Download presentation
Presentation is loading. Please wait.

1
ED trauma meeting 26 th July 2012 C spine Bonanza

2
Trauma Summary :June Snapshot 114 Alerts 6 Responds 19 Missed activations 2 needed urgent intervention Overall Disposition: ICU 7 OT 7 THDU 10 NHDU2 IR 1 ward35 More than half are admitted; 20% are sick

3
First half 2012 …. so far 2012 728 alerts 46 respond

4
Case 1 I think you call this a clusterf*** 1004917

5
Prehospital Monday 4 th June 08:45 M struck by motorcyclist who lost control of his bike I bone protruding (L) lower leg S alert, HD stable decreased pulses in foot T Ketamine 100mg, morphine 10mg # reduced and splinted, soft collar
 lower leg S alert, HD stable decreased pulses in foot T Ketamine 100mg, morphine 10mg # reduced and splinted, soft collar")
6
Emergency Dept 10:17 Airway & Breathing ✔ Circulation ✔ Disability ✔ Clinically Head, Neck, Abdo & pelvis – fairly unremarkable Predominately lower limb issues: L)leg deformed ankle, sml 2mm open wound neuro/vasc intact R) leg abrasion over medial ankle + lower leg
leg deformed ankle, sml 2mm open wound neuro/vasc intact R) leg abrasion over medial ankle + lower leg")
7
CXR

8
L lower limb

9
Initial ED management

10
Orthopaedic ward 10/5 Physio notes C-spine limited right rotation & lateral flexion (suggest stretches for C-spine) 11/5 C/O pins & needles in R) index + mid fingers Care transferred to plastics 18 th May
 11/5 C/O pins & needles in R) index + mid fingers Care transferred to plastics 18 th May")
11
Plastics ward –18/5 OT: free flap to L) lower leg –19/5 ↓ SpO2 85% RA, seen by ward call –20/5 CTPA : no PE, # 8th rib seen by plastics reg C-spine Xray (to investigate paraesthesiae) ortho review suggesting CT spine (shooting pain shoulder/neck)
 lower leg –19/5 ↓ SpO2 85% RA, seen by ward call –20/5 CTPA : no PE, # 8th rib seen by plastics reg C-spine Xray (to investigate paraesthesiae) ortho review suggesting CT spine (shooting pain shoulder/neck)")
13
CT C-spine

14
Back to orthopaedic ward –22/5 Tertiary Survey XR R) ankle medial malleolus # –26/5 OT ACDF C6-C7 + R) medial malleolus ORIF –13/6 Discharged home Day 28
 ankle medial malleolus # –26/5 OT ACDF C6-C7 + R) medial malleolus ORIF –13/6 Discharged home Day 28")
16
Clinically clearing a C-spine How do you do it?? Do decision rules help??

17
NEXUS 34069 patients (included children) 99% sensitivity Virtually no risk of C-spine injury if: NEXUS criteria met: –No neurology, normal alertness –Not intoxicated –No midline tenderness –No distracting painful injury
 99% sensitivity Virtually no risk of C-spine injury if: NEXUS criteria met: –No neurology, normal alertness –Not intoxicated –No midline tenderness –No distracting painful injury")
18
What is a distracting injury? What does NEXUS say???

