Download presentation
Presentation is loading. Please wait.

1
Romàn Pérez-Soler Gutman Professor of Medicine and Chairman of the Department of Oncology at the Montefiore Medical Center, Albert Einstein College of Medicine, Bronx, New York, USA Worked at the MD Anderson Cancer Center (Departments of Clinical Immunology and Thoracic/Head and Neck Medical Oncology) for 16 years Former Associate Director of Clinical and Translational Research, Kaplan Comprehensive Cancer Center, New York University Medical Center Author of 150 papers, 20 book chapters, and 175 abstracts Involved in the development of new targeted anticancer therapies, in particular for lung cancer Montefiore Medical Center
 for 16 years. Former Associate Director of Clinical and Translational Research, Kaplan Comprehensive Cancer Center, New York University Medical Center. Author of 150 papers, 20 book chapters, and 175 abstracts. Involved in the development of new targeted anticancer therapies, in particular for lung cancer. Montefiore Medical Center.")
2
First choice in second line: erlotinib in NSCLC
Romàn Pérez-Soler Montefiore Medical Center Albert Einstein College of Medicine New York, USA

3
Treating second-line NSCLC
Lung cancer is a major cause of morbidity and mortality huge impact on global health systems and one of the leading causes of cancer-related death Many patients diagnosed with advanced disease and unsuitable for surgery first-line chemotherapy is usual course of treatment Limited second-line treatment options available patients may have reduced performance status (PS) due to previous treatment or progression need to balance efficacy versus tolerability and quality of life (QoL) NSCLC = non-small-cell lung cancer
 due to previous treatment or progression. need to balance efficacy versus tolerability and quality of life (QoL) NSCLC = non-small-cell lung cancer.")
4
Continuing need for more treatment options
Need for new and different therapeutic options more choice for clinicians and patients Increasing interest in concept of tailored therapy new diagnostic methods e.g. biomarkers could be used to predict which patients benefit most Current second-line agents include chemotherapy (docetaxel, pemetrexed) epidermal growth factor receptor (EGFR) tyrosine-kinase inhibitors (erlotinib, gefitinib)
 epidermal growth factor receptor (EGFR) tyrosine-kinase inhibitors (erlotinib, gefitinib)")
5
The current treatment algorithm for NSCLC
Early (stage I/II/ selected IIIA) NSCLC Advanced (stage IIIB with PE/IV) Suitable for standard chemotherapy? PS Age Controlled/uncontrolled brain metastases Concomitant medical condition Surgery ± chemotherapy First line Yes No Radiotherapy (if unfit for surgery) Fit elderly/ PS 2? Frail elderly/ PS 3 PS 4 Best supportive care Locally advanced (stage IIIA/IIIB no PE) Platinum-based doublet chemotherapy ± bevacizumab Single agent Relapse Chemotherapy (platinum doublet) + concomitant radiotherapy or sequential Chemotherapy – docetaxel – pemetrexed – vinorelbine – gemcitabine EGFR-targeted therapy – erlotinib – gefitinib Second/third line PE = pleural effusion
 NSCLC. Advanced (stage IIIB with PE/IV) Suitable for standard chemotherapy PS. Age. Controlled/uncontrolled brain metastases. Concomitant medical condition. Surgery ± chemotherapy. First line. Yes. No. Radiotherapy (if unfit for surgery) Fit elderly/ PS 2 Frail elderly/ PS 3. PS 4. Best supportive care. Locally advanced. (stage IIIA/IIIB no PE) Platinum-based doublet chemotherapy ± bevacizumab. Single agent. Relapse. Chemotherapy. (platinum doublet) + concomitant. radiotherapy. or sequential. Chemotherapy – docetaxel. – pemetrexed. – vinorelbine. – gemcitabine. EGFR-targeted therapy. – erlotinib. – gefitinib. Second/third line. PE = pleural effusion.")
6
Data overview: the BR.21 and TRUST studies

7
Erlotinib 150mg daily (n=488)
BR.21: trial design Erlotinib 150mg daily (n=488) RANDOM I SE Phase III trial Advanced stage IIIB/IV NSCLC (n=731) 2 Placebo (n=243) 1 Primary endpoint = overall survival (OS) Secondary endpoints = progression-free survival (PFS), response rate (RR) and duration of response, safety, QoL
 RANDOM I SE. Phase III trial. Advanced stage IIIB/IV NSCLC. (n=731) 2. Placebo (n=243) 1. Primary endpoint = overall survival (OS) Secondary endpoints = progression-free survival (PFS), response rate (RR) and duration of response, safety, QoL.")
