Download presentation
Presentation is loading. Please wait.

1
VCU DEATH AND COMPLICATIONS CONFERENCE

2
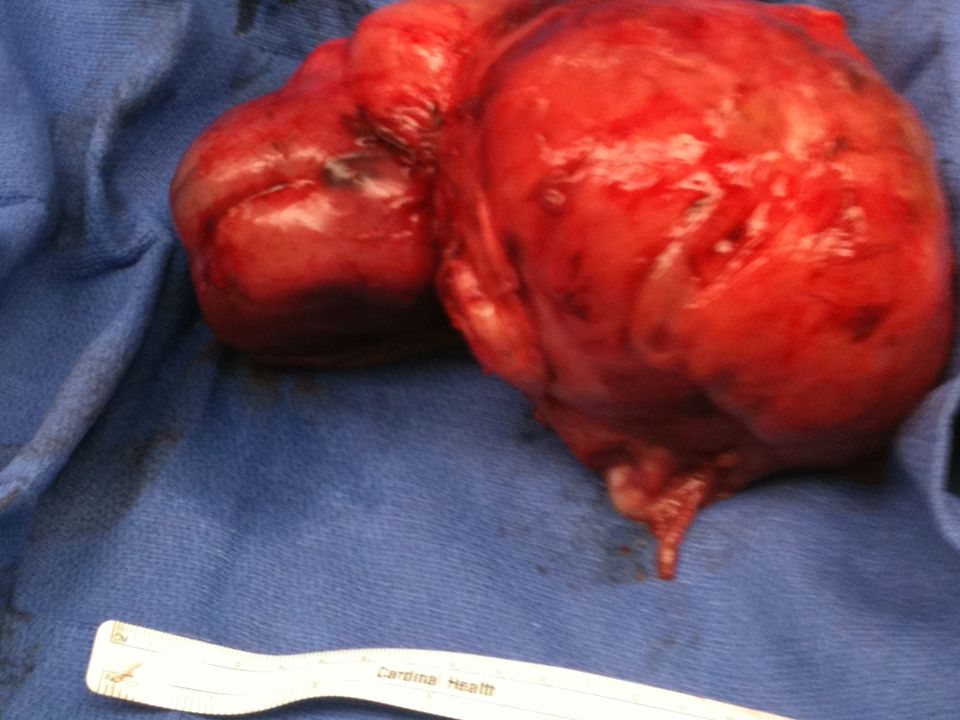
Introduction Complication Death, coagulopathy Procedure Partial resection of massive intraabdominal tumor Primary Diagnosis Sarcoma NOS

3
Clinical History 2 yo girl from Honduras Large intraabdominal tumor PMH seizure disorder Mass diagnosed at age 6 months s/p 2 resections/biopsies, 6 cycles chemo Multiple working tumor diagnoses, multiple pathologists Admitted 3/1 for imaging, hyperalimentation Stepdown status for refeeding syndrome Heme-onc and nutrition consults Outside path specimens reviewed at MCV

4
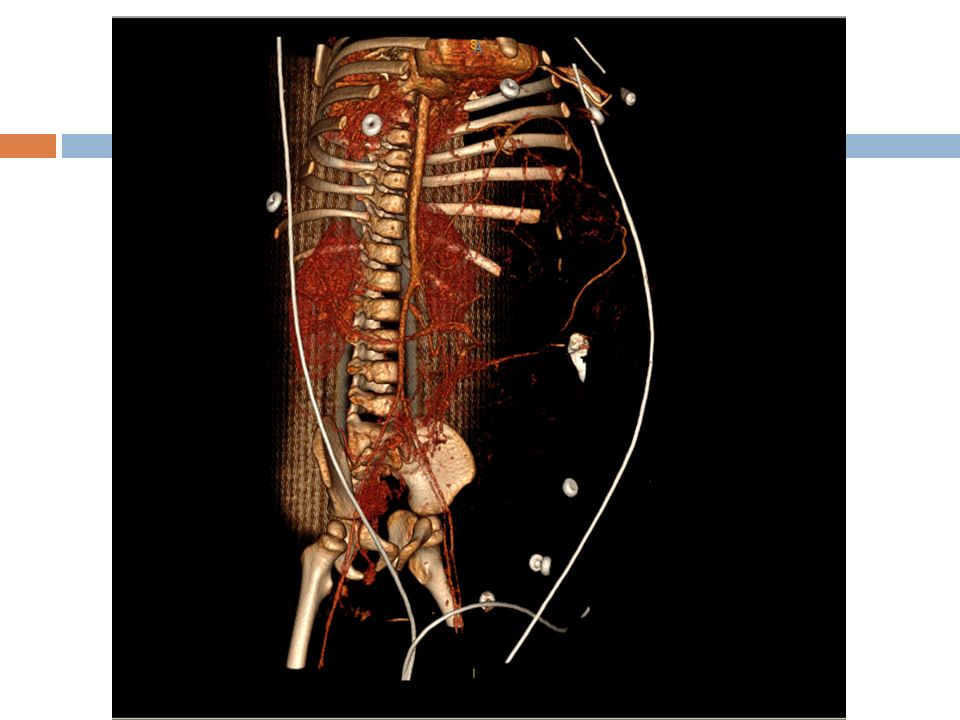
Timeline of Key Events 3/2 To OR for R brachial PICC line, CT abdomen 3/5 PICC adjustment by IR, placement of R IJ PICC CTA abdomen/pelvis MRI head 3/6 OR for resection

