Download presentation
Presentation is loading. Please wait.

1
Hematology Oncology Board Review Anas Sawas

2
Blood Transfusion Reactions Febrile Non-Hemolytic Transfusion Reaction (FNHTR) Simple Allergic (Urticarial) Reaction Acute Hemolytic Transfusion Reaction (AHTR) Transfusion Associated Sepsis Severe Allergic (Anaphylactic) Reaction Transfusion Related Acute Lung Injury (TRALI) Transfusion-Associated Circulatory Overload (TACO)
 Simple Allergic (Urticarial) Reaction Acute Hemolytic Transfusion Reaction (AHTR) Transfusion Associated Sepsis Severe Allergic (Anaphylactic) Reaction Transfusion Related Acute Lung Injury (TRALI) Transfusion-Associated Circulatory Overload (TACO)")
3
Febrile Non-Hemolytic Transfusion Reaction (FNHTR) Patient receiving blood transfusion develops chills or fever (<1 C increase) Occurs during or up to 4 hours after Incidence: 1:500 Pathophysiology: Cytokine mediated Treatment: Stop transfusion while continuing to give patient normal saline Acetaminophen Resume transfusion if patient symptoms subside while observing patient for 15-30 min
 Patient receiving blood transfusion develops chills or fever (<1 C increase) Occurs during or up to 4 hours after Incidence: 1:500 Pathophysiology: Cytokine mediated Treatment: Stop transfusion while continuing to give patient normal saline Acetaminophen Resume transfusion if patient symptoms subside while observing patient for min")
4
Simple Allergic (Urticarial) Reaction Occurs during or a few hours after Incidence: 1:3 – 1:300 ONLY transfusion reaction where if mild you can continue transfusion Pathophysiology: antigen-antibody interaction Treatment: Diphenhydramine
 Reaction Occurs during or a few hours after Incidence: 1:3 – 1:300 ONLY transfusion reaction where if mild you can continue transfusion Pathophysiology: antigen-antibody interaction Treatment: Diphenhydramine")
5
Acute Hemolytic Transfusion Reaction (AHTR) Life-threatening reaction caused by acute intravascular hemolysis of transfused RBCs can lead to DIC/ARF/ Shock Incidence: 1:38,000 – 1:70,000 and Mortality: 1:30 Usually due to ABO incompatibility often caused by a clerical error Symptoms: fever, chills, flank pain, and oozing from intravenous sites Diagnosis: Pink Plasma, Coombs Test Treatment: STOP Transfusion Aggressive hydration Notify Blood Bank Send labs: Chem, Hg/Hct, Blood Type and screen, Coombs test
 Life-threatening reaction caused by acute intravascular hemolysis of transfused RBCs can lead to DIC/ARF/ Shock Incidence: 1:38,000 – 1:70,000 and Mortality: 1:30 Usually due to ABO incompatibility often caused by a clerical error Symptoms: fever, chills, flank pain, and oozing from intravenous sites Diagnosis: Pink Plasma, Coombs Test Treatment: STOP Transfusion Aggressive hydration Notify Blood Bank Send labs: Chem, Hg/Hct, Blood Type and screen, Coombs test")
6
Transfusion Associated Sepsis Occur in first hour of transfusion and is Rare Caused by transfusion of a product that contains a microorganism and endotoxin Symptoms: fever, chills, and hypotension. Treatment: STOP transfusion Notify blood bank Culture blood (recipient and donor) Broad spectrum antibiotics Fluids and Pressors if needed
 Broad spectrum antibiotics Fluids and Pressors if needed.")
7
Severe Allergic (Anaphylactic) Reaction Occur at the start of the transfusion and up to 4 hrs following the transfusion Incidence: 1:20000- 1:50000 Presentation: angioedema, wheezing, respiratory distress and/or hypotension Treatment: STOP Transfusion Supportive Care and Airway management Epinephrine
 Reaction Occur at the start of the transfusion and up to 4 hrs following the transfusion Incidence: 1: :50000 Presentation: angioedema, wheezing, respiratory distress and/or hypotension Treatment: STOP Transfusion Supportive Care and Airway management Epinephrine")
8
Transfusion Related Acute Lung Injury (TRALI) Life-threatening emergency Occur during or up to 6 hours following transfusion Incidence: 1:5,000-1:150,000 Pathophysiology: HLA antibodies react with antigens on recipient granulocytes. Triggers an inflammatory response in the pulmonary vasculature Presentation: pulmonary edema, tachypnea, tachycardia – hypotension, frothy pink sputum and/or fever Treatment: Stop transfusion Supportive (monitor, airway, hemodynamics) NO LASIX
 NO LASIX.")
9
Transfusion-Associated Circulatory Overload (TACO) Occur few hours following transfusion Pathophysiology : pulmonary edema 2/2 to volume overload and more common in patients with cardio vascular disease. Presentation: pulmonary edema, tachypnea, tachycardia, Hypertension Treatment: STOP Transfusion Supportive (monitor, airway, hemodynamics) Lasix
 Lasix.")
10
What is the appropriate intervention for itching associated with a blood transfusion? A. Acetaminophen B. Acute hemolytic workup C. Diphenhydramine D. Observation

