Download presentation
Presentation is loading. Please wait.

1
Fibromyalgia --- from pathophysiology to evidence-based treatment 財團法人為恭紀念醫院 精神科 鄧方怡醫師

2
Conceptual evolution

3
The misnomer of “fibrositis” Clinical descriptions of fibromyalgia have been reported since mid-1800s In 1904, Sir William Gowers introduced the term "Fibrositis" to describe the inflammation of fibrous tissue in his description of low back pain. Also In 1904, Ralph Stockman first reported evidence of inflammatory changes in the fibrous, intra-muscular septa on biopsies from patients

4
The misnomer of “fibrositis” However, subsequent studies of muscle biopsies have failed to reproduce Stockman’s findings. Various terms, included neurasthenia, fibrositis, fibromyositis, psychogenic, psychosomatic, muscular rheumatism, had been applied in subsequent years. Yet the term fibrositis has been most resilient and "eventually became synonymous with idiopathic local or diffuse musculoskeletal pain of any type"

5
Recent development In the 1970’s, Hench first introduced the term "fibromyalgia". In the 1980’s, Yunus, proposed the need for a unified classification system as well as the first diagnostic criteria. Finally, in 1990, the American College of Rheumatology established firm criteria for the classification and diagnosis of fibromyalgia

6
Diagnostic Labels For Fibromyalgia Syndrome DaCosta Syndrome/Shell Shock (brain) Neurasthenia (nerves) Chronic Brucellosis (viral) Failure to Cope (psychological) Fibrositis (muscle inflammation) Affective Spectrum Disorder (depressive disorder) Fibromyalgia
 Neurasthenia (nerves) Chronic Brucellosis (viral) Failure to Cope (psychological) Fibrositis (muscle inflammation) Affective Spectrum Disorder (depressive disorder) Fibromyalgia")
7
The ACR criteria 1. History of widespread pain for 3 months in combination with 2. Tenderness at 11 or more of 18 specific tender points sites when digitally palpated with about 4 kg/1.4cm2 per unit area of force 3. No exclusions are made for the presence of concomitant radiographic or laboratory abnormalities

8
Location of tender points. * Represents "control" points.

9
Clinical presentation

10
What is Fibromyalgia Pain ---Clinical and experimental ---Lower pain threshold, allodynia, and hyperalgesia ---Involves musculoskeletal structures, skin, and in some cases, viscera Behavioral disturbances: ---Reduced activity, social interaction, function ---Avoidance of events that evoke pain ---Affective distress ---Increased usage of health services

11
Neuropsychological symptoms %

12
The Criticism of ACR criteria Many patients with chronic widespread pain may have les than the 11 of 18 tender points Artificially increase the female predominance Select for individuals with higher levels of disease-related distress Fail to capture the “essence”

13
Epidemiology

14
Prevalence 10~11% of the population has chronic widespread pain at ay given time 1/5 of above meet the ACR criteria of fibromyalgia 3.4% in women versus 0.5% in men It occurs in 5%~6% of adult patients presenting at general medical practice and in 10%~20% of adult patients presenting to rheumatologists. 2nd most common disorder observed by rheumatologists

15
Comorbidity 80%:chronic fatigue syndrome 80%:have headaches 75%:temporomandibular disorders 60%:irritable bowel syndrome

16
FMS is Multi-system—not just muscles Chronic Fatigue Syndrome Non-restorative Sleep Cognitive Problems (“fibro fog”) Irritable bowel Irritable bladder Chronic headache Vulvodynia Orthostatic Hypotension Postural Orthostatic Tachycardia (POTS) Anxiety Depression Delayed Post Exertional Flare-Up
 Irritable bowel Irritable bladder Chronic headache Vulvodynia Orthostatic Hypotension Postural Orthostatic Tachycardia (POTS) Anxiety Depression Delayed Post Exertional Flare-Up")
17
Disability 25.3% of patients received disability payments. However, only 25% of these were specifically for the diagnosis. 31% of patients employed prior to onset of their FM reported loss of employment due to their disease The disability associated with FM does not change substantially over time according to one 7 year cohort study

