Download presentation
Presentation is loading. Please wait.

1
Intraosseous needle insertion
Dr. Mohamed Haseen Basha Assistant professor ( Paediatrics) Faculty of Medicine Al Maarefa College of Science and Technology
 Faculty of Medicine. Al Maarefa College of Science and Technology.")
2
Indications Obtain emergency access in children during life-threatening situations. cardiopulmonary arrest, shock, burns, and life-threatening status epilepticus. IO line can be used to infuse medications, blood products, or fluids.

3
Contraindications Osteogenesis imperfect Osteoporosis
Clotting disorders. Fractures in the target bone Previous orthopaedic surgery near the insertion site Previous IO insertion in the target bone within the preceding 48 hours Infection at the insertion site

4
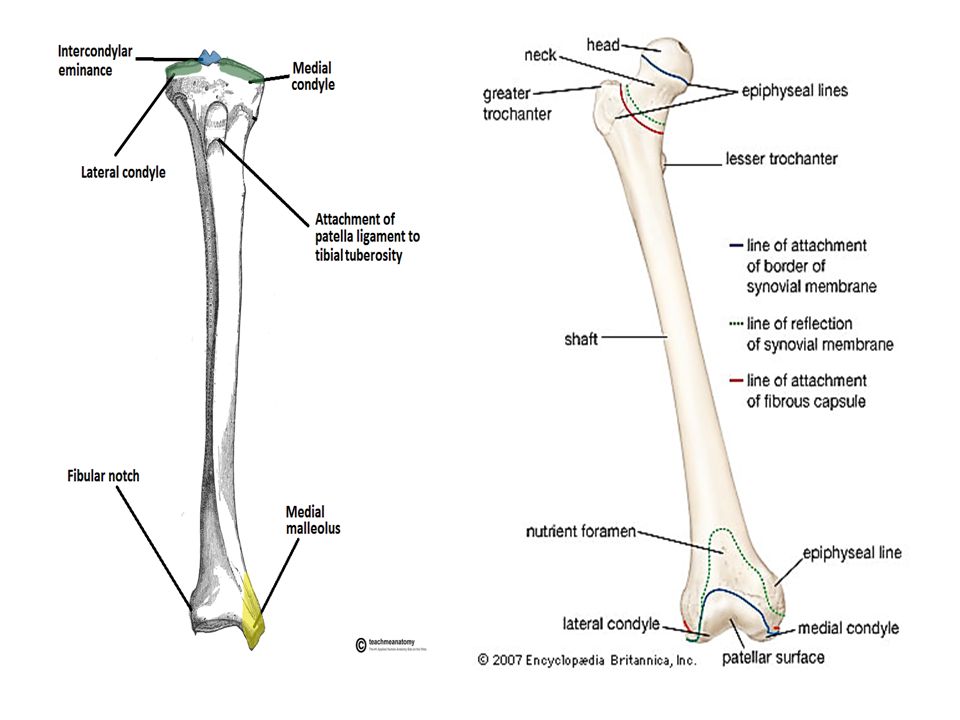
Anatomy The bone marrow cavity has an extensive virtually non-collapsible vascular network which communicates directly with the systemic circulation. Medications or fluids given by the IO route diffuse a few centimetres through the medullary cavity then enter the venous circulation. The IO needle should be removed once adequate vascular access has been established.

