Download presentation
Presentation is loading. Please wait.

1
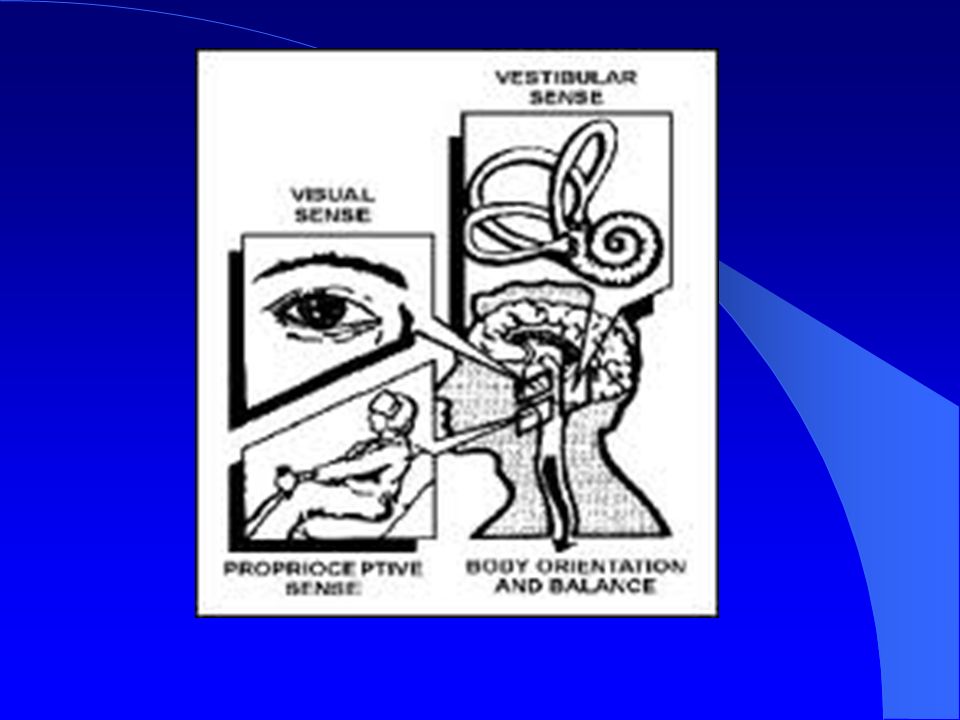
Rethinking Dizziness The Role of Vision, Utricle, and Saccule
Arthur Rosner, MD FACS Debby Feinberg, OD Mark Rosner, MD FACEP

2
John Kemink MD,

3
Shiro Fujita Listen to the Patient

4
How it Started

5
Current Diagnosis Failure to compensate Non-vertiginous dizziness
Mal debarquement syndrome Mall patient Visual vertigo dyslexia

6
Current diagnosis Vestibular Migraine Vomiting with anesthesia
Motion sickness Central vertigo Neck pain Anxiety

7
Current diagnosis Meniere’s Disease Agoraphobia
Bilateral vestibular loss Vomiting on VNG

8
Prevalence 4% of my practice has binocular vision dysfunction
Over 8000 patients have been treated Optometrists now trained in other states

9
Vertical Heterophoria
A condition where one eye sees the image higher than the other eye. The brain is intolerant of the unclear image, and forces the eyes to attempt to create a clear image. The strain on the visual system causes symptoms that mimic conditions such as sinusitis, inner ear disorders and migraines.

11
History Von Graefe. A Uber musculaire Asthenopic. Arch Opthal 1862;8: Doble J, Rosner M, Feinberg D, Rosner A , Identification of Binocular Vision Dysfunction (Vertical Heterophoria) in Traumatic Brain Injury Patients and Effects of Individualized Prismatic Spectacle Lenses in the Treatment of Postconcussive Symptoms: A Retrospective Analysis2010 PMR 2010;2:
 in Traumatic Brain Injury Patients and Effects of Individualized Prismatic Spectacle Lenses in the Treatment of Postconcussive Symptoms: A Retrospective Analysis2010 PMR 2010;2:")
12
Transient Diplopia or Blurred Vision
Thierry M. Using Prism Graphics. Detroit Free Press. August 2, 2005.

