Download presentation
Presentation is loading. Please wait.

1
1 Health System Resilience Amidst Political Instability The case of Lebanon Harvard Kennedy School Sept. 2015 Walid Ammar MD, Ph.D.

2
2 Health System Resilience Amidst Political Instability The case of Lebanon This presentation is not meant to introduce the health system in Lebanon as a model to follow in normal circumstances. It does not pretend either that the system has been able to satisfy all needs of the Syrian refugees, who are still facing obstacles to access certain hospital services. No country could reasonably be expected to cater for needs of a massive influx of refugees, increasing suddenly its population by one third. The purpose of this presentation is to show how the health care system in Lebanon has been able to absorb recurring pressures and shocks, particularly the recent Syrian Crisis, and to sustain its functions and achievements, and even improve some. Hence challenging certain well established concepts and paradigms in relation to health system’s performance. Walid Ammar, MD.; Ph.D. - 2015

3
3 The political system in Lebanon Characteristics of the health system Political instability context with focus on the recent syrian crisis Resilience indicators Factors behind resilience Walid Ammar, MD.; Ph.D. - 2015 Health System Resilience Amidst Political Instability The case of Lebanon

4
4 The Political System Lebanon is a small country of 10452 km 2, and a population of 4 million inhabitants including 400000 Palestinian refugees (2010). The political system is described as parliamentarian democratic. In fact the regime is an oligarchy established on power sharing based on religious affiliation (18 sects). The health system operates in a context of free market economy with a strong tradition of laissez-faire. The economy is service-oriented (76%), mainly banking and tourism. In 2013, Nominal GDP was 47.2 billion USD at current prices, and a GDP per capita of 11,324 USD. Walid Ammar, MD.; Ph.D. - 2015
. The health system operates in a context of free market economy with a strong tradition of laissez-faire. The economy is service-oriented (76%), mainly banking and tourism. In 2013, Nominal GDP was 47.2 billion USD at current prices, and a GDP per capita of 11,324 USD. Walid Ammar, MD.; Ph.D")
5
5 Sectarianism and Distorted Accountability Governing political parties have an interest in keeping the government weak and using their own channels to provide services. Mechanisms to hold parties accountable, such as elections, are perverted by sectarian considerations. External financial and political support to political groups diverts accountability to regional powers, where coalitions are mostly based on confessionnel loyalties. Walid Ammar, MD.; Ph.D. - 2015

6
6 Health Coverage in Lebanon Walid Ammar, MD.; Ph.D. - 2015 6 Public Funds Private Insurance (& Mutual Funds) 12% Almost half of the population, has no formal insurance, and is entitled to the coverage of the Ministry of Public Health (MOPH). Social Security Fund 28% Civil Servants Cooperative 5% 4 Military Schemes 9%
 12% Almost half of the population, has no formal insurance, and is entitled to the coverage of the Ministry of Public Health (MOPH). Social Security Fund 28% Civil Servants Cooperative 5% 4 Military Schemes 9%.")
7
7 MOPH Coverage As the insurer of last resort, the MOPH covers hospital care and expensive treatments i.e what may constitute a catastrophic spending for households (ensuring accessibility while protecting households from impoverishment). The MOPH does not reimburse ambulatory care. It provides, however, an alternative for the poor by subsidizing a comprehensive package of PHC services through a wide network of PHC centers. Walid Ammar, MD.; Ph.D. - 2014

8
8 Strong Private Sector Walid Ammar, MD.; Ph.D. - 2015 Overwhelming Private provider: 75% of hospitals beds 90% of ambulatory care facilities Oversupply and supplier induced demand: - Physicians 32 per 10000 (average of 13 in EMR). - CT Scan machines 26 per million (15 in Canada).
. - CT Scan machines 26 per million (15 in Canada)..")
9
9 Weak Government Complex and lengthy decision making processes at both legislative and executive levels. Lack of MOPH authority, incapacity to enforce laws for both political and institutional reasons. Walid Ammar, MD.; Ph.D. - 2015

10
10 Fragmentation Overlapping & gaps in coverage Weakens the bargaining power of public funds Hinders planning and regulation, inability to see the whole picture Risk pooling issues Provision Fragmentation: Public / private. No formal referral system through different levels of health care. Walid Ammar, MD.; Ph.D. - 2014

11
11 Failed Reform Attempts Walid Ammar, MD.; Ph.D. - 2014 Restructuring the MOPH Control of Supply / Carte Sanitaire Unifying Public Funds & Expanding the SS coverage

