Download presentation
Presentation is loading. Please wait.

1
Behavioral Pediatrics: The Top Three
Jodi Polaha, Ph.D. Assistant Professor, Pediatrics Munroe-Meyer Institute

2
Behavioral Health Clinics

3
Why Primary Care? Physicians as gate keepers for mental health services

4
Why Primary Care? Physicians as gate keepers for mental health services Increased continuity of care

5
Why Primary Care? Physicians as gate keepers for mental health services Increased continuity of care De-stigmatizes mental health treatment

6
Top Three Problems Behavior-based problems (58%) Otitis Media (48%)
URI (41%) Arndorfer, R. E., Allen, K. D., Aljazireh, L. (1999). Behavioral health needs in pediatric medicine and the acceptability of behavioral solutions: Implications for behavioral psychologists. Behavior Therapy, 30,
 Arndorfer, R. E., Allen, K. D., Aljazireh, L. (1999). Behavioral health needs in pediatric medicine and the acceptability of behavioral solutions: Implications for behavioral psychologists. Behavior Therapy, 30,")
7
Top Three Behavior Problems
Oppositional behavior Sleep/bedtime problems ADHD Arndorfer, R. E., Allen, K. D., Aljazireh, L. (1999). Behavioral health needs in pediatric medicine and the acceptability of behavioral solutions: Implications for behavioral psychologists. Behavior Therapy, 30,
. Behavioral health needs in pediatric medicine and the acceptability of behavioral solutions: Implications for behavioral psychologists. Behavior Therapy, 30,")
8
Case #1 5 y.o. boy at well-child check Questions
Mom’s main concern is sleep Notes he is aggressive at school Questions What concerns should be assessed? What screening measures should be used? What diagnoses should be considered? What recommendations should be made?

9
Oppositional Behavior
Core issue is typically noncompliance How many of 10 instructions would s/he do the first time asked? Mealtimes? Bedtime? Public outings?

10
Oppositional Behavior
Significant problems will not dissipate with age

11
Oppositional Behavior
Oppositional Defiant Disorder (DSM-IV) 6 month pattern of negative, hostile, defiant behavior with 4 of the following: Loses temper Argues with adults Blames others Etc. Causes Impairment Not psychosis Not Conduct Disorder
 6 month pattern of negative, hostile, defiant behavior with 4 of the following: Loses temper. Argues with adults. Blames others. Etc. Causes Impairment. Not psychosis. Not Conduct Disorder.")
12
Oppositional Behavior
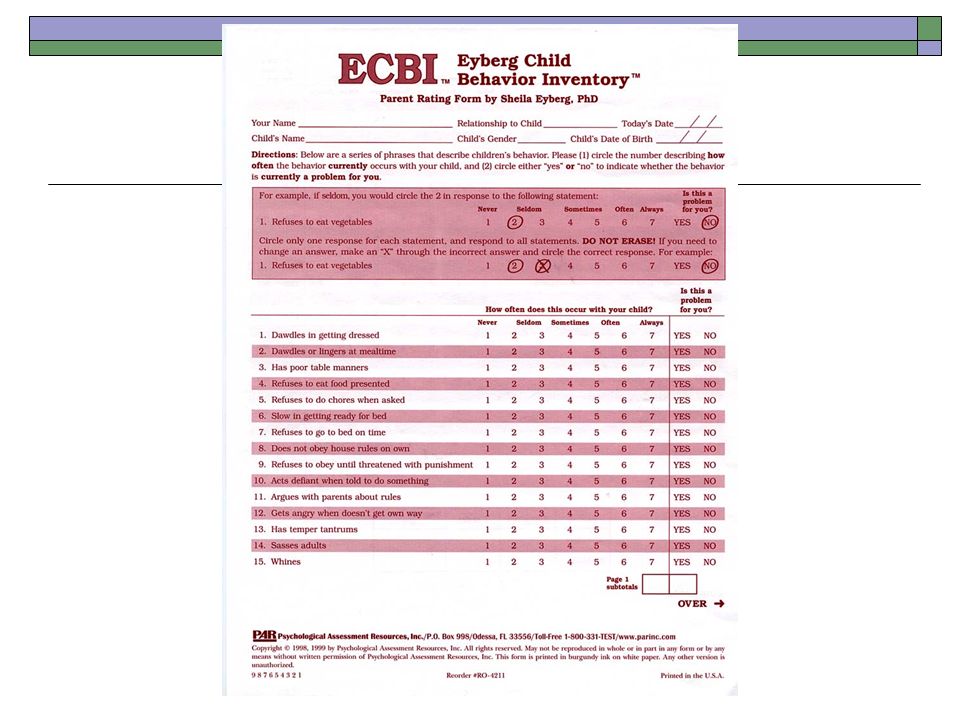
Use behavioral screening such as the Eyberg Child Behavior Checklist (ECBI) For those who exceed cutoff, consider referral to behavioral health specialist. For those who do not, but have concerns, provide handouts, brief verbal guidance based on empirically supported findings.
 For those who exceed cutoff, consider referral to behavioral health specialist. For those who do not, but have concerns, provide handouts, brief verbal guidance based on empirically supported findings.")
14
Oppositional Behavior
Talking with parents: “teaching a behavioral skill” Following instructions Coping with anger Persisting on a task Self-quieting