13
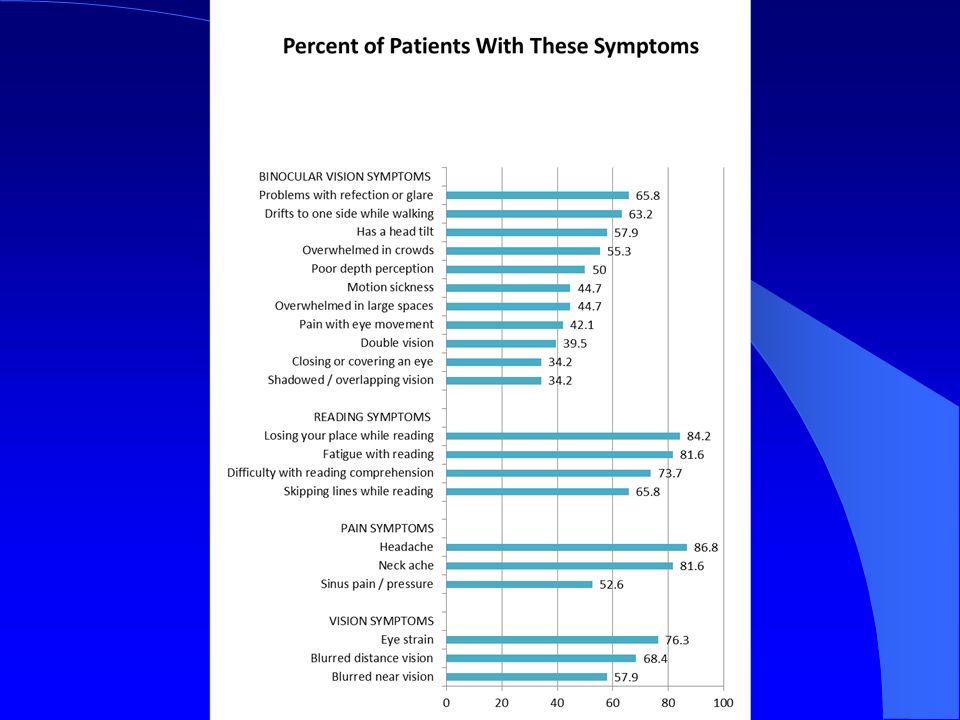
Symptoms Dizziness Headache Head Tilt Nausea Agoraphobia Anxiety
Motion sickness Unsteady while walking Problems reading Thierry M. Using Prism Graphics. Detroit Free Press. August 2, 2005.

14
Anxiety Symptoms Associated with Dizziness
The multiple objects in a large space can overload the visual system and trigger a dizzy episode. The resultant feeling is one of being overwhelmed and anxious. Overwhelmed in big box stores, malls, supermarkets, sports arenas, stadiums, theatres Anxious in crowds, school assemblies

15
Trigeminal nerve

16
Trigeminal nerve

17
Otolaryngology Examination
Head Tilt Vertical and horizontal disparity between the eyes Convergence insufficiency Duplication of symptoms on eye movements Thierry M. Using Prism Graphics. Detroit Free Press. August 2, 2005.

19
Study Design Otolaryngology examination
Pre-treatment Vertical Heterophoria Symptom Questionnaire (VHSQ) Optometry examination Eyeglasses with corrected prescription including vertical and horizontal prism Post-treatment VHSQ
 Optometry examination. Eyeglasses with corrected prescription including vertical and horizontal prism. Post-treatment VHSQ.")
20
Inclusion and Exclusion Criteria
100 patients sent for optometry evaluation 60 patients seen by the optometrist 39 patients filled out pre and post questionnaires 29 patients with vertical heterophoria treated with prism

21
Demographics Number of patients from the study group Female 25 Male 4
Number of patients from the study group Female 25 Male 4 Prior prescription eyeglasses Trouble adjusting to prior eyeglasses 9 Prior history of eye muscle imbalance or prior prism Migraine history 7 Concomitant benign paroxysmal positional vertigo at initial office visit, which resolved with Eply maneuver

22
Chief Complaint on Presentation to the Otolaryngologist
Number of patients with a chief complaint of dizziness Number of patients with a chief complaint of sinus headache Number of patients with a chief complaint of both dizziness and headache At initial presentation 16 7 6 Results from questionnaire before treatment 1 21

23
Number of patients from the study group MRI of the head 8 All normal except for minimal mucosal thickening CT scan of the head 6 All normal except for minimal mucosal thickening Audiogram total 9 Audiogram normal 5 Bilateral symmetrical low frequency sensorineural hearing loss 1 Bilateral symmetrical high frequency sensorineural hearing loss 2 Asymmetric high frequency sensorineural hearing loss with normal MRI Elecronystagmogram total 6 Elecronystagmogram normal 4 Elecronystagmogram abnormal 2 abnormal optokinetic nystagmus