19
Canadian C-spine Rule 8924 adult patients 100% sensitivity

20
Now we have decided to do an Xray ……How do we interpret it?

21
Anatomy refresher: C1 anatomy

22
C2 anatomy

23
C4 anatomy

24
Lateral view

25
Adequacy 7 2 3 4 5 6

26
Lines Anterior Vertebral Line

27
Lines Posterior Vertebral Line

28
Lines Spinolaminal Line

29
Lines Posterior Spinous Line

30
Spaces Pre-dental space < 5mm children < 2.5mm adults

31
Soft tissue < ⅓ width of C2 < full width of C7

32
Peg view

33
Check bony landmarks

34
Symmetry of lateral dens space

35
Check the lateral tips of C1

36
Some abnormal C spines

41
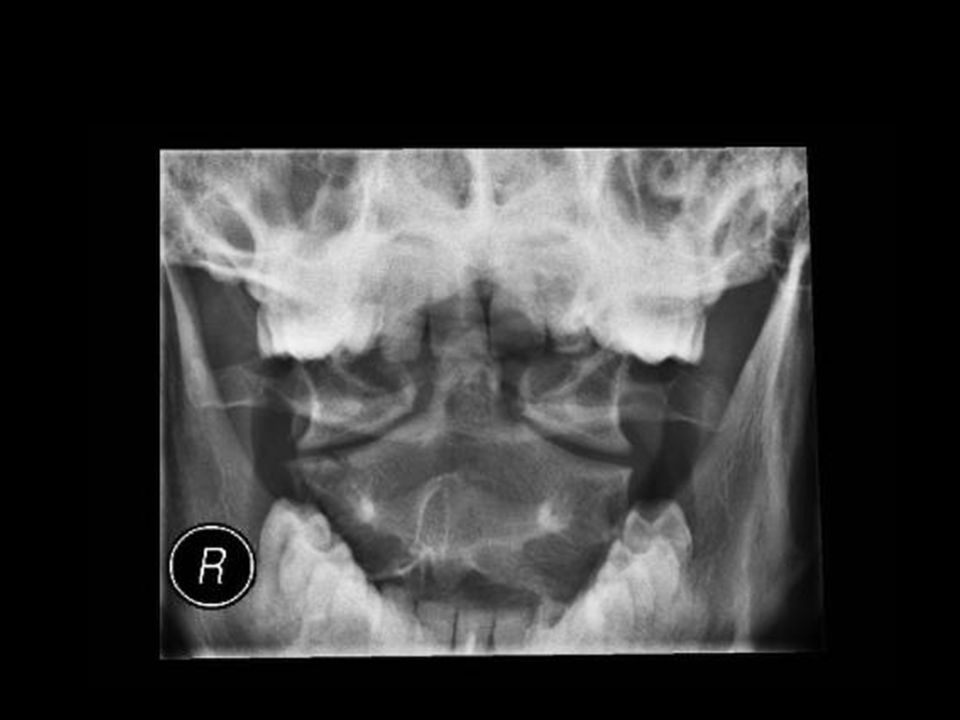
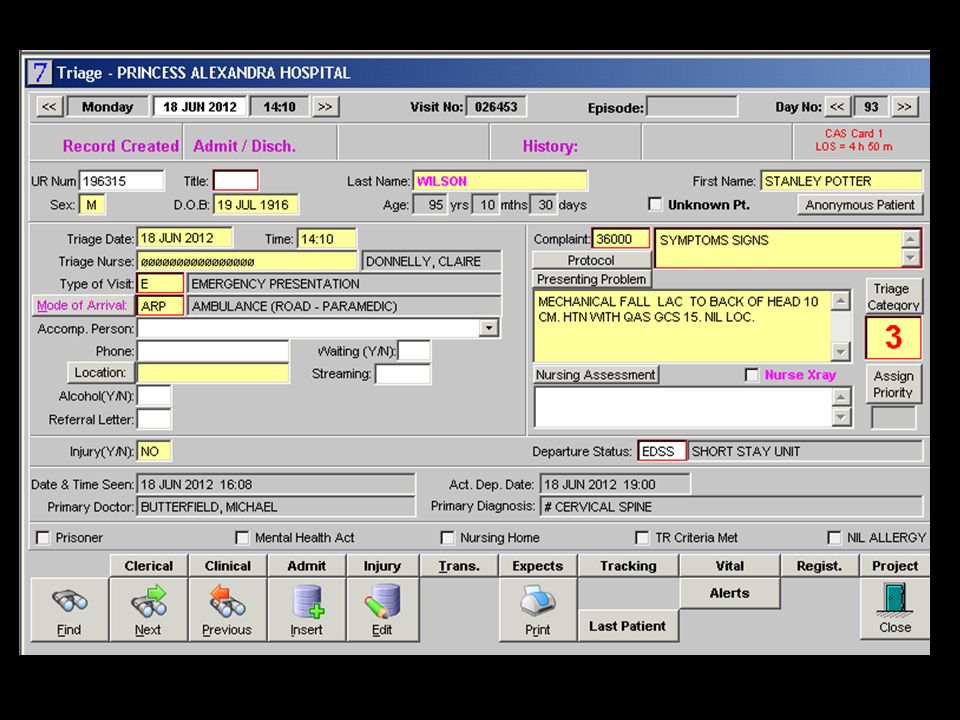
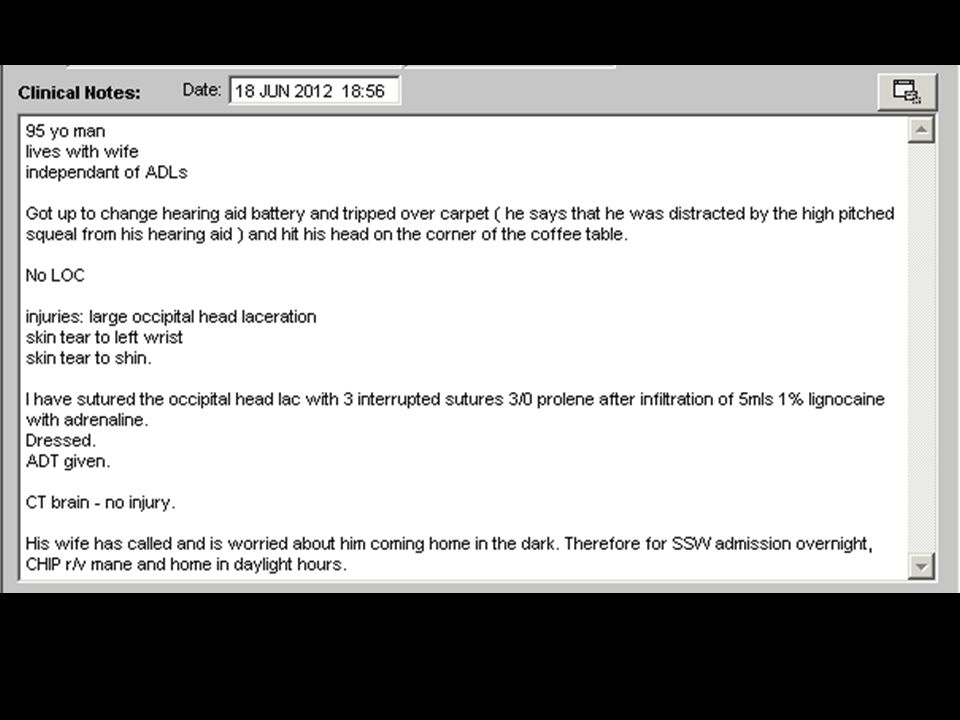
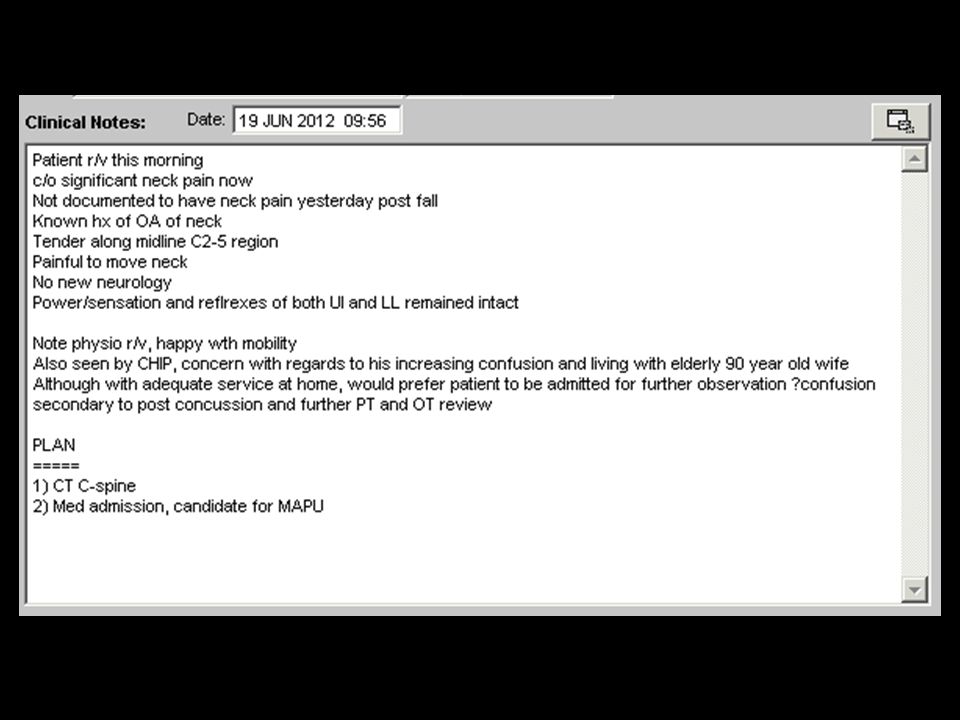
Case 2 Thank God for Short Stay 196315