18
Pathophysiology

19
Aberrant pain processing?

20
Temporal summation/Wind-up Pain increases in intensity when painful stimuli are applied repetitively. Only repetitive stimuli at shorter interval(3 s) resulted in a significant increase in pain ratings.
 resulted in a significant increase in pain ratings..")
21
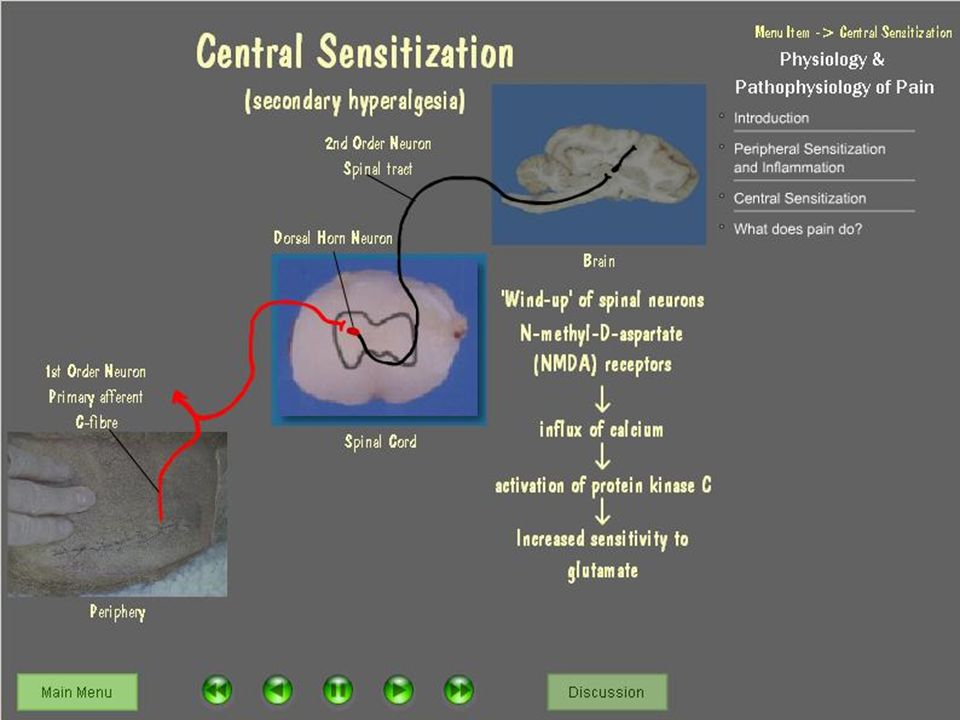
Central sensitization Hyperalgesia: augmentation of pain sensation Allodynia: lowered pain threshold It is associated with enlarged receptive fields and is often occur as a consequence of temporal summation