12
12 Civil war 1975-1999 Wars with Israel 1982, 1993, 1996, 2006 Armed conflicts at the borders with Syria since 2011 Social tension and confessionnel disputes Paralysis of political institutions Walid Ammar, MD.; Ph.D. - 2014 Political Instability Context

13
13 The influx of Syrian refugees started in 2011 1,500,000 Syrian refugees 52,000Palestinian Refugees from Syria 40,000Lebanese residents in Syria 1,000,000 host community members directly affected by the Syrian crisis The equivalent % of refugees to the French population would be 20,000,000 refugees. The EU (500 million) considers itself in a state of crisis for an influx of less than 100,000 syrian refugees. Walid Ammar, MD.; Ph.D. - 2014 The Impact of the Syrian Crisis
 considers itself in a state of crisis for an influx of less than 100,000 syrian refugees. Walid Ammar, MD.; Ph.D The Impact of the Syrian Crisis.")
14
14 The WB in collaboration with UN, EU, IMF conducted a study quantifying the impact and stabilization needs of Lebanon. It was estimated at 7 billion USD. (Lebanon, Economic and Social Impact Assessment of the Syrian Conflict. September, 2013) The current estimate is at 10 billion USD only a total of 1.6 billion USD transferred from 2011 till 2014 Walid Ammar, MD.; Ph.D. - 2014 The Impact of the Syrian Crisis
 The current estimate is at 10 billion USD only a total of 1.6 billion USD transferred from 2011 till 2014 Walid Ammar, MD.; Ph.D The Impact of the Syrian Crisis.")
15
15 Health System Resilience Capacity to absorb pressures and shocks, to prevent or contain outbreaks, to maintain its institutions functional and sustain achievements. In terms of Inputs: Human resources - Production - Retention problems Financial resources- MOPH budget and public spending - Disbursement delays - Deficient financial assistance from the international community. In terms of Process: Operationality of Public and Private institutions Governance, financing and provision functions of the health system: level of functionality Walid Ammar, MD.; Ph.D. - 2015