8
BR.21: key eligibility criteria
Confirmed NSCLC, stage IIIB or IV Age 18 years PS 0, 1, 2 or 3 Measurable or non-measurable disease One or two prior chemotherapy regimens Adequate organ function EGFR immunohistochemistry (IHC+) status not required No prior EGFR inhibitors No prior malignancies or uncontrolled central nervous system (CNS) metastases Written informed consent
 status not required. No prior EGFR inhibitors. No prior malignancies or uncontrolled central nervous system (CNS) metastases. Written informed consent.")
9
BR.21: overall survival 100 75 50 25 n Median survival (months)
n Median survival (months) 1-year survival Erlotinib 488 6.7 31 Placebo 243 4.7 21 Survival probability (%) HR=0.73, p=0.001* 42.5% increase in median OS *HR and p (log-rank test) adjusted for stratification factors at randomisation and EGFR status HR = hazard ratio Time (months) Shepherd F, et al. N Engl J Med 2005;353:123–32 Tarceva Summary of Product Characteristics, F. Hoffmann-La Roche Ltd
 1-year survival. Erlotinib Placebo Survival probability (%) HR=0.73, p=0.001* 42.5% increase in median OS *HR and p (log-rank test) adjusted for stratification factors at randomisation and EGFR status HR = hazard ratio. Time (months) Shepherd F, et al. N Engl J Med 2005;353:123–32 Tarceva Summary of Product Characteristics, F. Hoffmann-La Roche Ltd.")
10
BR.21: progression-free survival
1.00 0.75 0.50 0.25 n Median survival (weeks) 6 months (%) Erlotinib 488 9.7 25 Placebo 243 8.0 10 HR=0.61, p<0.001* Survival distribution function 25% 10% Time (months) *HR and p (log-rank test) adjusted for stratification factors at randomisation and EGFR status Shepherd F, et al. N Engl J Med 2005;353:123–32
 6 months (%) Erlotinib Placebo HR=0.61, p<0.001* Survival distribution function. 25% 10% Time (months) *HR and p (log-rank test) adjusted for stratification. factors at randomisation and EGFR status. Shepherd F, et al. N Engl J Med 2005;353:123–32.")
11
Is there a clinical benefit with erlotinib in men? Answer: Yes
Survival Women Men 1.00 0.75 0.50 0.25 1.00 0.75 0.50 0.25 HR=0.8 (0.6–1.1), p=0.13 HR=0.8 (0.6–0.9), p=0.01 Erlotinib (n=173) Erlotinib (n=315) Survival distribution function Placebo (n=83) Placebo (n=160) Months Months Shepherd F, et al. N Engl J Med 2005;353:123–32
, p=0.13. HR=0.8 (0.6–0.9), p=0.01. Erlotinib (n=173) Erlotinib (n=315) Survival distribution function. Placebo (n=83) Placebo (n=160) Months. Months. Shepherd F, et al. N Engl J Med 2005;353:123–32.")
12
Squamous-cell carcinoma Survival distribution function
Is there a clinical benefit with erlotinib in squamous-cell carcinoma? Answer: Yes Survival Adenocarcinomas Squamous-cell carcinoma 1.00 1.00 0.75 0.50 0.25 0.75 HR=0.7 (0.6– 0.9), p=0.008 HR=0.67 (0.5–0.9), p=0.0007 0.50 Survival distribution function Erlotinib (n=246) Erlotinib (n=144) 0.25 Placebo (n=119) Placebo (n=78) Months Months Shepherd F, et al. N Engl J Med 2005;353:123–32
, p= HR=0.67 (0.5–0.9), p= Survival distribution function. Erlotinib (n=246) Erlotinib (n=144) Placebo (n=119) Placebo (n=78) Months. Months. Shepherd F, et al. N Engl J Med 2005;353:123–32.")
13
Is there a clinical benefit with erlotinib in current/ex-smokers
Is there a clinical benefit with erlotinib in current/ex-smokers? Answer: Yes Current/ex-smokers Never smokers 1.00 1.00 HR=0.9 (0.7–1.0), p=0.141* HR=0.42 (0.28–0.64), p<0.001 0.75 0.75 Erlotinib (n=358) Erlotinib (n=104) Survival distribution function 0.50 0.50 0.25 0.25 Placebo (n=187) Placebo (n=42) Months Months *Log-rank test Shepherd F, et al. N Engl J Med 2005;353:123–32
, p=0.141* HR=0.42 (0.28–0.64), p< Erlotinib (n=358) Erlotinib (n=104) Survival distribution function Placebo (n=187) Placebo (n=42) Months. Months. *Log-rank test. Shepherd F, et al. N Engl J Med 2005;353:123–32.")
