Download presentation
Presentation is loading. Please wait.

1
Quinolone and Aminoglycoside Antibiotics Edgar Rios, Pharm.D., BCPS MHH Clinical Pharmacist UTHSCH Clinical Assistant Professor

2
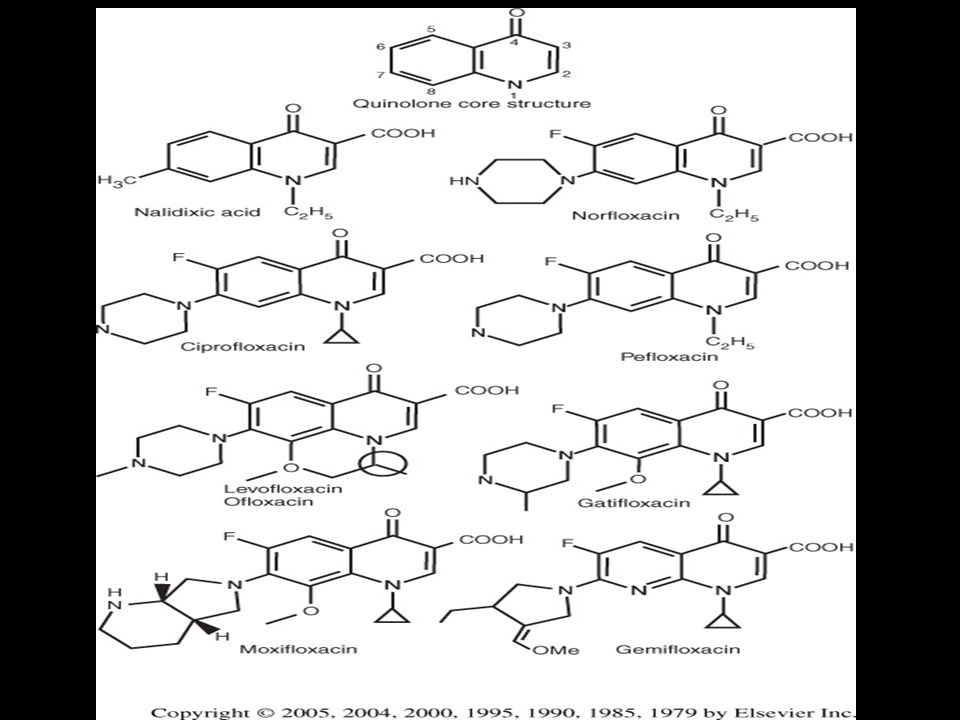
Overview Chemical Structure Chemical Structure Classifications and spectrum of activity Classifications and spectrum of activity Mechanism of action and resistance Mechanism of action and resistance Pharmacologic properties and pharmacodynamics Pharmacologic properties and pharmacodynamics Adverse effects Adverse effects Clinical uses Clinical uses

7
Silver Nature Reviews Drug Discovery 6, 41–55 (January 2007) | doi:10.1038 / nrd2202
 | doi: / nrd2202")
8
Mechanisms of resistance Alterations in target enzymes Alterations in target enzymes Chromosomally mediated Chromosomally mediated Occur in 1 in 10 6 to 1 in 10 9 bacteria Occur in 1 in 10 6 to 1 in 10 9 bacteria Resistance arises in a stepwise fashion Resistance arises in a stepwise fashion Decreased permeation Decreased permeation Changes in porins (OmpF) Changes in porins (OmpF) Efflux pumps (MexAB-OprM) Efflux pumps (MexAB-OprM) Low to intermediate levels of resistance Low to intermediate levels of resistance Can effect other drugs Can effect other drugs Plasmid meditated resistance Plasmid meditated resistance qnr gene qnr gene Protects DNA gyrase and topoisomerase IV Protects DNA gyrase and topoisomerase IV Low level resistance Low level resistance
 Changes in porins (OmpF) Efflux pumps (MexAB-OprM) Efflux pumps (MexAB-OprM) Low to intermediate levels of resistance Low to intermediate levels of resistance Can effect other drugs Can effect other drugs Plasmid meditated resistance Plasmid meditated resistance qnr gene qnr gene Protects DNA gyrase and topoisomerase IV Protects DNA gyrase and topoisomerase IV Low level resistance Low level resistance")
11
Pharmacodynamic Interactions MIC Concentration Time Peak/MIC AUC/MIC

