Download presentation
Presentation is loading. Please wait.

1
AAAAAAAAAAAAAAA ENDOMYOCARDIAL BIOPSY Claudio Moretti School of Cardiology - University of Turin Department of Medicine Turin-Asti - Italy Claudio Moretti School of Cardiology - University of Turin Department of Medicine Turin-Asti - Italy

2
ENDOMYOCARDIAL BIOPSY 1. STONE AGE ENDOMYOCARDIAL BIOPSY 1. STONE AGE NEEDLE BIOPSY

3
2. FIRST “JAP” ENDOVASCULAR ATTEMPTS 1962 – SAKAKIBARA AND KONNO Introduced a transvascular approach to obtaining endomyiocadial tissue. The device was so large that access to a vessel was difficult. One series of over 450 pts in Japan underwent the procedure without complication.

4
2. THE EUROPEAN SCHOOL (early ‘70) A modified bronchoscope biopsy forceps is introduced transvascularly for either right or left ventricle biopsy.
 A modified bronchoscope biopsy forceps is introduced transvascularly for either right or left ventricle biopsy..")
5
3. THE AMERICAN SCHOOL (mid-1970s) Developed by Caves et al for assessment of cardiac rejection
 Developed by Caves et al for assessment of cardiac rejection")
6
4. TODAY 50% sharper, straight or radial tip, 50 - 104 cm. Tissue sample 5.03 mm 3

7
EMB: tips & tricks Central vein puncture RV_EMB / Jugular approach RV EMB / Femoral approach

8
Patient positioning 1.Trendelemburg 2.Do not over-rotate 3.Valsalva ?

9
POINT OF CARE ECHO ultrasound-guided central line one of the "Top 11 Highly Proven A 2001 Agency for Healthcare Research and Quality report listed ultrasound-guided central line placement as one of the "Top 11 Highly Proven" patient safety practices not routinely used in clinical practice

10
RV_ EMB: THE TECHNIQUE (jugular approach)
")
11
A.P. view L.A.O view

12
Femoral approach

13
A.P. VIEW L.A.O. VIEW

15
EMB: COMPLICATIONS Single-centers experiences Repetitive procedures after H.TX Largest series reported by Holzmann et al 3048 RV.EMB - 0,12% major complications 3048 RV.EMB - 0,12% major complications 0,28 – 3.3 %

16
“ further investigations are necessary to prove the procedural risk and diagnostic value of the procedural risk and diagnostic value of LEFT VS RIGHT EMB ”. LEFT VS RIGHT EMB ”. 2007 AHA/ACC/ESC The role of EMB in the management of CV disease 2007 AHA/ACC/ESC The role of EMB in the management of CV disease

17
PROCEDURAL SAFETY DIAGNOSTIC PERFORMANCE SELECTIVE OR BIV. EMB SUSPECTED MYOCARDITIS STATE OF THE ART TECHNIQUE

18
SETTING 2 UNIVERSITY HOSPITALS EXPERIENCED INTERVENTIONALISTS (> 3 yrs exp) 755 pts (529 + 226) NO F.up. EMB, NO Heart TX follow up PRE-POST ECHO 71.5 % CMR (no edema-detect seq)
.")
19
POPULATION 265 SELECTIVE LEFT EMB 133 SELECTIVE RIGHT EMB 357 BIVENTRICULAR EMB

20
LV_ EMB 7F Cordis sheath 2.500 Heparin (ACT 150 sec) 7F guiding cath (JR 4, AL 1, JL 4) inferior, posterior, lateral and apical EMB with JR4 anterior segments with AL 1
 7F guiding cath (JR 4, AL 1, JL 4) inferior, posterior, lateral and apical EMB with JR4 anterior segments with AL 1")
21
MAJOR COMPLICATIONS 6361 EMBs 755 PTS (622 left EMB & 490 right EMB) 2 PERFORATIONS 2 STROKES 0.64 4 PERFORATIONS 0.82 BIV. EMB 1.51 MINOR COMPLICATIONS 14 PERICARDIAL EFFUSIONS + 1 TEMP P.M.