14
Investigating optimal dosing regimen for current/former smokers
Erlotinib PK single dose Never smokers: Erlotinib 150mg/day Screening and tissue collection Day 3 Current/former smokers: Erlotinib dose escalation Day –7 to 0 Day 1 Primary endpoint: non-progression at 8 weeks Follow-up = 6 months; dose escalation up to 300mg in 50mg increments; regular PK sampling during treatment period Status: 22/44 recruited (pan-Europe) Abstract submitted to ASCO 2008 PK = pharmacokinetic PI: Dr EF Smit (The Netherlands)
 Abstract submitted to ASCO PK = pharmacokinetic. PI: Dr EF Smit (The Netherlands)")
15
BR.21: all patient subgroups derived a survival benefit
Erlotinib:placebo PS 0– (0.6–0.9) PS 2– (0.6–1.0) Male (0.6–0.9) Female (0.6–1.1) <65 years (0.6–0.9) 65 years (0.6–1.0) Adenocarcinoma (0.6–0.9) Squamous-cell carcinoma (0.5–0.9) Other histology (0.7–1.5) Erlotinib:placebo Never-smoker (0.3–0.6) Current/ex-smoker (0.7–1.1) 1 prior regimen (0.6–1.0) 2+ prior regimens (0.6–1.0) Best prior response: CR/PR (0.5–0.9) Best prior response: SD (0.6–1.1) Best prior response: PD (0.6–1.2) Asian (0.4–1.0) Other (0.7–0.9) Factors 0 1 2 0 1 2 HR HR CR = complete response; PD = progressive disease; PR = partial response; SD = stable disease; HR <1 = improved survival with erlotinib Shepherd F, et al. N Engl J Med 2005;353:123–32
 PS 2– (0.6–1.0) Male 0.76 (0.6–0.9) Female 0.80 (0.6–1.1) <65 years 0.75 (0.6–0.9) 65 years 0.79 (0.6–1.0) Adenocarcinoma 0.71 (0.6–0.9) Squamous-cell carcinoma 0.67 (0.5–0.9) Other histology 1.04 (0.7–1.5) Erlotinib:placebo. Never-smoker 0.42 (0.3–0.6) Current/ex-smoker 0.87 (0.7–1.1) 1 prior regimen 0.76 (0.6–1.0) 2+ prior regimens 0.75 (0.6–1.0) Best prior response: CR/PR 0.67 (0.5–0.9) Best prior response: SD 0.83 (0.6–1.1) Best prior response: PD 0.85 (0.6–1.2) Asian 0.61 (0.4–1.0) Other 0.79 (0.7–0.9) Factors HR. HR. CR = complete response; PD = progressive disease; PR = partial response; SD = stable disease; HR <1 = improved survival with erlotinib. Shepherd F, et al. N Engl J Med 2005;353:123–32.")
16
Erlotinib does not produce haematological toxicity
BR.21: adverse events Erlotinib (n=485) Placebo (n=242) Any (%) Grade 3/4 (%) Rash 75 9 17 Diarrhoea 54 6 18 <1 Nausea 33 3 24 2 Vomiting 23 19 Stomatitis Fatigue 52 45 20 Ocular (all) 27 1 Anorexia 38 5 Infection 4 15 Erlotinib does not produce haematological toxicity Shepherd F, et al. N Engl J Med 2005;353:123–32
 Placebo (n=242) Any (%) Grade 3/4 (%) Rash Diarrhoea <1. Nausea Vomiting Stomatitis. Fatigue Ocular (all) Anorexia Infection Erlotinib does not produce haematological toxicity. Shepherd F, et al. N Engl J Med 2005;353:123–32.")
17
BR.21: change in QoL domains (EORTC QLQ-C30)
Improved* (%) Stable (%) Worse (%) Variable Erlotinib Placebo Global QoL† 35 26 16 28 49 46 Physical function† 31 19 18 24 51 57 Role function 39 32 14 20 47 Cognitive function 29 23 Emotional function† 30 36 37 Social function 21 44 *³10 point change from baseline at any time (clinically significant) †p0.01 EORTC = European Organisation for Research and Treatment of Cancer Bezjak A, et al. J Clin Oncol 2006;24:3831–7
 Stable (%) Worse (%) Variable. Erlotinib. Placebo. Global QoL† Physical function† Role function Cognitive function Emotional function† Social function *³10 point change from baseline at any time (clinically significant) †p0.01. EORTC = European Organisation for Research and Treatment of Cancer. Bezjak A, et al. J Clin Oncol 2006;24:3831–7.")