11
What is the appropriate intervention for itching associated with a blood transfusion? A. Acetaminophen B. Acute hemolytic workup C. Diphenhydramine D. Observation

12
A 56-year-old man presents with an upper GI bleed from ulcer and a HG of 8. A transfusion of PRBC is started. 60 min later, pt has increased shortness of breath and his oxygen saturation drops to 91% on room air chest X-ray is shown. What management is indicated? A. Ceftriaxone and Vancomycin B. Hydrocorisone and diphenhydramine C. Intubate and Stop Transfusion D. Slow the rate of infusion

13
A 56-year-old man presents with an upper GI bleed from ulcer and a HG of 8. A transfusion of PRBC is started. 60 min later, pt has increased shortness of breath and his oxygen saturation drops to 91% on room air chest X-ray is shown. What management is indicated? A. Ceftriaxone and Vancomycin B. Hydrocorisone and diphenhydramine C. Intubate and Stop Transfusion D. Slow the rate of infusion

14
Which of the following viruses represents the most common infection transmitted in blood transfusion? A. Hepatitis A B. Hepatitis B C. Hepatitis C D. HIV

15
Which of the following viruses represents the most common infection transmitted in blood transfusion? A. Hepatitis A B. Hepatitis B C. Hepatitis C D. HIV The risk of hepatitis B transmission is 1 in 200,000 – 500,000