15
Oppositional Behavior
Talking with parents: “teaching a behavioral skill” Following instructions Coping with anger Persisting on a task Self-quieting Must use two-part approach Encourage skills you want to see more often. Discourage behaviors you want to see less.

16
Oppositional behavior
Time-In: Encouraging use of new skill Frequent, intermittent “bursts” of attention to average behavior BIG reaction for demonstrating skill

17
Oppositional Behavior
Time-Out: Discouraging Problem Behavior Misconceptions: Child must be quiet Child must sit still Child must be sorry Child must understand

18
Oppositional Behavior
Time-Out: Discouraging Problem Behavior What it IS: Brief, unpleasant consequence during which there is no access to attention or anything fun

19
Oppositional Behavior
Time-Out: Discouraging Problem Behavior Procedure Adult-sized chair Area easy to covertly monitor 2-3 minutes Parent ends the time-out Child completes task after time-out is over

20
Sleep/Bedtime Problems
Most common: Difficulty settling and night time awakenings

21
Sleep/Bedtime Problems
Basic Intervention: Improved sleep hygiene Systematic ignoring Faded bedtime procedure Reward program

22
Sleep/Bedtime Problems
Basic Intervention: Improved sleep hygiene Systematic ignoring Unmodified (“cold turkey”) With parental presence Quick check Graduated (Ferber)
 With parental presence. Quick check. Graduated (Ferber)")
23
Sleep/Bedtime Problems
Basic Intervention: Improved sleep hygiene Systematic ignoring Faded bedtime procedure Establish time of sleep onset Set “window” of sleep Gradually increase time

24
Sleep/Bedtime Problems
Basic Intervention: Improved sleep hygiene Systematic ignoring Faded bedtime procedure Reward Program

25
Case #2 8 y.o. female with “difficulty sleeping” Questions:
Noncompliant at bedtime Three hour latency to sleep Co-sleeping Questions: How much sleep is the child lacking? How would you set up the faded procedure? What other procedures might you employ?

26
ADHD “Attentional problems” greatest increase of all mental health problems in PC since 1979 ADHD diagnosis a 2.3-fold increase in the population-adjusted rate from Children with ADHD use primary care more, cost more

27
Formal Diagnostic Criteria DSM-IV, 1994
Criterion A: Six or more symptoms from one or both of these lists: Inattentive Type Hyperactive/Impulsive Type …have been present for at least 6 months.