18
TRUST study design Phase IV, open-label, non-randomised, multicentre study in patients with advanced, inoperable (stage IIIB/IV) NSCLC, previously treated with 1–2 courses of chemotherapy or radiotherapy, or considered unsuitable for such treatment Erlotinib was given orally (150mg/day) until disease progression or unacceptable toxicity Dose interruption or reduction (to 100mg/day, then to 50mg/day) was permitted for treatment-related Adverse events (AEs) Data from 6,236 patients available for interim analysis
 NSCLC, previously treated with 1–2 courses of chemotherapy or radiotherapy, or considered unsuitable for such treatment. Erlotinib was given orally (150mg/day) until disease progression or unacceptable toxicity. Dose interruption or reduction (to 100mg/day, then to 50mg/day) was permitted for treatment-related Adverse events (AEs) Data from 6,236 patients available for interim analysis.")
19
TRUST: summary of safety data
Patients with available safety data 5,730 Patients with 1 AE (any cause) (%)* 3,063 (53) Patients with 1 AE (erlotinib-related) (%)* 635 (11) Patients with 1 erlotinib-related SAE (%) 256 (4) Patients who withdrew due to erlotinib-related AEs (%) 319 (6) *Other than the 15 prespecified AEs SAE = serious adverse event Ardizzoni A, et al. J Thorac Oncol 2007;2(Suppl 4):S342 (Abstract B3–06)
 (%)* 3,063 (53) Patients with 1 AE (erlotinib-related) (%)* 635 (11) Patients with 1 erlotinib-related SAE (%) 256 (4) Patients who withdrew due to erlotinib-related AEs (%) 319 (6) *Other than the 15 prespecified AEs SAE = serious adverse event. Ardizzoni A, et al. J Thorac Oncol 2007;2(Suppl 4):S342 (Abstract B3–06)")
20
TRUST: incidence of erlotinib-related rash*
30% 58% 12% Ardizzoni A, et al. J Thorac Oncol 2007;2(Suppl 4):S342 (Abstract B3–06) *Based on data from 6,153 patients
:S342 (Abstract B3–06) *Based on data from 6,153 patients.")
21
Rash may be related to magnitude of benefit from erlotinib in NSCLC
Excludes patients who died within 28 days of entry Grade 0 (n=86) Median: 3.3 months Grade 1 (n=135) Median: 7.1 months Grade 2+ (n=223) Median: 11.1 months 1.00 0.75 0.50 0.25 Grade HR 95% CI p value 2+ vs 0 0.29 0.22–0.38 <0.001 1 vs 0 0.41 0.31–0.55 2+ vs 1 0.70 0.54–0.90 0.005 Survival probability Time (months) Correlation was maintained in multivariate analyses CI = confidence interval Wacker B, et al. Clin Cancer Res 2007;13:3913–21
 Median: 3.3 months. Grade 1 (n=135) Median: 7.1 months. Grade 2+ (n=223) Median: 11.1 months Grade. HR. 95% CI. p value. 2+ vs –0.38. < vs – vs – Survival probability Time (months) Correlation was maintained in multivariate analyses. CI = confidence interval. Wacker B, et al. Clin Cancer Res 2007;13:3913–21.")
22
Comparison between TRUST and BR.21
CR <1 1 PR 11 8 SD 56 35 Disease control rate (CR + PR + SD) 68 44 Dose reductions due to erlotinib-related event 14 19 Withdrawals due to erlotinib-related event 6 5 Incidence of erlotinib-related rash 70 76 Incidence of interstitial lung disease *Given the differences between study designs and patient populations, the studies are not directly comparable †Patient numbers are different between parameters 1Ardizzoni A, et al. J Thorac Oncol. 2007;2(Suppl. 4):S342 (Abstract B3–06) 2Shepherd FA, et al. N Engl J Med 2005;353:123–32
 Dose reductions due to erlotinib-related event Withdrawals due to erlotinib-related event Incidence of erlotinib-related rash Incidence of interstitial lung disease. *Given the differences between study designs and patient populations, the studies are not directly comparable †Patient numbers are different between parameters. 1Ardizzoni A, et al. J Thorac Oncol. 2007;2(Suppl. 4):S342 (Abstract B3–06) 2Shepherd FA, et al. N Engl J Med 2005;353:123–32.")