17
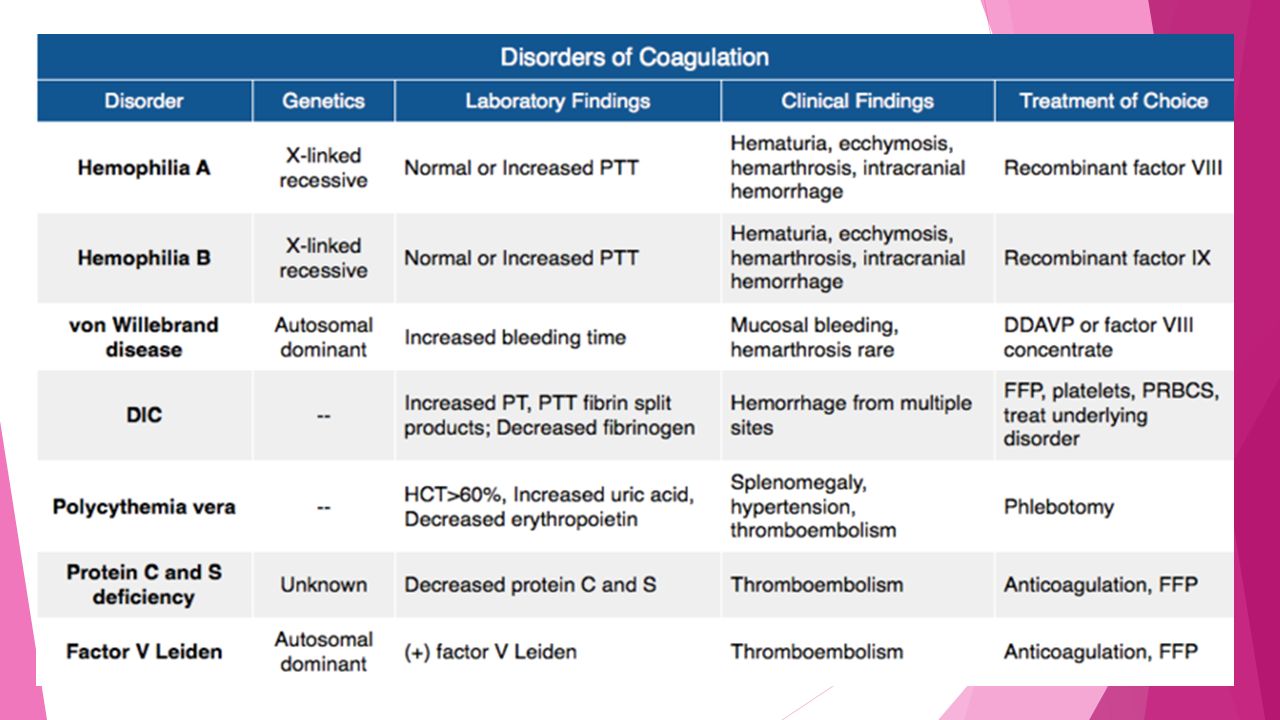
Coagulopathy Hemophilia Hemophilia A : Factor VIII deficient Hemophilia B : Factor IX deficient Von Willebrand Disease Medication Complications

19
Hemophilia X-linked recessive mutation Incidence: Hemophilia A 1:5000 male live births, Hemophilia B 1:30000 Presentations: bleeding and bruising easily Diagnosis: factor VIII and IX activity levels and aPTT Treatment: Factor VIII or IX replacement: wt x 0.5 x desired activity % FFP ( 1 u of Factor VIII per 1 ml) Cryoprecipitate ( 100 u of Factor VIII per bag) DDAVP
 Cryoprecipitate ( 100 u of Factor VIII per bag) DDAVP")
20
Von Willebrand Disease Autosomal Dominant, most common bleeding disorder Function: involved in platelet adhesion to collagen, platelet aggregation and protects Factor VIII Pathophysiology: Attaches to platelets by glycoprotein Ib receptor and connects subendothelium with platelets. Protects FVIII and delivers FVIII to the site of injury Presentations: bleeding, epistaxis, hemarthroses, hematuria. Diagnosis: Increased bleeding time and decreased vWF activity Treatment: DDAVP Non-recombinant Factor VIII Cryoprecipitate Anti-Fibirolytics: Amicar and TXA Estrogen OCP

21
Heparin Pathophysiology: activates ATIII and inactivates Xa and Thrombin. Prevents fibrin clot Monitor activity by aPTT Antidote: Protamine Sulfate Transfuse PRBCs or PLT if needed

22
Heparin Induced Thrombocytopenia Patient on heparin develops > 50 % drop in PLTs Pathophysiology: immune mediated destruction of platelets Diagnosis: when suspected send HIT assay, calculate 4 Ts score ( Timing, Thrombocytopenia, Thrombosis or other causes for thrombocytopenia ) Treatment : STOP Heparin Give non-heparin anticoagulant
 Treatment : STOP Heparin Give non-heparin anticoagulant")
23
Warfarin Pathophysiology: Vit K antagonist affecting factors II, VII, IX, X. Protein C and S. Monitor activity by INR Reversal: FFP Vit K PCC