13
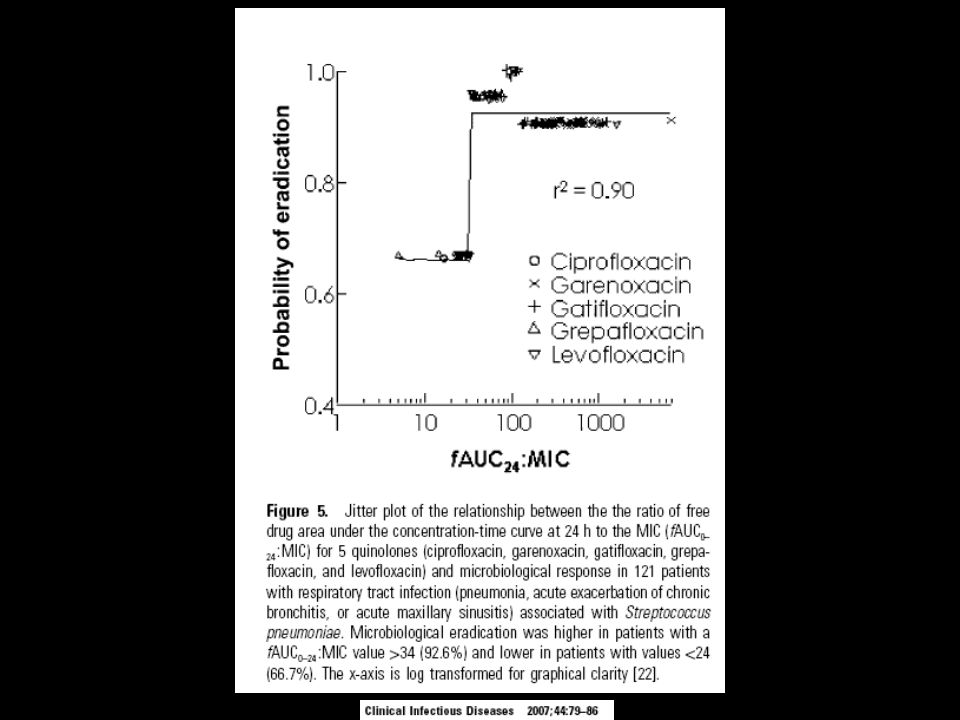
Relationship Between AUC 24 /MIC and Efficacy of Ciprofloxacin in Patients with Serious Bacterial Infections Forrest A, et al. AAC, 1993; 37: 1073-1081

14
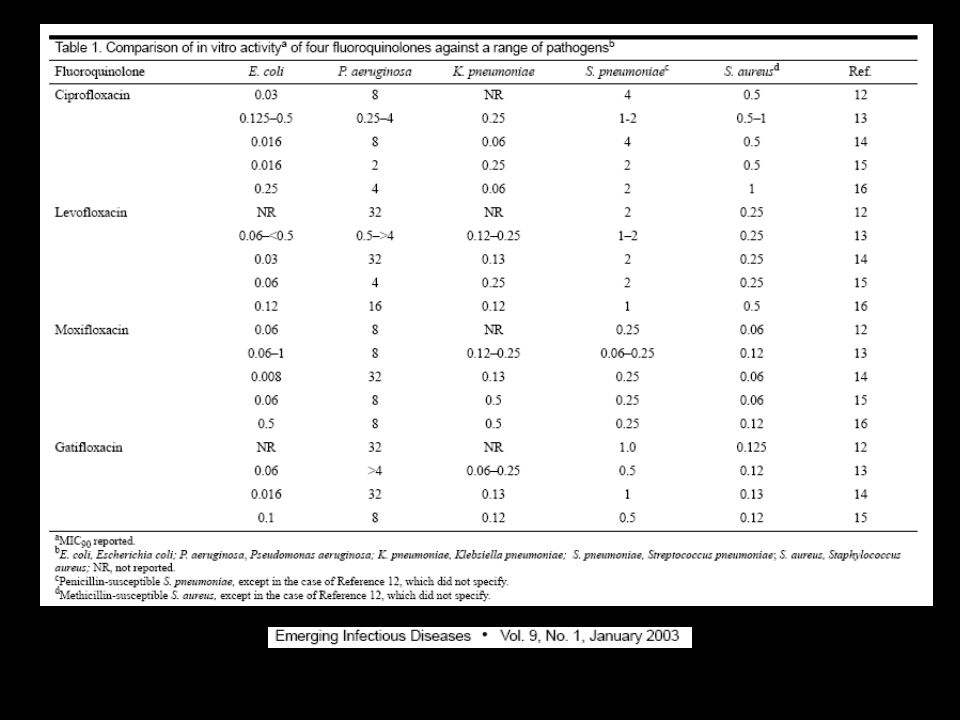
Proposing PK/PD limits for sensitivity PK values PK/PD limits Breakpoints (mg/L) DrugDaily DoseCmaxAUCEfficacy EUCASTCLSI (mg/L)(mg*h/L)(mg/L) AUC/MIC(S-R)(S,I,R) Cipro1000mg2.5240.2,0.8120,30 1 4 1500mg3.632160,40 Levo500mg4.0400.3,0.9133,44 2 8 Moxi400mg3.1350.2,0.7175,50 1 8 (G-) 4 (G+) Adapted with data from: Clin Microbiol Infect 2005; 11:256-280 Emerging Infectious Diseases 2003; 9:1-9
 DrugDaily DoseCmaxAUCEfficacy EUCASTCLSI (mg/L)(mg*h/L)(mg/L) AUC/MIC(S-R)(S,I,R) Cipro1000mg ,0.8120, mg ,40 Levo500mg ,0.9133, Moxi400mg ,0.7175, (G-) 4 (G+) Adapted with data from: Clin Microbiol Infect 2005; 11: Emerging Infectious Diseases 2003; 9:1-9")
17
Clinical Uses IndicationCiproLevoMoxi UTIXX ProstatitisXX GonorrheaX GastroenteritisX Intra-abdominal infectionX a X b Respiratory tract infectionXXX Bone and joint infectionX Skin and skin structure infectionXXX a In combination with metronidazole b As monotherapy