23
BR.21 and TRUST*: improvement in PFS with erlotinib
1.00 0.75 0.50 0.25 BR.211 Median PFS: erlotinib 9.7 weeks; placebo 8 weeks (p<0.001) TRUST2 Median PFS: 13 weeks Erlotinib (TRUST), n=6,181† Survival distribution function Erlotinib (BR.21), n=488 Placebo (BR.21), n=243 *Given the differences between study designs and patient populations, the studies are not directly comparable †Patient numbers are different between parameters PFS (months) 1Shepherd FA, et al. N Engl J Med 2005;353:123–32 2Ardizzoni A, et al. J Thorac Oncol. 2007;2(Suppl. 4):S342 (Abstract B3–06)
 TRUST2. Median PFS: 13 weeks. Erlotinib (TRUST), n=6,181† Survival distribution function. Erlotinib (BR.21), n=488. Placebo (BR.21), n= *Given the differences between study designs and patient populations, the studies are not directly comparable †Patient numbers are different between parameters. PFS (months) 1Shepherd FA, et al. N Engl J Med 2005;353:123–32 2Ardizzoni A, et al. J Thorac Oncol. 2007;2(Suppl. 4):S342 (Abstract B3–06)")
24
TRUST and BR.21: conclusions
TRUST interim safety data no new safety signals confirmed favourable safety profile of erlotinib observed in phase III BR.21 study TRUST interim efficacy data appeared consistent with previous data observed disease control rate and median PFS in line with those from BR.21 study

25
Erlotinib in the routine clinical setting

26
Case study: patient history and initial treatment
67-year-old female, former smoker (10 pack-years) December 2006: examination found mass in left upper lobe plus a single brain metastasis (T2N2M1) January 2007: brain metastasis resected followed by brain radiotherapy (XRT); confirmed adenocarcinoma March 2007: multiple bone metastases observed 2 cycles of carboplatin + paclitaxel, followed by concomitant weekly carboplatin + paclitaxel + chest XRT (completed in July 2007) partial response in left lung lesion stable disease in bone lesions
 December 2006: examination found mass in left upper lobe plus a single brain metastasis (T2N2M1) January 2007: brain metastasis resected followed by brain radiotherapy (XRT); confirmed adenocarcinoma. March 2007: multiple bone metastases observed. 2 cycles of carboplatin + paclitaxel, followed by concomitant weekly carboplatin + paclitaxel + chest XRT (completed in July 2007) partial response in left lung lesion. stable disease in bone lesions.")
27
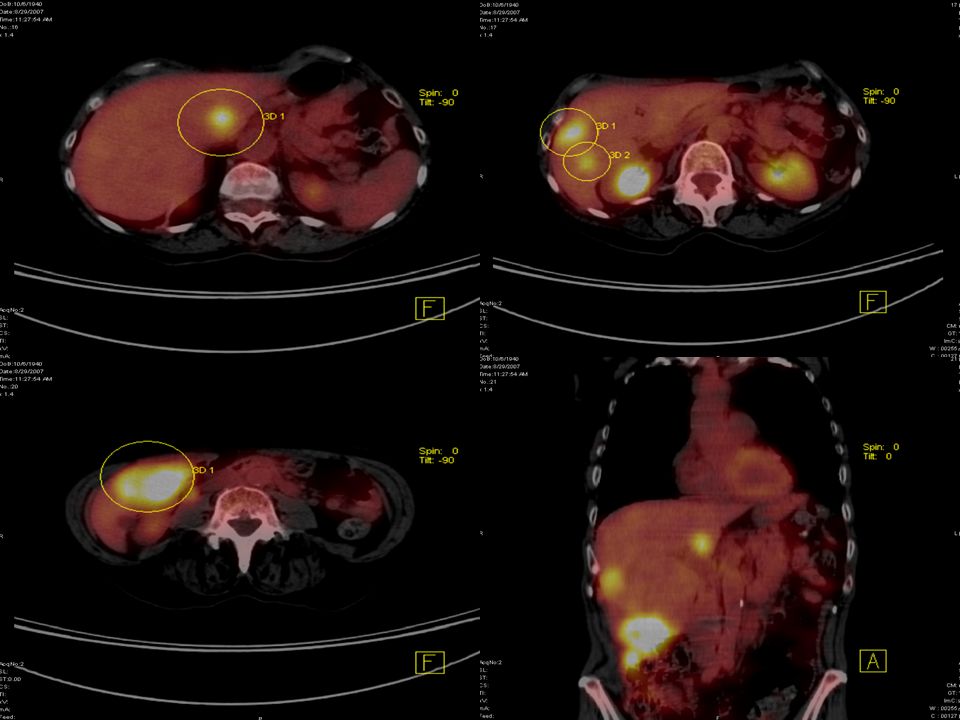
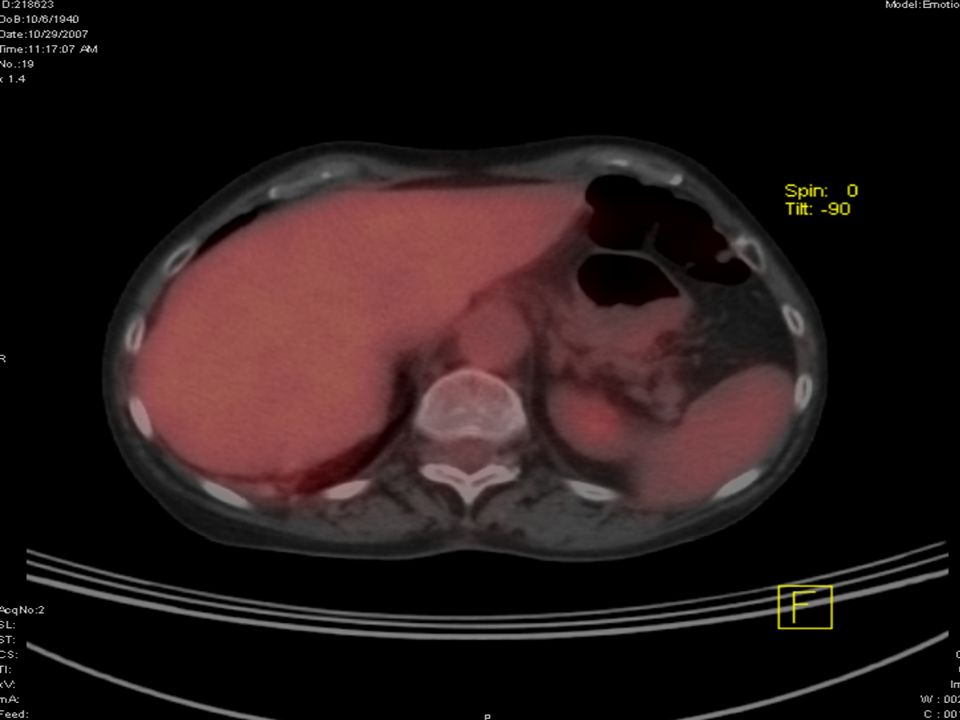
Case study: second-line treatment with erlotinib
September 2007: 15-pound weight loss, ECOG PS of 2 disease progression confirmed in bone and liver Patient commenced erlotinib 150mg/day immediate symptomatic improvement grade 1 skin rash that resolved with administration of topical moisturiser; no diarrhoea February 2008: patient continues to receive erlotinib no further side effects; sustained partial response ECOG PS = Eastern Cooperative Oncology Group performance status