24
Optometry Evaluation Functional Vision Tests Average Results
Range of Results Expected Findings Vertical Distance Phoria .5PD base-up left eye 0-1.5 PD base-up left eye Ortho or 0 Vertical Near Phoria 1PD base-up left eye 1 PD base-down left eye-3.5PD base-up left eye Vertical Vergence at Near 4 PD/2PD base up left eye 2PD/0PD base down left eye 4PD/1PD base up left eye; 5PD/1PD base down left eye - 7PD/4PD base up left eye; Break: 3-4 PD Recovery: PD

25
Trial Frame

26
Trial Framing Dynamic process between patient and doctor
Quarter unit prism lenses are required Time needed between adjustments to allow muscles in eyes and neck to relax Prescription modified based on the patients response Needs to be learned in person

27
Prescription Before Treatment After Treatment Patients with bifocals
10 27 Patients with myopia 18 19 Patients with hyperopia 5 9 Patients with astigmatism Patients with glasses 25 29 Patients with vertical prism to correct a high left eye and horizontal base-in prism

28
Statistics Likert scale 0 = Never 1 = Occasionally 2 = Frequently
3 = always Paired t-test before and after treatment For each question Total questionnaire score

29
Optometric Examination
Standard optometric exam Phoria testing, vertical vergence, and Maddox rod tests do not predict the need for prism, amount of prism or direction of prism

30
Rank Question P Value Mean difference after treatment 1 Do you experience dizziness, light-headedness, or nausea associated with bending down then standing back up quickly from a seated position? < .0001 .8271 2 Do you blink to “clear up” distant objects after working at a desk or with near centered tasks? 3 Do you feel unsteady with walking? .758 4 Do you tire easy with reading? < .0014 .724 5 Do you experience poor depth perception or have difficulty estimating distances accurately? < .002 .62

31
Rank Question P Value Mean difference after treatment 6 Does print blur after reading a short time? < .002 .62 7 Do you skip lines or lose your place while reading (using your finger or other guide to maintain position on the page)? .625 8 Do you tilt your head to one side when reading or working at a desk? 9 Do you experience dizziness, light-headedness, or nausea associated with close-up activities (i.e., reading, writing, computer work)? < .0088 .552 10 Do you experience words running together with reading? < .0090 .379
 Do you tilt your head to one side when reading or working at a desk 9. Do you experience dizziness, light-headedness, or nausea associated with close-up activities (i.e., reading, writing, computer work) < Do you experience words running together with reading <")
32
Rank Question P Value Mean difference after treatment 11 Do you feel overwhelmed while walking in a large department store (i.e., K-mart, Meijer)? < .0108 .552 12 Do you experience double vision or overlapping vision at far? < .0136 .379 13 Do you experience blurred vision with close-up activities (i.e., reading, writing, computer work, sewing)? < .0208 14 Do you experience dizziness, light-headedness, or nausea associated with far distance activities (i.e., driving, television, movies)? < .0252 .448 15 Do you experience blurred vision with far-distance activities (i.e., driving, television movies, chalkboard at school)? < .0298
 < Do you experience double vision or overlapping vision at far < Do you experience blurred vision with close-up activities (i.e., reading, writing, computer work, sewing) < Do you experience dizziness, light-headedness, or nausea associated with far distance activities (i.e., driving, television, movies) < Do you experience blurred vision with far-distance activities (i.e., driving, television movies, chalkboard at school) <")
33
Rank Question P Value Mean difference after treatment 16 Do you cover one eye while reading? < .0365 .310 17 Do you have headache and/or facial pain? < .053 .517 18 Do you hold reading material too close to your eyes? < .0572 .345 19 Do you avoid close up tasks? (reading, writing, computer work) < .0668 20 Do you experience double vision or overlapping at near distance? < .1095 .241
 < Do you experience double vision or overlapping at near distance <")
34
Rank Question P Value Mean difference after treatment 21 Do you have pain in your eyes with movement? < .3053 .172

35
Aggregate Results Lowest Score Highest Score Average Score
Lowest Score Highest Score Average Score Pre-Treatment Questionnaire Score 7 47 21.5 Post-Treatment Questionnaire Score 30 10.5 Difference in questionnaire score Pre-treatment to Post-treatment 11.0 P< .0001

36
Conclusions Vertical Heterophoria is a syndrome
Treatment with fractional units of horizontal and vertical prism significantly reduces patient symptoms p< .0001 VHSQ seems to be a useful tool to identify VH suspects and measure improvement