44
CT head

48
CT C-spine

51
Issues Old people break stuff look for it Good news is they hardly ever have to do anything about it

52
Case 3 Silly people break things too 816340

53
Prehospital Monday 4 th June 18:02

54
Emergency : Resus 4 Primary survey ✔ –C-spine nil central tenderness (ETOH on board) –Mild abrasions to L shoulder –CXR & C-spine NAD
 –Mild abrasions to L shoulder –CXR & C-spine NAD")
55
CXR

56
C-spine

57
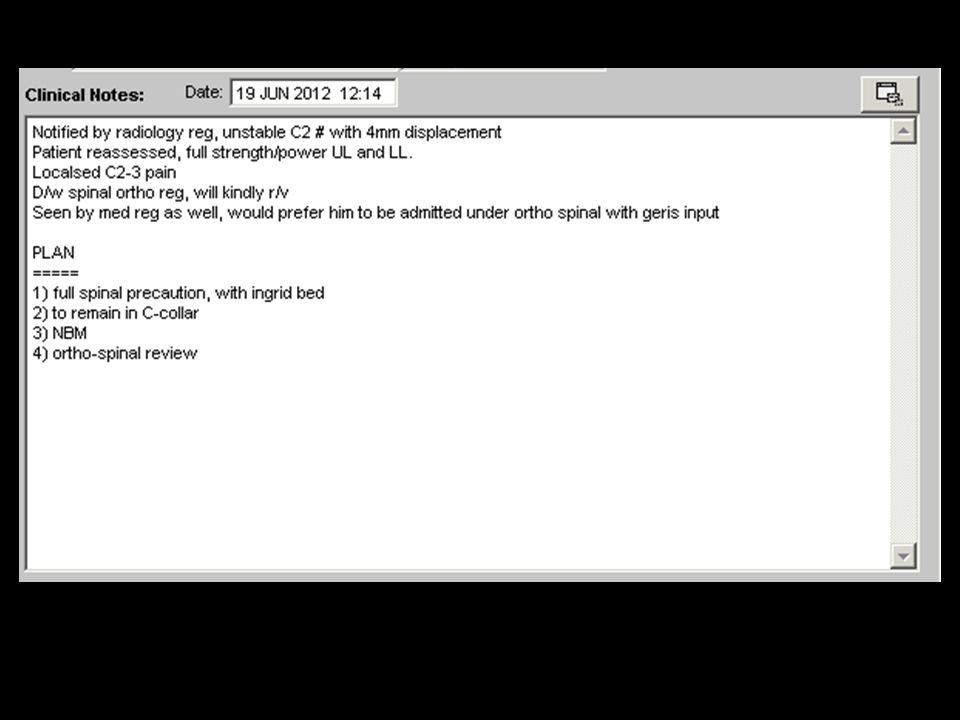
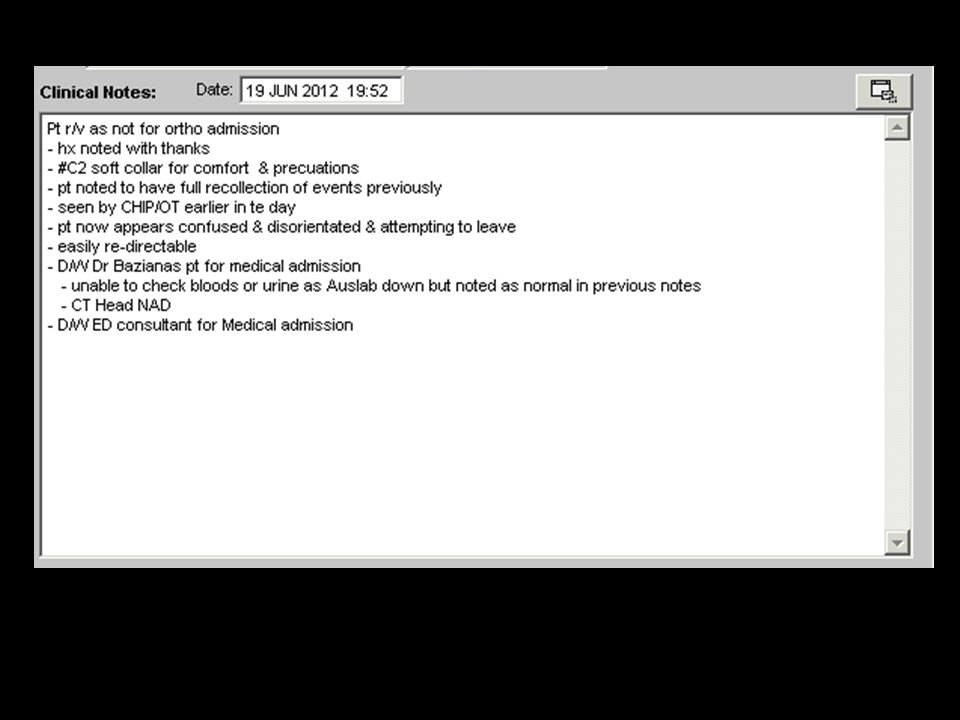
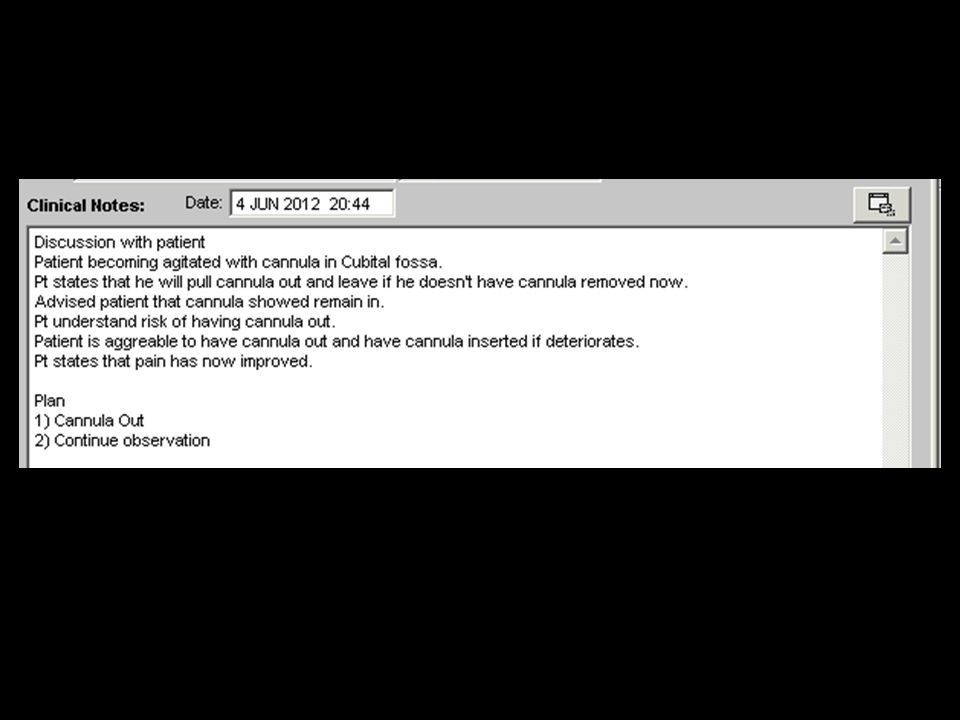
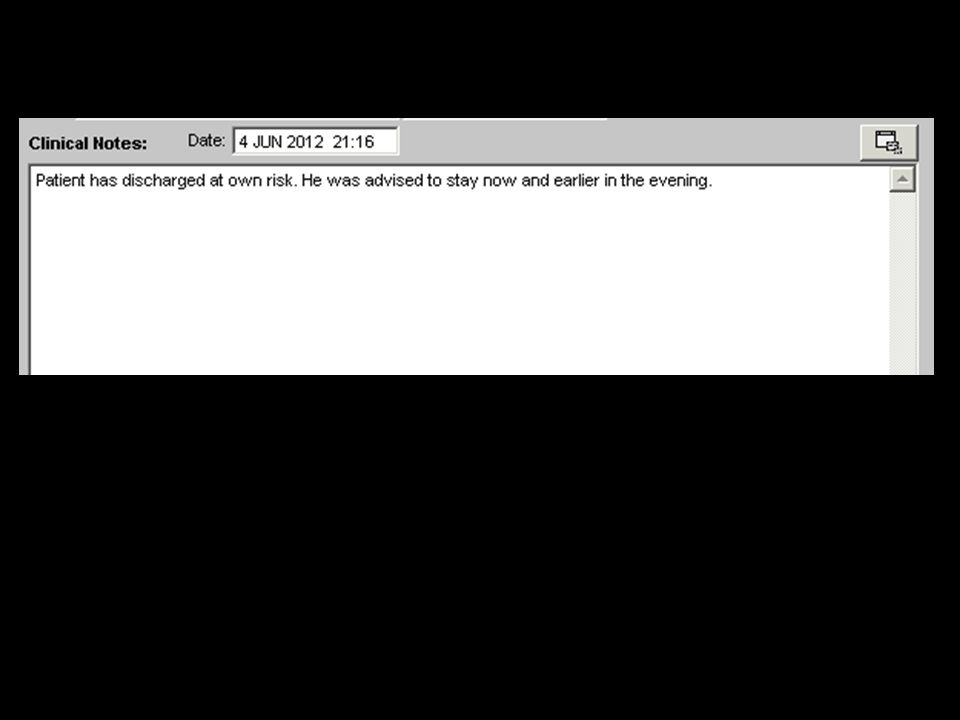
Our Plan

60
What do you do??

61
Represents

62
What next?

63
CT result

64
Outcome Orthopaedic admission Rest of spine imaged on the ward –T 12 anterior wedge # –Free fluid in pelvis Halo brace fitted, discharged d4

65
Issues raised The intoxicated patient has an unreliable examination If you order tests make sure you check them in a timely fashion If you find a spinal # look for more DOCUMENTATION!!!

Similar presentations











>")