31
Predicting clinical benefit with erlotinib

32
Biomarkers A biomarker is a characteristic that is objectively measured and evaluated as an indicator of normal biological processes, pathogenic processes or pharmacological responses to therapeutic intervention1 A useful biomarker can be measured reproducibly, using a reliable and widely available assay provides information about the disease that is meaningful to the physician and the patient is more informative than other measurable factors 1Biomarker Definitions Working Group, Biomarkers and Surrogate Endpoints: Preferred Definitions and Conceptual Framework. Clin Pharmacol & Ther 2001;69:89–95

33
Prognostic versus predictive markers: an important distinction
Prognostic marker Indicates the likelihood of outcome (tumour recurrence or patient survival) regardless of the specific treatment the patient receives Predictive marker Indicates the likelihood of response to a specific therapy Markers may have both prognostic and predictive value – this can complicate assessment
 regardless of the specific treatment the patient receives. Predictive marker. Indicates the likelihood of response to a specific therapy. Markers may have both prognostic and predictive value – this can complicate assessment.")
34
Challenges of biomarker testing
Obtaining tissue in sufficient quantities and of high enough quality for analyses to take place Variations in testing methods used at different sites – results cannot be directly compared Validation of biomarkers and testing methods is a complex and lengthy process Assays need to be quick, reliable, inexpensive and easy to establish in laboratories Need to have consensus and cooperation between industry and academia Future biomarkers, e.g. proteomics and gene chips, may require new technology and methods

35
BR.21: EGFR biomarker status does not predict for survival benefit with erlotinib
HR CI p* p† EGFR expression (IHC) IHC+ IHC– 0.49– –1.36 Gene copy number (FISH) Low High 0.49– –0.78 EGFR mutation status Wild-type‡ Mutant§ 0.52– –1.19 0.25 0.12 0.47 *p value for subgroup compared with placebo; †p value for interaction ‡Includes indeterminate variants; §Exon 19 deletions and L858R Tsao M-S, et al. N Engl J Med 2005;353:133–44 Tsao M-S, et al. N Engl J Med 2006;354:527–8 Shepherd FA, et al. J Clin Oncol 2007;25(Suppl. 18I):402s (Abstract 7571) FISH = fluorescence in-situ hybridisation
 IHC+ IHC– – – Gene copy number (FISH) Low High – – EGFR mutation status Wild-type‡ Mutant§ – – *p value for subgroup compared with placebo; †p value for interaction ‡Includes indeterminate variants; §Exon 19 deletions and L858R. Tsao M-S, et al. N Engl J Med 2005;353:133–44. Tsao M-S, et al. N Engl J Med 2006;354:527–8. Shepherd FA, et al. J Clin Oncol 2007;25(Suppl. 18I):402s (Abstract 7571) FISH = fluorescence in-situ hybridisation.")