37
Symptoms Most Improved
Dizziness on bending down and standing up Blinking to clear up distant objects Unsteadiness when walking Fatigue with reading Poor depth perception

39
Vertical Heterophoria in Children

41
Pediatric Study Design
Retrospective study of pediatric patients comparing and contrasting to adult population

42
Pediatric Patient Analysis
2/16/05 thru 3/25/06 33 children 9 lost to f/u 3 non-compliant (refused to wear glasses) 21 children with complete data 7 yo – 17 yo, avg 10.4 yo 11 boys, 10 girls 8 previous eye glass wearers / 14 not
 21 children with complete data. 7 yo – 17 yo, avg 10.4 yo. 11 boys, 10 girls. 8 previous eye glass wearers / 14 not.")
43
PMHx / ROS Headaches = 14 pts Dizziness = 7 Motion sickness = 6
Nausea = 6 Tires with reading = 6 Skips lines with reading = 6 ADHD / ADD = 5 Head tilt = 4 Double vision = 2 Anxiety = 2

44
Prescription Results Farsighted = 17 Nearsighted = 4
Pediatricians only routinely test for nearsightedness 20 out of 21 needed prism 20 out of 21 needed bifocal

45
VHSQ Results Pre-treatment VHSQ score avg = 17.9 (range 2-47)
Post-treatment VHSQ score avg = 6.9 (range 1-17) Normality tests – distribution of differences are normally distributed Pre-treatment VHSQ is significantly higher than post-treatment VHSQ score (p<0.0001, using Student’s t-test) Implies that treatment is effective
 Normality tests – distribution of differences are normally distributed. Pre-treatment VHSQ is significantly higher than post-treatment VHSQ score (p<0.0001, using Student’s t-test) Implies that treatment is effective.")
46
Vertical Heterophoria
Children and adults both have: Headaches and Dizziness as the primary symptoms History of motion sickness Difficulty with near point tasks and comprehension

47
Impact on School Experience
Unable to maintain attention on near tasks for prolonged periods: Computer and reading difficulty

48
Vertical Heterophoria
Compared to adults, children have: Lower VHSQ scores, Pre-treatment and post-treatment Less need for spectacle prescription modifications Less anxiety More farsightedness

49
Headaches “Head hurts”
Tend to be worse at the end of school days, better on weekends Frontal, periorbital, temporal, crown, occipital

50
Visual Causes of Dizziness
Riding in a car Reading in a car Swinging on swings Spinning rides at fair Postural changes Bending down and coming up quickly Standing quickly from seated or prone position

51
Problems With Depth Perception
Binocular vision critical for depth perception Lack of binocularity causes symptoms: Feel klutzy and / or uncoordinated Walk into friends when walking beside them Fall often Difficulty with catching a ball Bumps into door jambs and furniture