16
16 Health System Resilience In terms of Outputs and outcomes : No discrimination between Lebanese and non- Lebanese at the PHC level. This is unfortunately not the case in hospital care. Evidence shows that provided services have been steadily increasing in both PHC and hospital care. Major outbreaks were controlled (measles, hep. A) or prevented (Polio, leishmaniasis, cholera…) MDGs 4 & 5 achieved Walid Ammar, MD.; Ph.D. - 2014
 or prevented (Polio, leishmaniasis, cholera…) MDGs 4 & 5 achieved Walid Ammar, MD.; Ph.D")
17
17 Out Of Pocket In a context of increased demand for health care (older population and higher prevalence of NCDs) and high cost of medical technology: Imposed fees and co-payment may hinder the accessibility of the poor to health services. Health spendings may become catastrophic for the near poor and push them under the poverty line. The MOPH strategy focused on reducing OOP (mainly by improving accessibility to PHC) from 60% of THE in the 90’s, (spent mostly on private ambulatory services) to less than 40%. Walid Ammar, MD.; Ph.D. - 2014
 from 60% of THE in the 90’s, (spent mostly on private ambulatory services) to less than 40%. Walid Ammar, MD.; Ph.D")
18
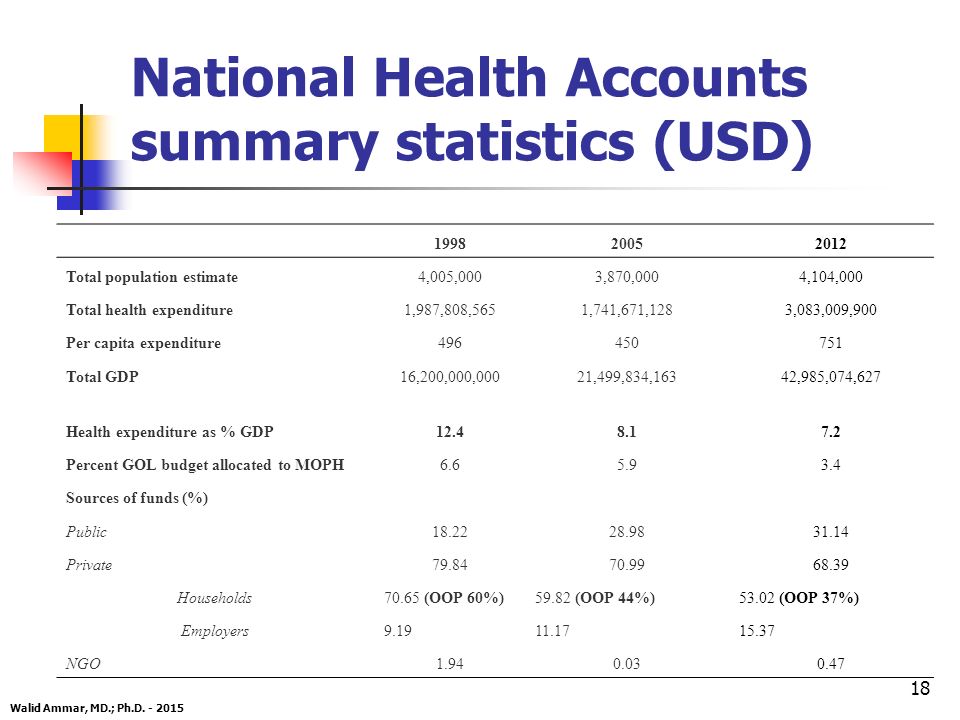
18 National Health Accounts summary statistics (USD) 199820052012 Total population estimate4,005,0003,870,000 4,104,000 Total health expenditure1,987,808,5651,741,671,128 3,083,009,900 Per capita expenditure496450 751 Total GDP16,200,000,00021,499,834,163 42,985,074,627 Health expenditure as % GDP12.48.1 7.2 Percent GOL budget allocated to MOPH6.65.9 3.4 Sources of funds (%) Public 18.2228.9831.14 Private 79.8470.9968.39 Households 70.65 (OOP 60%)59.82 (OOP 44%)53.02 (OOP 37%) Employers 9.1911.1715.37 NGO1.940.030.47 Walid Ammar, MD.; Ph.D. - 2015
19
19 MDGs related health indicators 19901995200020042013* IMR (per 1000 live births)35332716.18 <5 MR (per 1000 live births)43403518.39 Births attended by skilled health personnel (%) 458998.2 Maternal Mortality Ratio (per 100,000)30013010486.316 Walid Ammar, MD.; Ph.D. - 2015 MMR 2008 LEB 26 (World Statistics Report Sept. 2010), >5MR (2009) 10‰ (MICS 3, 2011) * World Health Statistics Maternal deaths among refugees are proportionally close to those of the Lebanese and are included in the 2013 national MMR of 16, compared to 2010 MMR in Syria of 70 per 100000
, >5MR (2009) 10‰ (MICS 3, 2011) * World Health Statistics Maternal deaths among refugees are proportionally close to those of the Lebanese and are included in the 2013 national MMR of 16, compared to 2010 MMR in Syria of 70 per")
20
Health Reform in Lebanon: A success story in the "WHO Report 2010 on Health Care Financing"