18
Aminoglycosides AgentSourceYear StreptomycinStreptomyces griseus1944 NeomycinStreptomyces fradiae1949 KanamycinS. kanamyceticus1957 ParomomycinS. fradiae1959 SpectinomycinS. spectabilis1962 GentamicinMicromonospora purpurea1963 and M. echinospora and M. echinospora Tobramycin S. tenebrarius1968 Amikacin S. kanamyceticus1971 Netilmicin M. inyoensis1975

19
Mechanism of Action

20
Resistance Alteration in ribosomal binding sites Mycobacterial resistance to streptomycin Mycobacterial resistance to streptomycin Altered uptake Staph spp. and Pseudomonas aeruginosa Staph spp. and Pseudomonas aeruginosa Aminoglycoside modifying enzymes Plasmids and transposons Plasmids and transposons Confer cross resistance Confer cross resistance Amikacin least effected Amikacin least effected

21
Spectrum Gentamicin = tobramycin < amikacin Gram-negative organisms Fermenters and Pseudomonas aeruginosa Fermenters and Pseudomonas aeruginosa Gram-positive organisms Staphylococcus spp. and Enterococci Staphylococcus spp. and EnterococciMiscellaneous

22
Pharmacokinetics Absorption Not absorbed orally Not absorbed orally Must be given parenterally Must be given parenterallyDistribution Poor into most tissues Poor into most tissuesElimination Renal Renal

23
Concentration vs Time-dependent Killing TobramycinTicarcillin Time (hours)
")
24
Peak/MIC Ratio and Clinical Response with Aminoglycosides Moore,et al. J Inf Disease, 1987; 155(1): 93-98
:")
25
Does “S” Really Mean Sensitive? MICGent/TobraAmikacin 0.253284 0.51640 1820 2410 425 812.5 160.51.25 320.250.625 640.1250.3125 SIR G/T 16 A 64 G/T: 2 mg/kg = 8 mcg/ml A: 5 mg/kg = 20 mcg/ml Peak / MIC Peak serum concentration CLSI breakpoints

26
Once Daily vs Traditional Dosing What’s the difference? Rational Concentration-dependent killing Concentration-dependent killing Post antibiotic effect Post antibiotic effect Bacteria remains “stunned” even without any drug Bacteria remains “stunned” even without any drug Allows for a drug free interval Allows for a drug free interval Less toxicity Less toxicity

27
ODA vs Traditional Dosing

28
Once Daily vs Traditional Dosing? Evidence for once daily Pneumonia, UTI, PID, IAI, bacteremia Pneumonia, UTI, PID, IAI, bacteremia Lack of evidence for once daily Geriatric, CrCl <20ml/min, obese, pregnant, burn, cystic fibrosis, ascites, osteomyelitis, enterococcal infections Geriatric, CrCl <20ml/min, obese, pregnant, burn, cystic fibrosis, ascites, osteomyelitis, enterococcal infections