28
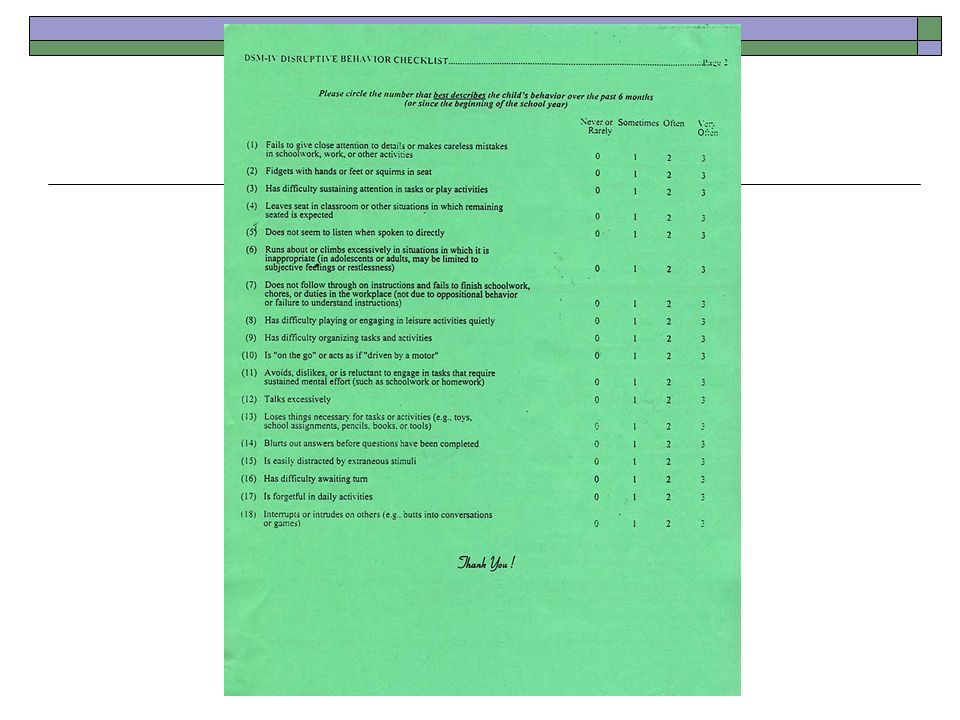
Symptom Lists Hyper/Impulsive Type Inattentive Type
often fidgets hands/feet or squirms often leaves seat when sitting is expected runs about or climbs excessively difficulty playing or engaging in leisure activities quietly often “on the go”/ “driven by motor” talks excessively blurts out answers before questions completed difficulty awaiting turn interrupts or intrudes on others Inattentive Type fails to attend to details, makes careless mistakes difficulty sustaining attention in play or work does not listen when spoken to does not follow through difficulty organizing tasks avoids task requiring sustained mental effort loses things needed distracted by extraneous stimuli often forgetful

29
Formal Diagnostic Criteria DSM-IV, 1994
Criterion B: Some of the symptoms were present before the age of seven years.

30
Formal Diagnostic Criteria DSM-IV, 1994
Criterion C: Some impairment from the symptoms is present in two or more settings (e.g., home, and school or work).
.")
31
Formal Diagnostic Criteria DSM-IV, 1994
Criterion D: There is evidence of clinically significant impairment in social, academic, or occupational functioning.

32
Formal Diagnostic Criteria DSM-IV, 1994
Criterion E: The identified symptoms are not better accounted for by another mental disorder.