21
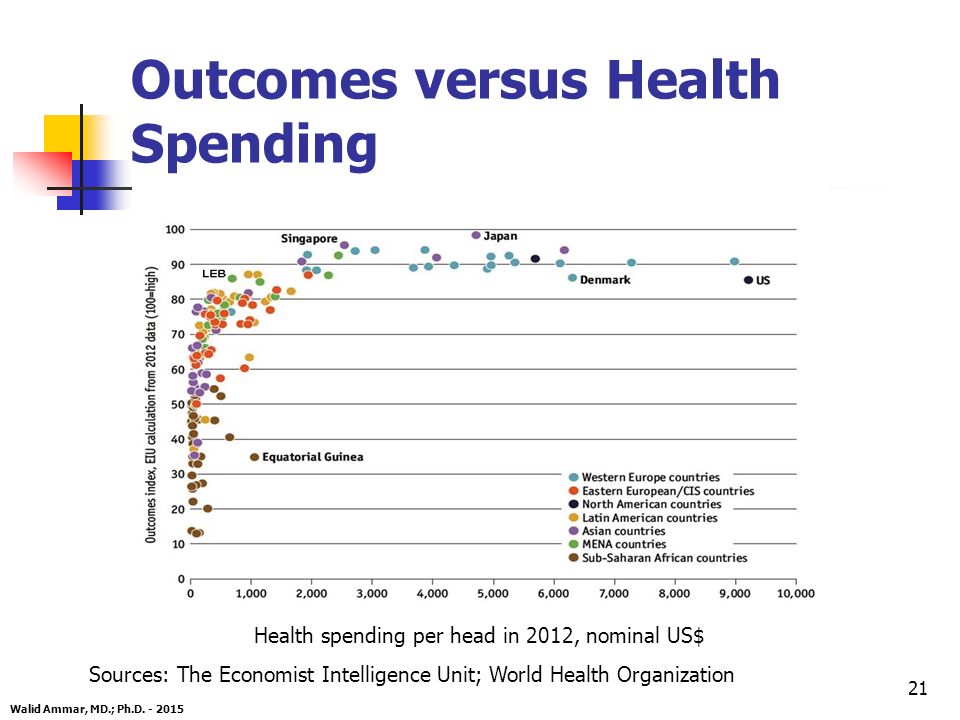
21 Outcomes versus Health Spending Health spending per head in 2012, nominal US$ Sources: The Economist Intelligence Unit; World Health Organization Walid Ammar, MD.; Ph.D. - 2015
22
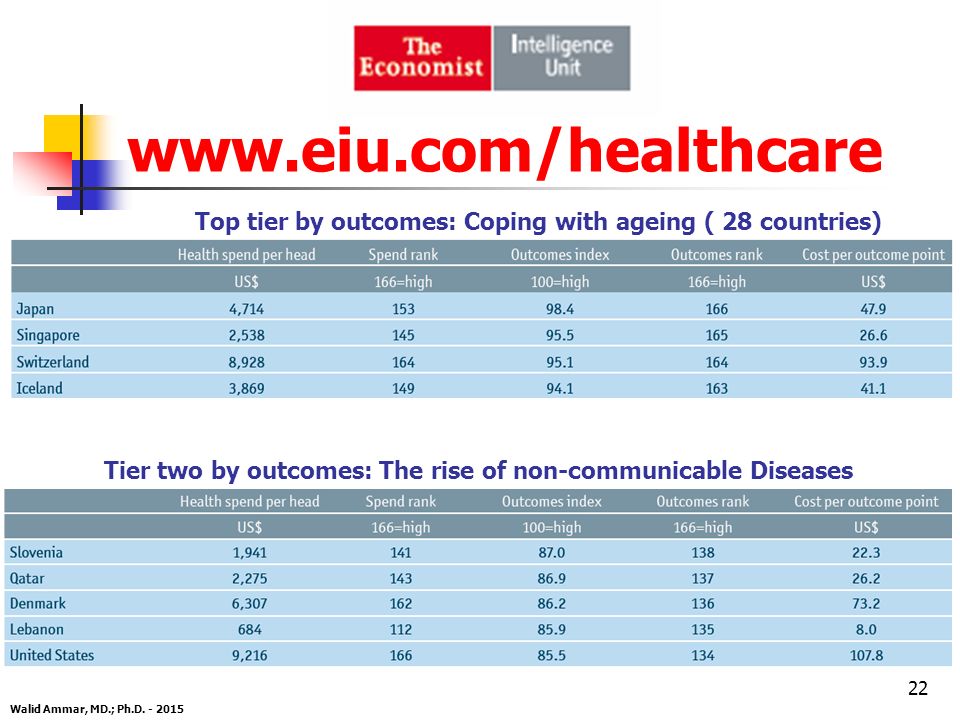
www.eiu.com/healthcare Top tier by outcomes: Coping with ageing ( 28 countries) Tier two by outcomes: The rise of non-communicable Diseases Walid Ammar, MD.; Ph.D. - 2015 22
23
23 ? how to deal at the same time with: Strong private sector. Weak Government. Fragmented health system. MOPH lack of authority. Increasing demand. MOPH shortage in human and financial resources. A chronic context of political instability. Acute crisis of massive influx of Syrian refugees and their distribution all over the country. Walid Ammar, MD.; Ph.D. - 2015

24
24 Weak Regulation VS Flexibility Legislation loopholes offer room for manoeuver. Capacity to adapt and innovate. Soft Regulation through contracting, in the framework of Public-Private partnership. Results based monitoring and accountability (to bypass resource consuming procedural control). Financing as a leverage for enforcing regulations (MOPH financing is a consequence of unaccomplished Social Security coverage). Walid Ammar, MD.; Ph.D. - 2015
. Financing as a leverage for enforcing regulations (MOPH financing is a consequence of unaccomplished Social Security coverage). Walid Ammar, MD.; Ph.D")
25
25 Fragmentation VS Diversity Mitigating fragmentation while benefiting from the advantages of diversity. Diversity: Of sources of funding: balance between taxes, contributions and OOP. Of Institutions with different problems at different times. Of Interveners at different levels of provision. Walid Ammar, MD.; Ph.D. - 2015