6
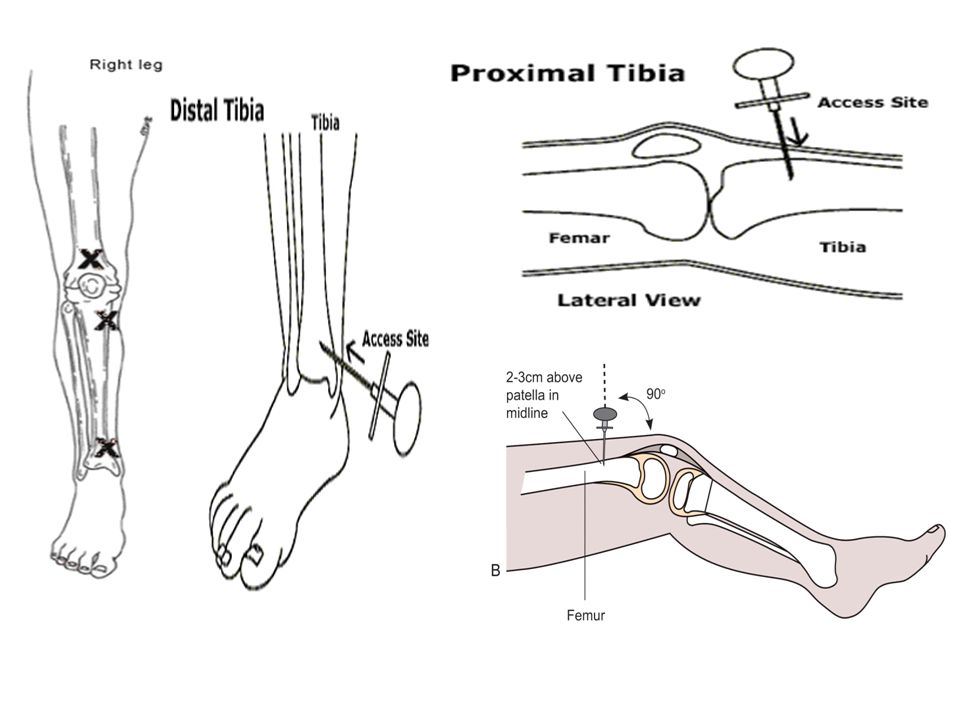
Sites Proximal Tibia Anteromedial surface of the proximal tibia, 2 cm below and 1 to 2 cm medial to the tibial tuberosity on the flat part of the bone Distal Tibia Medial surface of the distal tibia 1 to 2 cm above the medial malleolus (may be a more effective site in older children) Distal femur 3 cm above the lateral condyle in the midline
 Distal femur. 3 cm above the lateral condyle in the midline.")
8
Equipment required sterile gloves and gown basic dressing pack
antiseptic to prepare the skin rigid needle with an inner stylet (for patients < 18 months an lumbar puncture needle can be used) syringe with NaCl 0.9% flush routine IV line tubing set-up and tape
 syringe with NaCl 0.9% flush. routine IV line tubing set-up and tape.")
9
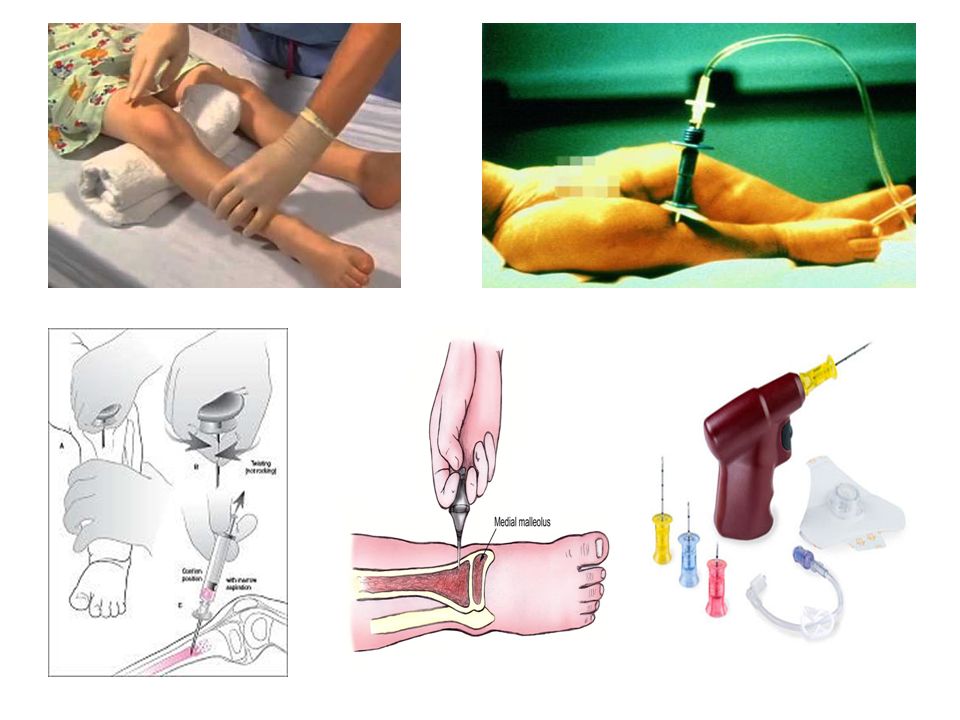
procedure Immobilize the extremity. Prepare the site with antiseptic.
Consider need to use local anaesthetic( mL 1% lignocaine ) if time permits. Insert the needle:Hold the needle handle in the palm of the hand while the thumb and forefinger grip the shaft about a centimetre from the point to stabilize the needle.
 if time permits. Insert the needle:Hold the needle handle in the palm of the hand while the thumb and forefinger grip the shaft about a centimetre from the point to stabilize the needle.")
10
Apply firm pressure while using a screwing or rotary action until the bone cortex is traversed.
Note that at approximately 1cm or less below the skin surface, a distinct loss of resistance on entry of the bone marrow is felt. Blockage of the needle may occurr if an inner stylet is not used.

11
Three indicators of successful insertion
A distinctive pop with insertion, or a give or release of resistance is felt. The needle flushes without significant subcutaneous infiltration and bone marrow is easily aspirated. The needle stands without support.

12
After successful insertion
Once insertion is confirmed: Unscrew and remove the stylet. Attempt bone marrow aspiration (bone marrow can be used as a substitute for venous blood for estimation of PCO2, pH, Hb, electrolytes, urea, creatinine, proteins etc). Flush the needle with 5-10 mL of normal saline to decrease the cellularity of the surrounding marrow, aiding subsequent infusions. Attach IV tubing and commence the infusion of medications or fluids by pump.
. Flush the needle with 5-10 mL of normal saline to decrease the cellularity of the surrounding marrow, aiding subsequent infusions. Attach IV tubing and commence the infusion of medications or fluids by pump.")
13
Absorption Recommended intravenous rates for drugs and fluids can be administered via the IO route and reach the central circulation in equivalent times. Strong alkaline and hypertonic solutions should be diluted before use.

15
complications fracture of the target bone infection extravasation
subperiosteal infusion embolism compartment syndrome pain on use dislodgement skin necrosis

Similar presentations










 infusion. The anatomical and physiological principle of I.O. infusion. Familiarization.>")