36
Survival according to EGFR IHC* and EGFR FISH status in TRUST study
1.00 0.75 0.50 0.25 1.00 0.75 0.50 0.25 EGFR IHC+ (n=229) EGFR IHC– (n=55) EGFR FISH+ (n=49) EGFR FISH– (n=156) Survival distribution function Survival distribution function HR=0.766 p=0.1056† HR=0.662 p=0.0341† OS (days) OS (days) TRUST is a single-arm study and cannot therefore distinguish between prognostic and predictive value *Based on staining in 10% tumour cells †Log-rank test Schneider CP, et al. J Clin Oncol 2007;25(Suppl. 18 Pt I):S427 (Abstract 7674)
 EGFR IHC– (n=55) EGFR FISH+ (n=49) EGFR FISH– (n=156) Survival distribution function. Survival distribution function. HR=0.766 p=0.1056† HR=0.662 p=0.0341† OS (days) OS (days) TRUST is a single-arm study and cannot therefore distinguish between prognostic and predictive value. *Based on staining in 10% tumour cells †Log-rank test. Schneider CP, et al. J Clin Oncol 2007;25(Suppl. 18 Pt I):S427 (Abstract 7674)")
37
EGFR mutations and clinical outcomes with erlotinib
Presence of an EGFR mutation may increase tumour responsiveness to erlotinib requires confirmation in larger, prospective analysis BR.21 failed to show a significant effect of mutation status on survival patients with wild-type and mutated EGFR both derive survival benefit from erlotinib OS benefit seen in BR.21 cannot be fully explained by presence of patients with mutations presence of EGFR mutations may be prognostic Small patient numbers, difficulties in obtaining samples and retrospective nature limit the analyses

38
MERIT (MarkER Identification Trial): design and objectives
Mandatory samples Tumour biopsy Tumour block (if available) RNA blood sample Primary endpoint To identify differentially expressed genes that predict clinical benefit (CR, PR, SD 12 weeks) with erlotinib Patients stage IIIB/IV NSCLC (failed 1 first-line treatment*) Open-label erlotinib 150mg/day PD Second RNA blood sample Follow-up every 12 weeks Screening Day –28 Day 1 Week 6 Secondary endpoints Correlation of EGFR mutations with clinical benefit Exploratory assessment of EGFR and downstream targets Clinical assessment at screening, then every 6 weeks until PD *Or refused/were unsuitable for chemotherapy RNA = ribonucleic acid
 RNA blood sample. Primary endpoint. To identify differentially expressed genes that predict clinical benefit (CR, PR, SD 12 weeks) with erlotinib. Patients. stage IIIB/IV NSCLC (failed 1 first-line treatment*) Open-label. erlotinib. 150mg/day. PD. Second RNA blood sample. Follow-up. every 12 weeks. Screening. Day –28. Day 1. Week 6. Secondary endpoints. Correlation of EGFR mutations with clinical benefit. Exploratory assessment of EGFR and downstream targets. Clinical assessment at screening, then every 6 weeks until PD. *Or refused/were unsuitable for chemotherapy RNA = ribonucleic acid.")
39
MERIT: summary of results
MERIT is the largest prospective genomic profiling study ever conducted in advanced NSCLC The study found no binary markers for clinical benefit at the RNA expression level in baseline tumour biopsy samples In exploratory analyses, three candidate markers for response were identified on chromosome 7 EGFR, PSPH, RAPGEF5 The findings from MERIT support the use of erlotinib in patients with advanced NSCLC who have failed 1 chemotherapy regimen further validation of these findings is ongoing Reck M, et al. Eur J Cancer Suppl 2007;5:360 (Abstract 6512)
")
40
SATURN (Sequential Tarceva® in unresectable NSCLC)
Chemotherapy naïve stage IIIB/IV NSCLC Planned n=1,700 Stratify by EGFR protein expression (IHC) ‘10% cut-off’ Tumour samples (mandatory) PD Placebo Erlotinib 150mg/day Four cycles of first-line standard platinum-based doublet Non-PD (n=850) 1:1 rand TITAN (n=650) or off study PD
 ‘10% cut-off’ Tumour samples. (mandatory) PD. Placebo. Erlotinib. 150mg/day. Four cycles of first-line standard platinum-based doublet. Non-PD. (n=850) 1:1 rand. TITAN (n=650) or off study. PD.")