23
Greater windup in patients with FM

24
Prolonged and more intense after-sensations

25
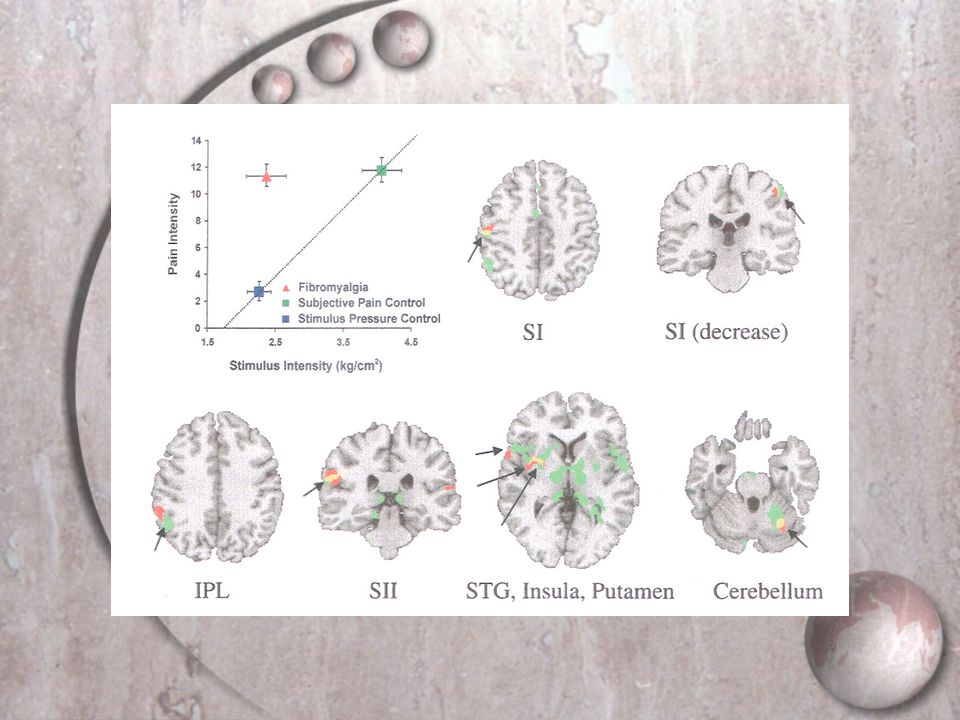
Evidence from fMRI Patients display a normal “detection” threshold to sensory stimuli, but exhibit a decreased “noxious threshold” This phenomenon is independent of psychological factors such as expectancy or hypervigilance Increased activity of cerebral pain processing areas on fMRI

26
Evidence from fMRI Decreased thalamic activity on functional brain scans fMRI/SPECT studies support the hypothesis that fibromyalgia is characterized by cortical or sub- cortical augmentation of pain processing Gracely R, et. al. Arthritis Rheum. 2002 Gracely R, et. al. Bet Pract res Clin rheum, 2003

28
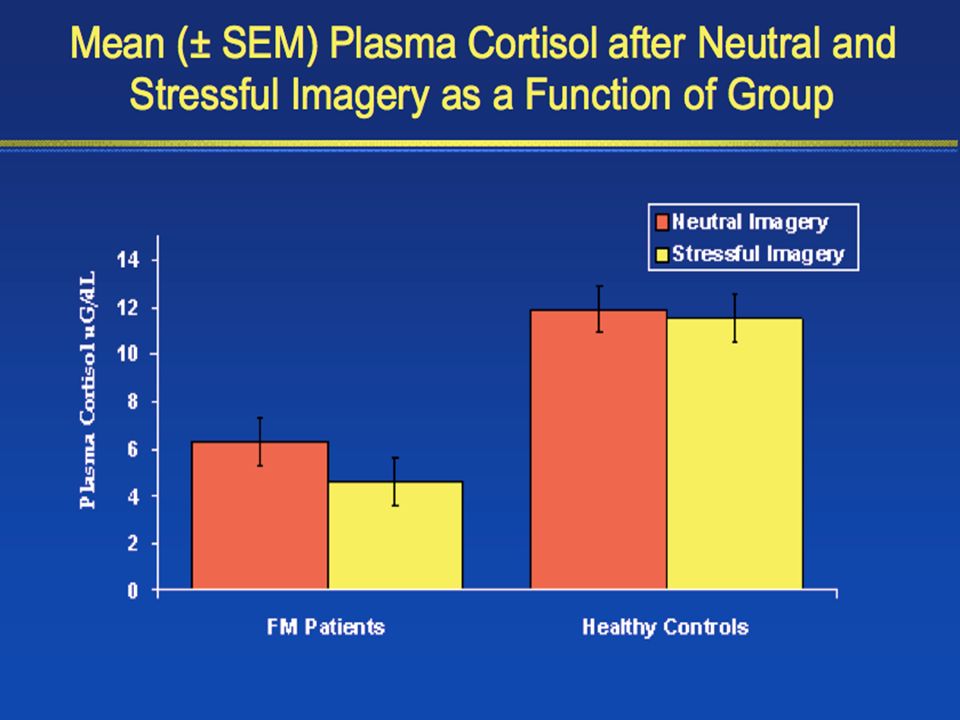
Effects of stress Symptom onset and exacerbation during periods of stress Clinical response of symptoms to therapeutic agents that alter stress mediators(exercise, TCA, SSRI) FM has been reported to occur at increased frequency in PTSD patients Some authors have suggested that it is stress itself that provides the etiology for FM
 FM has been reported to occur at increased frequency in PTSD patients Some authors have suggested that it is stress itself that provides the etiology for FM")
30
Disturbance in HPA axis Healthy HPA axis: circadian variation with high cortisol in AM and low cortisol in PM FM patients: abnormally elevated plasma cortisol concentration in the evening It may be related to reduced levels of 5-HT