9
Intraoperative events Transverse abdominal incision made over mass Transverse colon mesentery dramatically stretched Anatomy grossly distorted Dissection proceeded on left lobule Left sided masses removed x 2 after reduction of transverse colon Perforation noted near pylorus, mass origin Distal gastrectomy, cholecystectomy

11
Intraoperative events Intraoperative TEE Sinus bradycardia @ 1209 Loss of pulse @ 1219, chest compressions Ventricular fibrillation 1247, shock x 2 (30J, 50J) Intraoperative TEE revealed collapsed RV Decision made to close abdomen and transfer to ICU for rewarming, resuscitation and correction of coagulopathy
 Intraoperative TEE revealed collapsed RV Decision made to close abdomen and transfer to ICU for rewarming, resuscitation and correction of coagulopathy")
12
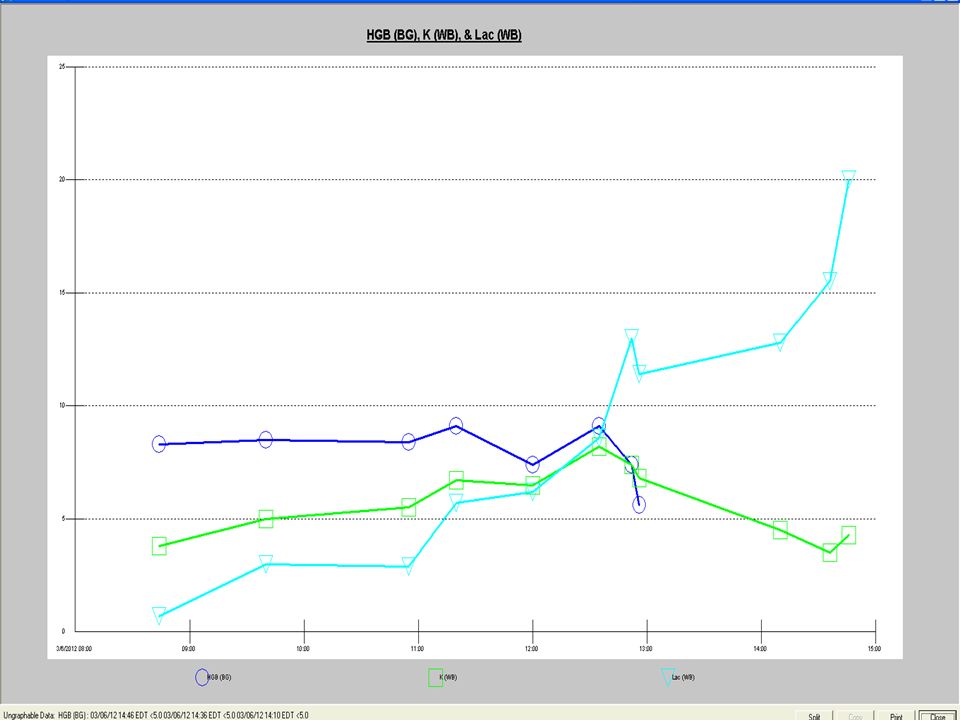
Postoperative events Transferred to ICU hyperkalemic (6.8), temp of 35, coagulopathic, anemic (5.6), lactate 11.4, acidotic (7.08) Coded again within 1 hour of arrival to PICU ACLS again initiated, ultimately pupils fixed and dilated, continued hemorrhage from abdomen
, temp of 35, coagulopathic, anemic (5.6), lactate 11.4, acidotic (7.08) Coded again within 1 hour of arrival to PICU ACLS again initiated, ultimately pupils fixed and dilated, continued hemorrhage from abdomen")
14
Facts and failures Platelets checked at 1125 (45) with coags (INR 3), fibrinogen ( 20) Intraoperative temperature range 30.8 – 36.8 C Bair hugger reportedly on 43 deg C TEG done at 1125 revealed DIC with low platelet function/count and low fibrinogen Coags and fibrinogen unchanged on arrival to PICU 3 hours later Massive transfusion protocol never initiated
 with coags (INR 3), fibrinogen ( 20) Intraoperative temperature range 30.8 – 36.8 C Bair hugger reportedly on 43 deg C TEG done at 1125 revealed DIC with low platelet function/count and low fibrinogen Coags and fibrinogen unchanged on arrival to PICU 3 hours later Massive transfusion protocol never initiated")
15
Facts Totals for case EBL 800 cc 1850 cc PRBC 1100 cc NaCl 0.9% 583 FFP 100 U cryoprecipitate 500 cc albumin 200 cc TPN

16
Analysis of Complication Was the complication potentially avoidable? – Yes. Could have elected not to resect, or simply to biopsy for additional stains/markers. Could have had better communication with anesthesia regarding intraoperative resuscitation status. Would avoiding the complication change the outcome for the patient? – Yes. What factors contributed the complication? – Lack of communication between surgery and anesthesia, size of tumor, extensive dissection and distortion of anatomy, release of inflammatory mediators, nutritional status.

17
Contributing problems Poor planning Distorted anatomy Grossly disturbed physiology Inadequate resuscitation Factor deficiencies, hemodilution Ineffective communication

18
Final Pathology

Similar presentations







-Score: Probability of Mass Transfusion as Surrogate for Life Threatening Hemorrhage after Multiple Trauma The.>")






 I am encouraged by my colleagues to report any patient safety concerns.>")