52
Vertical Heterophoria in Traumatic Brain Injury Patients

53
Patients 83 patients sent for testing
77 positive for vertical heterophoria syndrome 43 had complete data

54
Specialists Seen (78 patients): 3. 25 specialists / patient
Specialists Seen (78 patients): specialists / patient range: 0-9 specialists / patient IM or FP 64% Ophtho or Opto 60% Neuro 47% ENT 43% Chiropractor 35% PM&R 23% Psych 21% ER 10% Peds 0.5%
: 3.25 specialists / patient range: 0-9 specialists / patient. IM or FP 64% Ophtho or Opto 60% Neuro 47% ENT 43% Chiropractor 35% PM&R 23% Psych 21% ER 10% Peds 0.5%")
55
Tests Performed (78 patients): 1. 27 tests / patient
Tests Performed (78 patients): tests / patient range: 0-4 tests / patient Brain MRI 43% HCT 42% Pt had either had a HCT or MRI 57% Had both HCT and MRI 27% Audiogram 22% ENG 21%
: 1.27 tests / patient range: 0-4 tests / patient. Brain MRI 43% HCT 42% Pt had either had a HCT or MRI 57% Had both HCT and MRI 27% Audiogram 22% ENG 21%")
56
Top 10 Symptoms VHSQ questions ranked by number of # of positive responders AND frequency of symptoms: (1) 3. Shoulder and neck discomfort (2) 1. Headache (3) 17. Glare / sensitivity to bright lights (4) 4. Dizzy / lightheaded (5) 8. Unsteady / drift to one side (6) 11. Car rides = uncomfortable / dizzy (7) 7. Dizziness with provocative head movements (8) 13. Head tilt (9) 20. Tire easily with close-up tasks (10) 23. Blink to clear up distant objects
 3. Shoulder and neck discomfort. (2) 1. Headache. (3) 17. Glare / sensitivity to bright lights. (4) 4. Dizzy / lightheaded. (5) 8. Unsteady / drift to one side. (6) 11. Car rides = uncomfortable / dizzy. (7) 7. Dizziness with provocative head movements. (8) 13. Head tilt. (9) 20. Tire easily with close-up tasks. (10) 23. Blink to clear up distant objects.")
57
Retrospective Data Analysis of 43 TBI Patients with VH Retrospective
Avg Age Initial VHS-Q score Final VHS-Q Score Subjective % Improved 44 M = 12 F = 31 35 18.3 (47.5% reduction) 72% 57 57
 72%")
58
Average duration of symptoms (years) 3.6 yrs 2
Study 2: TBI Study Number of Patients 43 Mean Age (years) 44 Female Gender 72% 1 Average duration of symptoms (years) 3.6 yrs 2 Average duration of treatment (months) 3.5 mos VHSQ Score (VH Symptom Burden): Initial 34.8 Final 18.1 3 Reduction with treatment 48% 6 Average subjective improvement with Prismatic Lens Treatment using numeric rating scale (Subjective Improvement %) 71.8% 58
 44. Female Gender. 72% 1. Average duration of symptoms (years) 3.6 yrs. 2. Average duration of treatment (months) 3.5 mos. VHSQ Score (VH Symptom Burden): Initial Final Reduction with treatment. 48% 6. Average subjective improvement with Prismatic Lens Treatment using numeric rating scale (Subjective Improvement %) 71.8% 58.")
61
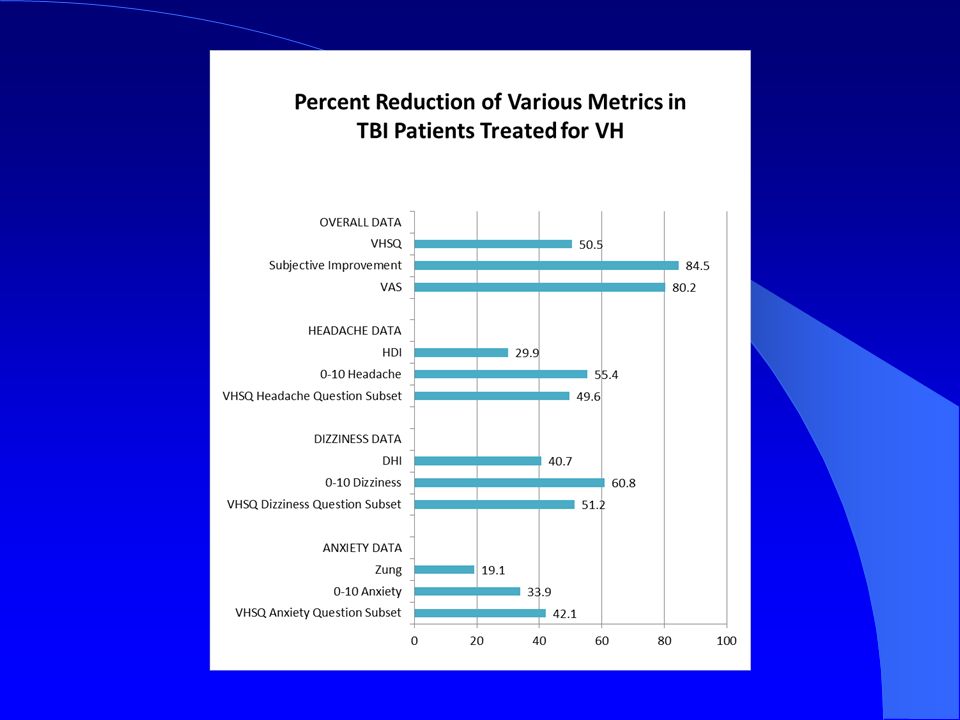
Dizziness 2012 46 patients 2009-2011 Chief complaint of dizziness
Dizziness Handicap Inventory (DHI) Headache Disability Index (HDI) Zung Anxiety Scale (Zung) Vertical Heterophoria Symptom Questionaire (VHSQ) 10 cm Visual Analog Scale (VAS)
 Headache Disability Index (HDI) Zung Anxiety Scale (Zung) Vertical Heterophoria Symptom Questionaire (VHSQ) 10 cm Visual Analog Scale (VAS)")
62
Results 2012 DHI decreased by 51% P<0.0001
HDI decreased by 45% P<0.0001 VHSQ decreased by 50% P<0.0001 Zung decreased by 22% P<0.0001 VAS decreased by 71% P<0.0001