26
26 Participation as a Principle of Good Governance Opportunities Formal participation frameworks (provided for by law). Active Civil Society and a strong NGO sector. Professional Orders legally representing different professions. Long history of contracting with the private sector. Challenges Absence of strong and credible consumer associations. Patients’ associations are very few and weak (sometimes manipulated). Disfunctioning national accountability mechanisms. Centralized public administration (MOPH). Walid Ammar, MD.; Ph.D. - 2015
. Disfunctioning national accountability mechanisms. Centralized public administration (MOPH). Walid Ammar, MD.; Ph.D")
27
27 Engaging NGOs and Municipalities After 17 years of civil war, the MOPH decided to capitalize on the NGOs resources and created the National PHC Network. MOPH-NGOs Relationship formalized by contractual agreements. Municipalities included as partners. Policy Level: Steering representative Committee Tripartite contracting agreements Legal framework based on common understanding. (explicit commitment to a comprehensive package of services and quality of care, performance based financing). Outcome based contracting (soft responsive regulation). Consumer empowerment Provide information on patient rights & Patient satisfaction surveys. Walid Ammar, MD.; Ph.D. - 2015
. Outcome based contracting (soft responsive regulation). Consumer empowerment Provide information on patient rights & Patient satisfaction surveys. Walid Ammar, MD.; Ph.D")
28
28 Give weight to the consumer voice vis-à-vis the provider Patient satisfaction linked to payment Election of municipality council members Accountability at the polls Accountability of the health center to the NGO Organizational accountability Accountability of the NGO to the MOPH accountability through contracting Walid Ammar, MD.; Ph.D. - 2014 Accountability in PHC

29
29 Hospital Care Accountability Framework Performance based financing Case-mix and output indicators Accreditation Patients reporting on: - Perception of quality of care - Extra payment imposed by provider - Responsiveness of provider to patient’s non medical expectations Contracting as a tool to improve quality and to meet patient’s expectations. Walid Ammar, MD.; Ph.D. - 2015

30
30 Concepts & Paradigms Should multiplicity of financing and provision still be considered as detrimental? Or should we benefit from diversity to promote competition, complementarity and mutual support? What about oversupply of physicians, hospital beds and high tech equipment? And the capacity to absorb an increased demand of a “flourishing medical tourism” or resulting from high influx of refugees!? Walid Ammar, MD.; Ph.D. - 2015

31
31 Should we rely more on legislation to regulate the health sector considering the Lebanese context and to what extent? VS developing negotiation skills and institutional capacity for contracting as a soft and flexible tool for regulation? Should refugees be concentrated in camps to be well controlled (by a strong government) and to facilitate delivery of services? or should they be left spreading all over the country, which helps distributing their burden over numerous communities and health providers? Walid Ammar, MD.; Ph.D. - 2015 Concepts & Paradigms
 and to facilitate delivery of services. or should they be left spreading all over the country, which helps distributing their burden over numerous communities and health providers. Walid Ammar, MD.; Ph.D Concepts & Paradigms.")
32
32 Political Dimensions Take strength from science to face the perverting “power” of confessionalism. Health is a uniting cause which helps overcome the hatred of “the other”, and break the vertical division of society and the vertical allegiance to sectarian parties. Create new accountability frameworks to palliate the deficient existing mechanisms. Enhance decentralization and community involvement. Overcome the lack of authority and resources Capitalize on existing resources (NGOs, Municipalities, Private Sector) Create soft tools rather than coercive legislations Use financing as leverage for change Performance contracting and results based management Walid Ammar, MD.; Ph.D. - 2014
 Create soft tools rather than coercive legislations Use financing as leverage for change Performance contracting and results based management Walid Ammar, MD.; Ph.D")
33
33 Conclusion Behind system’s weaknesses there are strengths that most often are the other side of the same coin. It is all about system dynamics within a specific context… and definitely a matter of governance. Walid Ammar, MD.; Ph.D. - 2014

Similar presentations














IS?. Purpose of HIS “is to produce relevant information that health system stakeholders can use for making transparent and evidence-based.>")