22
DIAGNOSTIC PERFORMANCE Which EMB approach gives the highest nr of diagnostic results ? BIVENTR. EMB VS LEFT VENTR. EMB + 7,1 % BIVENTR. EMB VS RIGHT VENTR. EMB + 12,6 %

23
DIAGNOSTIC RELEVANCE of a CMR-Guided EMB CMR has been proposed as a tool to direct EMB Surprisingly, in 292 pts with biventr EMB / CMR_LGE + NO differences in the number of diagnostic EMBs when related to The site of LGE

24
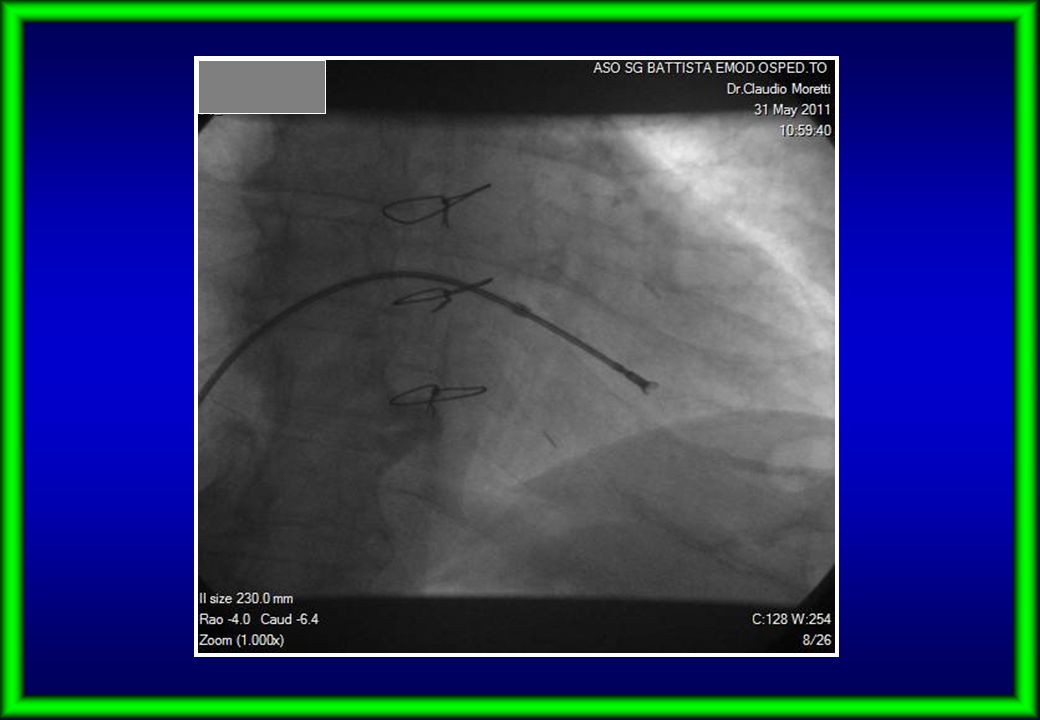
Although the pathological demonstration of myocardial degeneration and fibrofatty replacement is regarded as the diagnostic “gold standard,” EMB has not been consistently helpful in recognizing the disease partly owing to its patchy nature and lack of histological abnormalities at early stages 2011

27
FINAL REMARKS COMPLICATION RATE of 0.64% (LV) AND 0,82% (RV) COMPLICATION RATE of 0.64% (LV) AND 0,82% (RV) I.E. LV/RV EMB IS A SAFE PROCEDURE I.E. LV/RV EMB IS A SAFE PROCEDURE DIAGNOSTIC EMB RESULTS WERE OBTAINED MORE OFTEN IN BI-V EMBs (79,3%) COMPARED TO SELECTIVE OFTEN IN BI-V EMBs (79,3%) COMPARED TO SELECTIVE LV- OR SELECTIVE RV- (67.3%) LV- OR SELECTIVE RV- (67.3%) NO DIFFERENCES IN NR OF DIAGNOSTIC EMBs WHEN RELATED TO THE SITE OF CMR-BASED LGE WHEN RELATED TO THE SITE OF CMR-BASED LGE LV-EMB SHOULD BE PREFERRED IF MINIMIZING THE LENGHT OF THE PROCEDURE IS A CONSIDERATION LENGHT OF THE PROCEDURE IS A CONSIDERATION (HIGHER DX YIELD AND LOWER RISK !) (HIGHER DX YIELD AND LOWER RISK !)
 COMPARED TO SELECTIVE OFTEN IN BI-V EMBs (79,3%) COMPARED TO SELECTIVE LV- OR SELECTIVE RV- (67.3%) LV- OR SELECTIVE RV- (67.3%) NO DIFFERENCES IN NR OF DIAGNOSTIC EMBs WHEN RELATED TO THE SITE OF CMR-BASED LGE WHEN RELATED TO THE SITE OF CMR-BASED LGE LV-EMB SHOULD BE PREFERRED IF MINIMIZING THE LENGHT OF THE PROCEDURE IS A CONSIDERATION LENGHT OF THE PROCEDURE IS A CONSIDERATION (HIGHER DX YIELD AND LOWER RISK !) (HIGHER DX YIELD AND LOWER RISK !).")
28
Thanks a lot !

Similar presentations





 is characterized by.>")




>")







 and Restrictive cardiomyopathy (RCM) share several clinical, ultrasonographic and hemodynamic.>")