63
Phoric Eye Posture in VH
Orthophoria Fovea T Traditional Vertical Heterophoria (CN4 / SO palsy) OS *Vertical Heterophoria due to vertical orbital misalignment OD *Vertical Heterophoria due TBI *Optics not differentiated in the literature from Traditional VH (paradigm shift)
 OS. *Vertical Heterophoria due to vertical orbital misalignment. OD. *Vertical Heterophoria due TBI. *Optics not differentiated in the literature from Traditional VH (paradigm shift)")
65
VH (A – orbital asymmetry) – Initial pathology affects both eyes
Line of sight / phoric position of high eye is depressed (Initial pathology) Line of sight / phoric position of low eye is elevated (Initial pathology) High eye sees high image High eye is made even higher with head tilt* *Driving force is resolution of vertical diplopia CN 4 / SO Palsy (B – CVA, tumor) – Initial pathology affects only 1 eye Line of sight / phoric position of high eye is elevated and extorted (Initial pathology) Line of sight / phoric position of low eye is straight ahead (normal) and intorted (Secondary pathology) High eye sees low image High eye is made even higher with head tilt* *Driving force is resolution of torsional / rotational diplopia (still left with vertical disparity)
 Line of sight / phoric position of low eye is elevated (Initial pathology) High eye sees high image. High eye is made even higher with head tilt* *Driving force is resolution of vertical diplopia. CN 4 / SO Palsy (B – CVA, tumor) – Initial pathology affects only 1 eye. Line of sight / phoric position of high eye is elevated and extorted (Initial pathology) Line of sight / phoric position of low eye is straight ahead (normal) and intorted (Secondary pathology) High eye sees low image. High eye is made even higher with head tilt* *Driving force is resolution of torsional / rotational diplopia (still left with vertical disparity)")
69
Utricle Dysfunction

70
Precipitating Events Trauma Inner ear infection Eye surgery
Mono-vision contacts Congenital Middle age

71
Utricle Dyfunction Head tilt Vertical misalignment Ocular torsion

72
Superior semicircular canal
Works with utricle on vertcal eye posture SSCD Superior semicircular canal dehiscence

74
Head Roll Tilt Tilt to stabilize retinal image and reduce diplopia
Second most destabalized head posture after head back Semicircular canals, otoliths, eyes are not in proper alignment with gravity Change in center of gravity

75
Head Tilt Destabilize balance and posture
Inner ear and eyes not in normal plane Induction of vertical optokinetic nytagmus on motion

76
Foot Posture Feet position change with prism Toe in versus toe out

77
Vertical Eye Height Imbalance
30% of the population has one eye higher than the other 4% of the population has Vertical Herterophoria

78
Retinal Slip Eye misalignment and head tilt causes image to be off center of fovea Eye muscles are constantly trying to align images Transient diplopia from muscle fatigue Similar to meniere’s with a constantly changing sensory input Muscle pain mediated through V1 and V2

79
Visual Preference for Balance
Aldopho Bronstein Visual Vertigo

80
Motion Sickness Vertical optico-kinetic nystagmus Associated roll tilt
Combined with vertical eye skew Asymmetric optico-kinetic nystagmus in time and angle Utricle dysfunction Visual preference for balance

81
Hierarchy of Balance Staying upright Binocular vision Roll head tilt
Ocular torsion

82
Menieres Disese of the eye
Fluctuation of visual image causes symptoms Prevents compensation Translational vestibulo-occulo reflex vs rotational vestibulo-occulo reflex

83
Feel like falling Translational VOR Rotational VOR
Switching between visual and vestibular system

84
Medications Neurology of eye movements, John Leigh, and David Zee

85
Pathophysiology Combination of: vertical misalignment of the eyes, head tilt, utricle dysfunction, and a visual preference for balance causes symptoms