31
Disturbance in HPA axis Marked hypersecretion of ACTH in response to severe acute stressors. This has been suggested to result from chronic hyposecretion of CRH HPA abnormalities may be related to depressed autonomic nervous system function.

32
Common biological pathways shared in FM and psychiatric disorder FM patients’ response to dexamethasone suggests similarity with PTSD Increased “drive” to activity of the HPA axis in melancholic depression

33
Biochemical abnormalities underlying FM Levels of 5-HT & primary metabolites of NE and 5- HT are both reduced in patients with FM Reduced levels of 5-HIAA and tryptophan were associated with increased pain in FM patients 5-HT inhibits the release of neurotransmitters involved in pain processing (substance P, excitatory amino acids)
")
34
Biochemical abnormalities underlying FM Measures of pain intensity in FM patients are positively correlated with the levels of glutamate and aspartate metabolites, glycine, and taurine. The level of substance P,NGF,glutamate, and aspartate is elevated in CSF of FM patients Above changes lead to decrease in presynaptic inhibition of pain-related primary afferent neurons

35
Biochemical abnormalities underlying FM Low levels of 5-HIAA and high concentrations of substance P were both positively correlated with more severe sleep disturbance Dysregulation of 5-HT has been associated with depression and anxiety.

36
Behavior and psychological factors Psychological distress or psychiatric illness is associated with greater health careseeking behavior at tertiary care facilities Psychological factors are not necessary or sufficient to produce fibromyalgia. The most common psychiatric conditions observed in patients with FM include depression (current:30%, life time:60%), dysthymia (10%), panic disorder (7%), and simple phobia (12%)
, dysthymia (10%), panic disorder (7%), and simple phobia (12%).")
37
The Neurobiological / Psychobehavioral Continuum Neurobiological factors Abnormal sensory processing Biochemical dysfunction HPA dysfunction ? Peripheral factors Psychobehavioral factors General “distress” Cognitive factors Psychiatric comorbidities Maladaptive illness behaviors Secondary gain issues Population Primary Care Tertiary Care Definition factors (e.g., tender points)
.")
38
Treatment

39
Pharmacotherapy Wind-up is dependent on the activation of NMDA receptors by glutamate and substance P NMDA receptor blockers (ketamine and dextromethorphan) have prove benefit in pain control NE and 5-HT release from the descending tract and down-regulate dorsal neuron excitability.
 have prove benefit in pain control NE and 5-HT release from the descending tract and down-regulate dorsal neuron excitability.")
41
Anti-seizure medications are beneficial in inhibiting the release of glutamate and substance P Medications that block the re-uptake of both NE and 5-HT appear to be more effective than SSRI