29
Once Daily Dosing Dose Gent/tobra =7 mg/kg(peak ~ 20mcg/ml) Amikacin =15 mg/kg(peak ~ 40mcg/ml) Interval:every 24 hours (ClCr > 60ml/min) every 36 hours (ClCr 40 – 60ml/min) every 36 hours (ClCr 40 – 60ml/min)Monitor Level 6 – 14 hours after starting the infusion Trough (needs to be undetectable), renal function
 Amikacin =15 mg/kg(peak ~ 40mcg/ml) Interval:every 24 hours (ClCr > 60ml/min) every 36 hours (ClCr 40 – 60ml/min) every 36 hours (ClCr 40 – 60ml/min)Monitor Level 6 – 14 hours after starting the infusion Trough (needs to be undetectable), renal function")
30
Antimicrob Agents Chemother. 1995;39:650-55.

31
Traditional Dosing How to dose? Based on volume of distribution (0.25-0.3 L/kg) Peak serum levels (mcg/ml) Pneumonia/sepsissoft tissueUTI Gent/tobra6-10 5-74-6 Amikacin25-30 20-25 20 Loading Dose: Gent/tobra2 - 3 mg/kg Amikacin7.5 mg/kg Maintenance doses (mg/kg): Pneumonia/sepsissoft tissueUTI Gent/tobra 1.8-2 1.5 1 Amikacin 6.5 5.5 4 Trough Levels (mcg/ml) Gent/tobra < 2Amikacin 4-10
 Peak serum levels (mcg/ml) Pneumonia/sepsissoft tissueUTI Gent/tobra Amikacin Loading Dose: Gent/tobra2 - 3 mg/kg Amikacin7.5 mg/kg Maintenance doses (mg/kg): Pneumonia/sepsissoft tissueUTI Gent/tobra Amikacin Trough Levels (mcg/ml) Gent/tobra < 2Amikacin")
32
Traditional Dosing What interval do I choose? Based on CrCl (renal function) CrCl (ml/min)t1/2 (hours)interval (hours) >75 75 < 38 51-75 3-4.412 51-75 3-4.412 25-50 4.5-824 25-50 4.5-824 8> 24 8> 24 What do I monitor? Levels, renal function, ototoxicity
 CrCl (ml/min)t1/2 (hours)interval (hours) >75 75 < > 24 8> 24 What do I monitor. Levels, renal function, ototoxicity.")
34
Conclusion Fluoroquinolones Fluoroquinolones Broad-spectrum but differences Broad-spectrum but differences Resistance increasing Resistance increasing Concentration dependent killing (AUC/MIC) Concentration dependent killing (AUC/MIC) Well tolerated Well tolerated Aminoglycosides Aminoglycosides Resurgence because of resistance Resurgence because of resistance Mainly gram negative activity Mainly gram negative activity Concentration dependent killing (Peak/MIC) Concentration dependent killing (Peak/MIC) Serious toxicities Serious toxicities
 Concentration dependent killing (AUC/MIC) Well tolerated Well tolerated Aminoglycosides Aminoglycosides Resurgence because of resistance Resurgence because of resistance Mainly gram negative activity Mainly gram negative activity Concentration dependent killing (Peak/MIC) Concentration dependent killing (Peak/MIC) Serious toxicities Serious toxicities")
35
Bedside kinetics Typical Vd = 0.25 – 0.3 L/kg Typical half life = 2.5 -3 hours (with ClCr > 60ml/min) Wt: 80kgGoal peak: 10 mg/L LD = (80kg * 0.3 L/kg) * 10 mg/L = 240 mg At 3 half lives Conc = (10/2) = (5/2) = (2.5/2) = 1.25 Goal trough: 1mg/L MD = (10 mg/L – 1 mg/L) * 24 L = 216 ~ 220 mg
 Wt: 80kgGoal peak: 10 mg/L LD = (80kg * 0.3 L/kg) * 10 mg/L = 240 mg At 3 half lives Conc = (10/2) = (5/2) = (2.5/2) = 1.25 Goal trough: 1mg/L MD = (10 mg/L – 1 mg/L) * 24 L = 216 ~ 220 mg")
36
Dosage Regime Manipulation: Peaks/Troughs Concentration Parameter Manipulation P high, T OK Decrease dose P low, T OK Increase dose** P OK, T high Increase interval P OK, T low Decrease interval P high, T high Decrease dose, Increase interval P low, T low Increase dose, decrease interval ** Trough may increase**

Similar presentations














 * most commonly used Antibacterial Spectrum Bactericidal ( exclusive.>")