86
VNG findings Pursuit Saccade Optiko-kinetic
May have unilateral weakness or directional preponderance Central vertigo

87
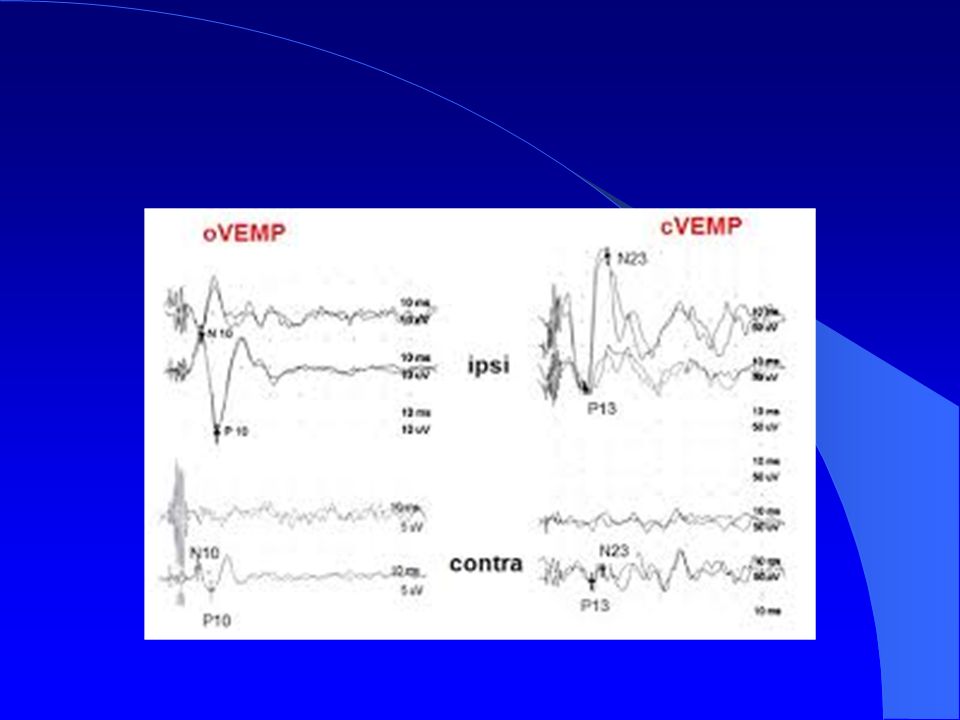
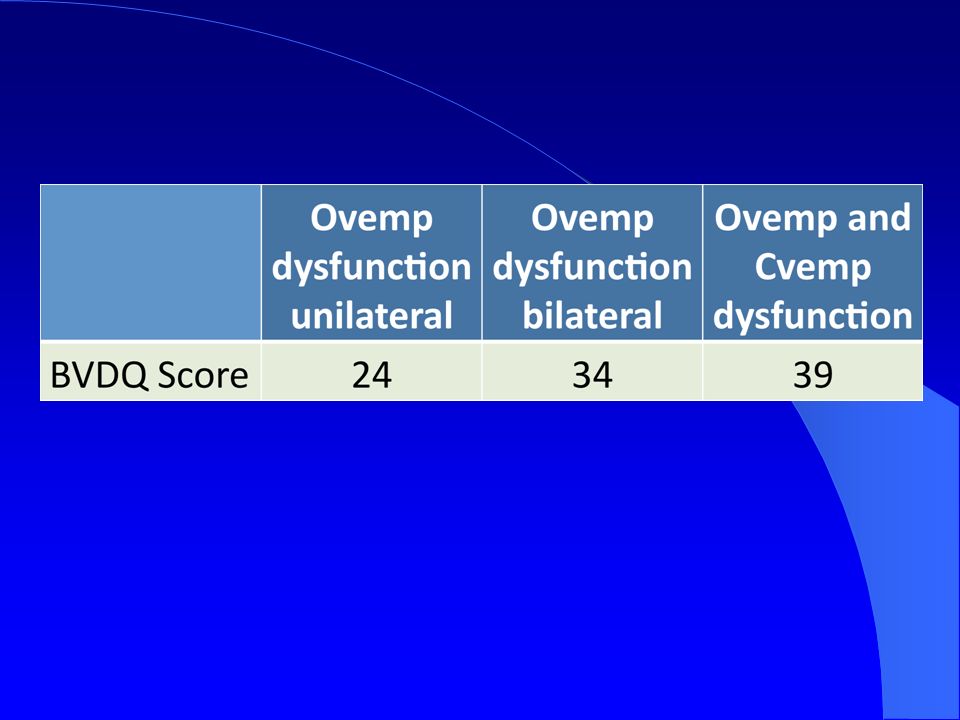
Vestibular evoked myogrenic potential
Occular VEMP utricle Cervical VEMP saccule Stimuli tone or vibration