42
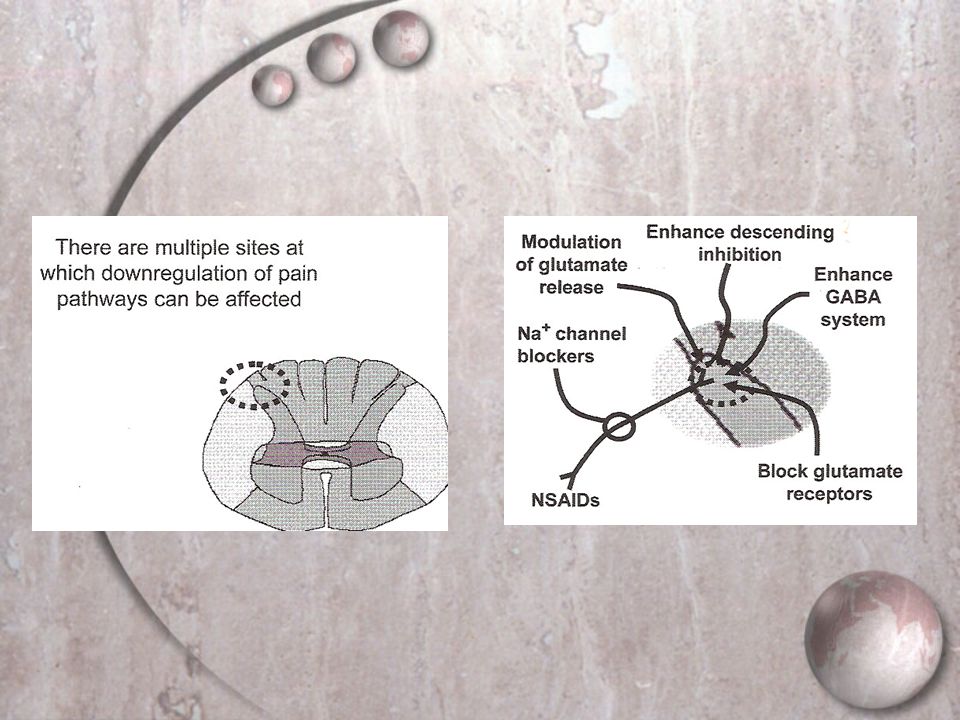
Medical strategy Anti-inflammatory [NSAID, Prednisone]-Failed Block substance P receptor-Failed Inhibit nerve signal conduction-success Correct insomnia-Success Augment descending inhibition-Success ---Increase 5-HT synthesis and /or NE-like ---Decrease 5-HT and/or NE reuptake
![Medical strategy Anti-inflammatory [NSAID, Prednisone]-Failed Block substance P receptor-Failed Inhibit nerve signal conduction-success Correct insomnia-Success Augment descending inhibition-Success ---Increase 5-HT synthesis and /or NE-like ---Decrease 5-HT and/or NE reuptake](http://images.slideplayer.com/26/8521961/slides/slide_42.jpg "Medical strategy Anti-inflammatory [NSAID, Prednisone]-Failed Block substance P receptor-Failed Inhibit nerve signal conduction-success Correct insomnia-Success Augment descending inhibition-Success ---Increase 5-HT synthesis and /or NE-like ---Decrease 5-HT and/or NE reuptake")
43
Treatment of Fibromyalgia Syndrome Medications Stron g Evidence for Efficacy Amitriptyline: often helps sleep a n d overall well-being; dose, 25-50 mg at bedtim e. Cyclobenzaprin e : similar response and adverse effects; dose, 10-30 mg at bedtim e. Modest Evidence for Efficacy Tramadol: long-term efficacy and tolerabil i ty unknown; administered with or without acetaminophen; dose, 200- 3 00 mg /d. Serotonin reuptake inhibitors (SSRIs): Fluoxet i ne (only one carefully evaluated at this time): dose, 20-80 m g; may be used with tricyclic given at bedtime; uncontrolled rep o rt of efficacy using sertrali ne. Dual-reuptake inhibit o rs (SNRIs): Venlafaxine: 1 RCT ineffective but 2 case repo r ts found higher dose effecti ve. Milnacipran: effective in single R CT. Duloxetine: effective in single R CT. Pregabal i n: second-generation anticonvulsant; effective in single R CT. Weak Evidence for Efficacy Growth hormone: modest improvemen t in subset of patients with FMS with low growth hormone level s at basel in e. 5-Hydroxytryptamine (serotonin): methodolog i cal probl ems. Tropisetron: not commercially availa bl e. S-adenosyl-methion i ne: mixed resu lt s. Goldenberg et al. JAMA. 2004
: Fluoxet i ne (only one carefully evaluated at this time): dose, m g; may be used with tricyclic given at bedtime; uncontrolled rep o rt of efficacy using sertrali ne. Dual-reuptake inhibit o rs (SNRIs): Venlafaxine: 1 RCT ineffective but 2 case repo r ts found higher dose effecti ve. Milnacipran: effective in single R CT. Duloxetine: effective in single R CT. Pregabal i n: second-generation anticonvulsant; effective in single R CT. Weak Evidence for Efficacy Growth hormone: modest improvemen t in subset of patients with FMS with low growth hormone level s at basel in e. 5-Hydroxytryptamine (serotonin): methodolog i cal probl ems. Tropisetron: not commercially availa bl e. S-adenosyl-methion i ne: mixed resu lt s. Goldenberg et al. JAMA")
44