24
Reversal for Newer Agents Plavix Platelets Pradaxa FFP, Cryoprecipitate (Factor VIII and vWF), PCC (Factors II, VII, IX and X) and dialysis. Antidote on the way Apixaban, Rivaroxaban (Xalerto) FFP, Cryo, PCC
 FFP, Cryo, PCC.")
25
A 6-year-old boy is brought in by his father 1 hour after sustaining a head injury. He was riding his bicycle down a hill and fell off after it struck a branch; he was not wearing a helmet. Medical history is significant for hemophilia A. Which of the following is the first step in management? A. Blood transfusion using 0-negative whole blood B. CT C. Factor VIII therapy to 100% activity D. Factor IX therapy to 50% activity

26
A 6-year-old boy is brought in by his father 1 hour after sustaining a head injury. He was riding his bicycle down a hill and fell off after it struck a branch; he was not wearing a helmet. Medical history is significant for hemophilia A. Which of the following is the first step in management? A. Blood transfusion using 0-negative whole blood B. CT C. Factor VIII therapy to 100% activity D. Factor IX therapy to 50% activity

27
In which of the following conditions is the patient most likely to have a normal platelet count? A. Disseminated intravascular coagulation B. Excessive hemorrhage C. Hemolytic uremic syndrome D. von Willebrand disease

28
In which of the following conditions is the patient most likely to have a normal platelet count? A. Disseminated intravascular coagulation B. Excessive hemorrhage C. Hemolytic uremic syndrome D. von Willebrand disease

29
A 43-year-old woman with a history of von Willebrand disease presents with epistaxis. Vital signs are unremarkable and exam reveals oozing from the right nares despite pressure. Which treatment is indicated in this patient’s management? A. Cryoprecipitate B. Desmopressin C. Factor VIII concentrate D. FFP

30
A 43-year-old woman with a history of von Willebrand disease presents with epistaxis. Vital signs are unremarkable and exam reveals oozing from the right nares despite pressure. Which treatment is indicated in this patient’s management? A. Cryoprecipitate B. Desmopressin C. Factor VIII concentrate D. FFP

31
A 4-year-old boy with hemophilia B presents to the ED after he fell from the monkey bars and struck his head on the ground. On exam, he has a large occipital hematoma and a GCS of 14. Which of the following should be administered? A. Cryoprecipitate B. Factor IX concentrate C. Factor VIII concentrate D. Recombinant human factor VIIa

32
A 4-year-old boy with hemophilia B presents to the ED after he fell from the monkey bars and struck his head on the ground. On exam, he has a large occipital hematoma and a GCS of 14. Which of the following should be administered? A. Cryoprecipitate B. Factor IX concentrate C. Factor VIII concentrate D. Recombinant human factor VIIa

33
A 44-year-old man is transferred from a nursing facility for thrombocytopenia. He was transferred 6 days ago for pulmonary embolism and is on low-molecular weight heparin. His platelets have fallen from 352 to 100. There is no active bleeding at this time. Which of the following is the most likely management indicated? A. Continue current therapy B. Order heparin-induced platelet aggregation studies and continue therapy while awaiting results C. Stop heparin and start Fondaparinux D. Transfuse platelets

34
A 44-year-old man is transferred from a nursing facility for thrombocytopenia. He was transferred 6 days ago for pulmonary embolism and is on low-molecular weight heparin. His platelets have fallen from 352 to 100. There is no active bleeding at this time. Which of the following is the most likely management indicated? A. Continue current therapy B. Order heparin-induced platelet aggregation studies and continue therapy while awaiting results C. Stop heparin and start fondaparinux D. Transfuse platelets

Similar presentations



 1:100 TACO1:100 TRALI1:5,000 Sepsis1:5,000 Acute hemolytic1:75,000 HBV1:160,000.>")



 – Leukocytes (WBCs) – Thrombocytes (platelets) Plasma – 90% water – 10% solutes – Proteins,>")






.>")


 1958: Plastic bag of transfusion 1656: Initial theory and.>")