88
C-VEMP

89
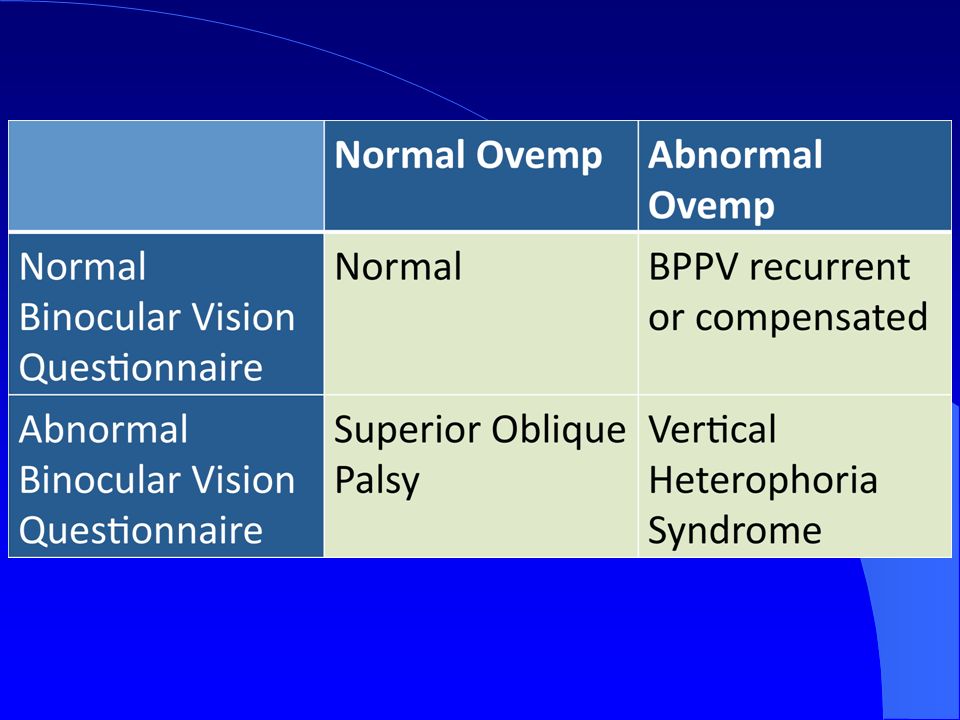
O-VEMP

94
Saccule Balance when supine or prone Autonomic dysfunction
Postural hypotention Aging Pots Syndrome

95
Vestibular Therapy Model from speech therapy
Therapy targeted to VNG and VEMP test results

96
Vestibular therapy Utricle dysfunction Saccule dysfunction
Pursuit abnormalities Saccade abnormality Optokinetic dysfunction motion sickness Caloric loss

97
Vestibular therapy Roll tilt Leg lenth abnormality Pelvic assymetry
Numbness of feet Low vison

98
Vestibular therapy Hearing loss

99
Acute Vertical Heterophoria Syndrome
Often associated with Benign paroxysmal positional vertigo Can be associated with vestibular neuronitis Often hospitalized Treated differently

100
“Who, indeed, could have supposed that a mere ocular defect could have given rise to so serious a train of evils…and who that had not seen it could believe that the correction by glasses of the eye trouble could have given a relief so speedy and so perfect that [the patient] herself described it as a miracle?” S. Weir Mitchell, Headaches and Eye Strain April 1876 (13)
![Who, indeed, could have supposed that a mere ocular defect could have given rise to so serious a train of evils…and who that had not seen it could believe that the correction by glasses of the eye trouble could have given a relief so speedy and so perfect that [the patient] herself described it as a miracle](http://slideplayer.com/slide/8566451/26/images/100/Who%2C+indeed%2C+could+have+supposed+that+a+mere+ocular+defect+could+have+given+rise+to+so+serious+a+train+of+evils%E2%80%A6and+who+that+had+not+seen+it+could+believe+that+the+correction+by+glasses+of+the+eye+trouble+could+have+given+a+relief+so+speedy+and+so+perfect+that+%5Bthe+patient%5D+herself+described+it+as+a+miracle.jpg "S. Weir Mitchell, Headaches and Eye Strain April 1876 (13)")
101
Thank you Angie Mcnab (Lederman) Cheryl Wilson
 Cheryl Wilson")
Similar presentations











 Range of Movement and Ocular Alignment Establish.>")










![Eyes and Vision [Name of Presenter] Doctor of Optometry.](/18/5703594/big_thumb.jpg "Eyes and Vision [Name of Presenter] Doctor of Optometry.>")