No Evidence for Efficacy Opioids, corticosteroids, nonsteroidal anti-inflammatory drugs, benzodiazepene and nonbenzodiazepene hypnotics, melatonin, calcitonin, thyroid hormone, guaifenesin, dehydroepiandrosterone, magnesium. Nonmedicinal Therapies Strong Evidence for Efficacy (Wait-List or Flexibility Controls But Not Blinded Trials) Cardiovascular exercise: efficacy not maintained if exercise stops. CBT: improvement often sustained for months. Patient education: group format using lectures, written materials, demonstrations; improvement sustained for 3 to 12 months. Multidisciplinary therapy, such as exercise and CBT or education and exercise. Moderate Evidence for Efficacy Strength training, acupuncture, hypnotherapy, biofeedback,balneotherapy. Weak Evidence for Efficacy Chiropractic, manual, and massage therapy; electrotherapy, ultrasound. No Evidence for Efficacy Tender (trigger) point injections, flexibility exercise. Goldenberg et al. JAMA. 2004
 Cardiovascular exercise: efficacy not maintained if exercise stops. CBT: improvement often sustained for months. Patient education: group format using lectures, written materials, demonstrations; improvement sustained for 3 to 12 months. Multidisciplinary therapy, such as exercise and CBT or education and exercise. Moderate Evidence for Efficacy Strength training, acupuncture, hypnotherapy, biofeedback,balneotherapy. Weak Evidence for Efficacy Chiropractic, manual, and massage therapy; electrotherapy, ultrasound. No Evidence for Efficacy Tender (trigger) point injections, flexibility exercise. Goldenberg et al. JAMA")
45
Evidence for treatment efficacy was ranked as: Strong: positive results from a meta-analysis or consistently positive results from more than 1 RCT Moderate : positive results from 1 RCT or largely positive results from multiple RCTs or consistently positive results from multiple non-RCT studies Weak:positive results from descriptive and case studies, inconsistent results from RCTs, or both Goldenberg et al. JAMA. 2004

46
Stepwise Fibromyalgia Management Step 1 Confirm the diagnosis. Explain the condition. Evaluate and treat comorbid illness, such as mood disturbances and primary sleep disturbances. Step 2 Trial with low-dose tricyclic antidepressant or cyclobenzaprine. Begin cardiovascular fitness exercise program. Refer for cognitive behavior therapy or combine that with exercise.

47
Step 3 Specialty referral (eg, rheumatologist, physiatrist, psychiatrist, pain management). Trials with selective serotonin reuptake inhibitor, serotonin and norepinephrine reuptake inhibitor, or tramadol. Consider combination medication trial or anticonvulsant.

48
Thanks for your concentration

Similar presentations





. OUTLINE What is Fibromyalgia (FMS)? What causes it? Who gets it? How is it diagnosed? How is it treated? What are some of.>")







. - FM is one of the main causes of Chronic Widespread Pain (CWP).>")