33
ADHD: Assessment Information gained by qualified clinician From family
From school Observation

34
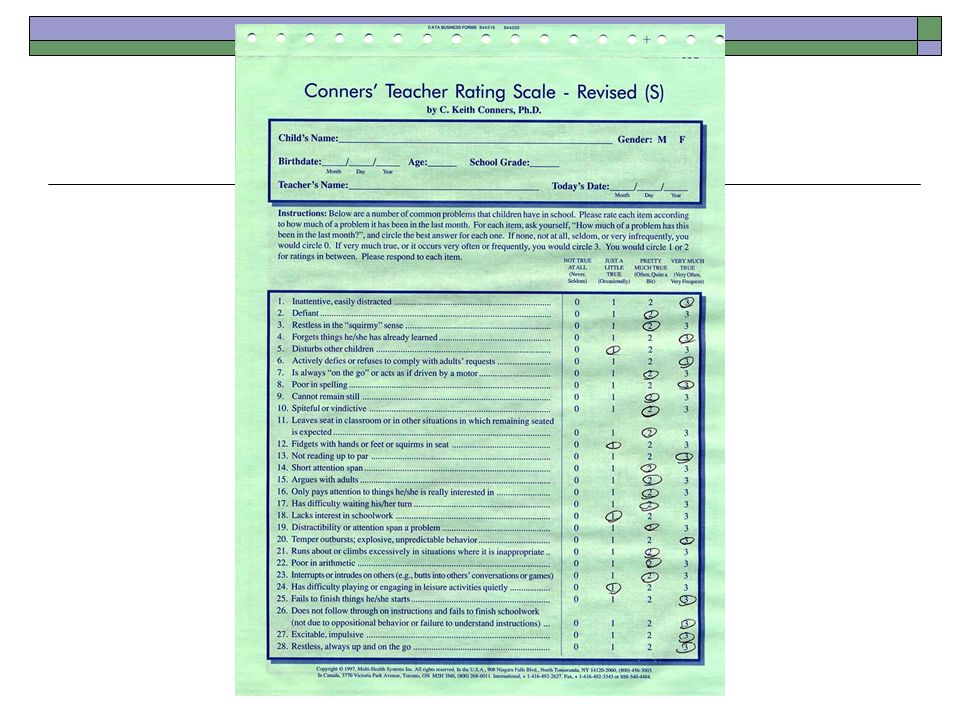
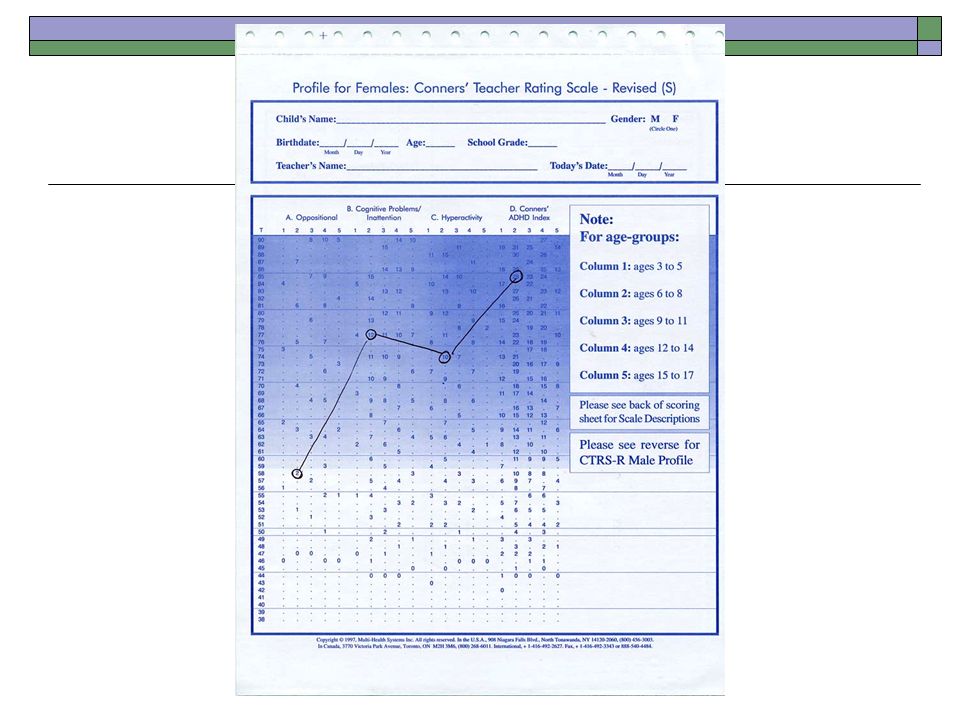
ADHD: Assessment Well-regarded rating scales:
Conners (Parent and Teacher) ADHD Checklist (DSM-IV)
 ADHD Checklist (DSM-IV)")
38
ADHD: Treatment What we KNOW works: Drug Therapy Behavior Therapy
Hundreds of studies (N > 5,000) Behavior Therapy 48 classroom studies (N > 900) 80 parent/home studies (N > 5,000) Combined Behavioral/Drug 10 classroom studies (N > 800)
 Behavior Therapy. 48 classroom studies (N > 900) 80 parent/home studies (N > 5,000) Combined Behavioral/Drug. 10 classroom studies (N > 800)")
39
ADHD: Treatment The AAP Guidelines: Establish management program
Specify target outcomes in cooperation Use medications/behavior therapy Re-evaluate Follow-up systematically

40
ADHD Other information NIH Consensus Statement
AAP Clinical Practice Guidelines (Pediatrics, 2000) AACAP Practice Parameters for the Assessment and Treatment of Children, Adolescents, and Adults with ADHD
 AACAP Practice Parameters for the Assessment and Treatment of Children, Adolescents, and Adults with ADHD.")
Similar presentations





>")
 By: Bianca Jimenez Period:5.>")
. Diagnostic and.>")


 and types of ADHD Basic interventions with ADHD ADHD and the typical comorbidity.>")








