Post-dilation Balloon Size 2.53.03.54.0 0 5 10 15 Balloon Size (mm) IVUS Derived Final stent CSA (mm 2 )
 IVUS Derived Final stent CSA (mm 2 )")
25
Seung-Ho Hur. Am J Cardiol 2001 Efficacy of Post-deployment Balloon Dilatation for Bare Metal Stents as Assessed by Intravascular Ultrasound Minimal stent area P <0.001 Stent volume index 6.4 7.4 6.6 7.5 P <0.001

26
Efficacy of Post-deployment Balloon Dilation for Bare Metal Stents as Assessed by Intravascular Ultrasound

27
Seung-Ho Hur. Am J Cardiol 2001 Stent CSA / reference CSA After stent deployment (stent/vessel ratio 1.1) After non compliant post dilation (balloon vessel/ratio 1.1) Efficacy of Post-deployment Balloon Dilation for Bare Metal Stents as Assessed by Intravascular Ultrasound
 After non compliant post dilation (balloon vessel/ratio 1.1) Efficacy of Post-deployment Balloon Dilation for Bare Metal Stents as Assessed by Intravascular Ultrasound.")
28
POST-IT Trial protocol Brodie BR, et al. Catheter Cardiovasc Interv 2003 Lesion predilation YesNo Stenting with delivery balloon (ballon/vessel ratio 1.1) IVUS assessment IVUS criteria for optimum stent deployment met? Post-dilate with NC balloon (ballon/vessel ratio 1.1) IVUS assessment IVUS criteria for optimum stent deployment met?Yes Procedure end
 IVUS assessment IVUS criteria for optimum stent deployment met. Post-dilate with NC balloon (ballon/vessel ratio 1.1) IVUS assessment IVUS criteria for optimum stent deployment met Yes Procedure end.")
29
High pressure stent deployment vs. non-compliant balloon postdilation High pressure stent deployment vs. non-compliant balloon postdilation Brodie BR, et al. Catheter Cardiovasc Interv 2003 21% 42% 6,6% 7,8% P < 0.01 MUSIC criteria satisfied MSA

30
High pressure stent deployment vs. non-compliant balloon postdilation High pressure stent deployment vs. non-compliant balloon postdilation Brodie BR, et al. Catheter Cardiovasc Interv 2003 MSD 2.2MSD 2.5 3.0 x 18 mm stent delivery balloon at 14 atm 3.0 x 15 mm non-compliant balloon at 14 atm

31
Risk of “dog bone”/edge effect with an SC balloon at high pressure NC balloon at high pressure Semi Compliant Non Compliant Semi-compliant vs. non-compliant balloon

32
Non compliant balloon Quantum 4.0 x 15 mm Standard stent delivery balloon 4.0 x 16 mm

33
Pre-Optimization Post-Optimization High pressure stent deployment vs. non-compliant balloon postdilation High pressure stent deployment vs. non-compliant balloon postdilation Avoid the Donkey effect!

34
Benefits of a NC balloon post-dilation after DES implantation Benefits of a NC balloon post-dilation after DES implantation In-stent restenosis: complete stent struts apposition; higher luminal MSA (<5 mm 2 threshold); stent symmetry (homogeneous drug release) Observational data suggest that stent under-expansion might be one of the most important causes of DES failure, advocating that, once neo-intimal hyperplasia is suppressed, the optimum stent deployment is still fundamental
; stent symmetry (homogeneous drug release) Observational data suggest that stent under-expansion might be one of the most important causes of DES failure, advocating that, once neo-intimal hyperplasia is suppressed, the optimum stent deployment is still fundamental")
35
Under deployment is a cause for In-Stent Restenosis 20% Castagna MT, et al. American Heart Journal 2001 Results from a retrospective study of 1.090 patients

36
Benefits of a NC balloon post-dilation after DES implantation Benefits of a NC balloon post-dilation after DES implantation Stent thrombosis (0.4%-0.6% of RCT up to 1.3-4.9 of registry) complete stent struts apposition; stent underexpansion (shear stress); reduced edge dissection shorter dual antiplatelet therapy In this view, the less care used by operators to obtain an optimal stent deployment and a lower use of post- dilation might represent a possible explanation of the higher rates of stent thrombosis observed with DES
 complete stent struts apposition; stent underexpansion (shear stress); reduced edge dissection shorter dual antiplatelet therapy In this view, the less care used by operators to obtain an optimal stent deployment and a lower use of post- dilation might represent a possible explanation of the higher rates of stent thrombosis observed with DES")
37
Under deployment is the main cause for subacute thrombosis 78% Cheneau E, et al. Circulation. 2003 Results from 7484 consecutive patients without acute MI

38
Stent underexpansion is an independent predictor of subacute stent thrombosis 4.3 +/- 1.6 6.2 +/- 1.9 Minimum stent CSA Stent expansion Stent thrombosis group (SES) Matched control group (SES) vs. 0.65 +/- 0.18 0.85 +/- 0.14 Fujii, K, et al. Journal of the American College of Cardiology 2005 p < 0.001

39
How to select and post-dilate with an non-compliant balloon Angiograph y-guided strategy Select a non- compliant balloon Shorter than the stent 0.50 mm larger than the stent delivery balloon Deploy at gradual high pressures i.e. >24 atm

40
ConclusionsConclusions Which is the role of post-dilation after DES implantation? In clinical practice, a considerable number of patients might benefit from repeat inflations with non-compliant balloons at higher pressures and/or with larger diameter size. Data from the literature suggest that achieving adequate stent expansion during PCI is important to reduce restenosis and the need for TVR, but it might also minimize the risk of stent thrombosis in the DES era.

41
N None of the baseline clinical or angiographic variables seemed able to predict the final MSA or MSD after stenting. Similarly, neither quantitative IVUS lesion measurements nor qualitative IVUS assessment of plaque morphology could predict stent expansion. These observations would suggest that the impact of plaque and vessel compliance on the final stent expansion can be limited by an appropriate use of post-dilation. ConclusionsConclusions Which is the role of post-dilation after DES implantation?

42
Although there are not enough randomized data to support its use, it seems wise to perform post-dilation with non- compliant balloons at high pressures in the majority of patients undergoing both BMS and DES implantation. Although there are not enough randomized data to support its use, it seems wise to perform post-dilation with non- compliant balloons at high pressures in the majority of patients undergoing both BMS and DES implantation. Particularly in IVUS-guided procedures, the recommended strategy to achieve an optimal stent deployment should be to select a noncompliant balloon whose size matches the media-to-media IVUS measurement. Particularly in IVUS-guided procedures, the recommended strategy to achieve an optimal stent deployment should be to select a noncompliant balloon whose size matches the media-to-media IVUS measurement. ConclusionsConclusions Which is the role of post-dilation after DES implantation?

43
Reference: Romagnoli et al. JACC intv. 2008;1:45-56 Romagnoli et al. JACC intv. 2008;1:45-56Romagnoli et al. JACC intv. 2008;1:45-56 Slides available at: www. metcardio.org www. metcardio.orgwww. metcardio.org Which is the role of post-dilation after DES implantation? Enrico Romagnoli 1,2 M.D., Ph.D.

Similar presentations








 study with the Sirolimus coated BX™ VElocity balloon expandable stent (CYPHER™)>")