41
What answers will SATURN provide?
EGFR IHC+ Erlotinib 150mg/day Co-primary endpoint = 33% increase in PFS in patients with EGFR IHC+ tumours EGFR IHC– Primary endpoint = 25% increase in PFS (all patients) EGFR IHC– Placebo EGFR IHC+
 EGFR IHC– Placebo. EGFR IHC+")
42
What answers will SATURN provide?
Many other putative biomarkers will be prospectively evaluated EGFR FISH EGFR/KRAS mutations pMAPK IHC pAKT IHC HER2 IHC EGFR intron 1 polymorphisms Erlotinib 150mg/day Placebo Largest prospective biomarker study ever performed for a targeted agent results expected in late 2008

43
Other erlotinib trials performing biomarker analyses
RADIANT Adjuvant trial in selected patients (IHC and/or FISH+) with mandatory sample collection US phase II first line Selecting patients based on IHC and/or FISH+ status and also looking at EGFR and KRAS mutations, EMT, pMAPK TIE Phase II trial of first-line erlotinib in elderly; examining EGFR IHC, EGFR FISH, EGFR and KRAS mutations FAST-ACT Sequential erlotinib plus chemotherapy in first-line; analysing IHC: EGFR and related markers (e.g. pAKT, pMAPK), EGFR FISH, EGFR and KRAS mutations TRUST Global open-label study providing patients with access to erlotinib; IHC (EGFR, pAKT and pMAPK), EGFR FISH and mutation analyses (EGFR and KRAS) have been carried out for the German subpopulation; global data to be presented at ASCO 2008
 with mandatory sample collection. US phase II first line. Selecting patients based on IHC and/or FISH+ status and also looking at EGFR and KRAS mutations, EMT, pMAPK. TIE. Phase II trial of first-line erlotinib in elderly; examining EGFR IHC, EGFR FISH, EGFR and KRAS mutations. FAST-ACT. Sequential erlotinib plus chemotherapy in first-line; analysing IHC: EGFR and related markers (e.g. pAKT, pMAPK), EGFR FISH, EGFR and KRAS mutations. TRUST. Global open-label study providing patients with access to erlotinib; IHC (EGFR, pAKT and pMAPK), EGFR FISH and mutation analyses (EGFR and KRAS) have been carried out for the German subpopulation; global data to be presented at ASCO")
44
Adding other agents to erlotinib

45
Erlotinib as a combination partner in first- and second-line NSCLC
Favourable tolerability profile of erlotinib makes it an ideal agent for combination regimens in NSCLC Erlotinib/bevacizumab combination has shown promising results in clinical trials and further investigations are ongoing Erlotinib is also being investigated in sequential regimens with chemotherapy

46
Phase II study of bevacizumab with chemotherapy or erlotinib in advanced NSCLC
Median PFS (months) 6-month PFS rate (%) 1-year OS rate (%) 4.4 33.6 57.1 4.8 30.5 53.6 3.0 21.5 34.8 Erlotinib + bevacizumab (n=39) PD Erlotinib Previously treated advanced non-squamous NSCLC (n=120) Chemotherapy + bevacizumab (n=40) Chemotherapy (n=41) Randomised, multicentre study Primary endpoint: safety and preliminary efficacy (PFS) Secondary endpoints: ORR (plus duration); duration of survival OSI-2950g Bevacizumab 15mg/kg every 3 weeks; erlotinib 150mg/day orally; docetaxel 75mg/m2 and pemetrexed 500mg/m2 every 3 weeks Promising results seen with this novel approach ORR = overall response rate Herbst R, et al. J Clin Oncol 2007;25:4743–50
 6-month PFS rate (%) 1-year OS rate (%) Erlotinib + bevacizumab (n=39) PD. Erlotinib. Previously treated advanced non-squamous NSCLC (n=120) Chemotherapy + bevacizumab (n=40) Chemotherapy (n=41) Randomised, multicentre study. Primary endpoint: safety and preliminary efficacy (PFS) Secondary endpoints: ORR (plus duration); duration of survival. OSI-2950g. Bevacizumab 15mg/kg every 3 weeks; erlotinib 150mg/day orally; docetaxel 75mg/m2 and pemetrexed 500mg/m2 every 3 weeks. Promising results seen with this novel approach. ORR = overall response rate. Herbst R, et al. J Clin Oncol 2007;25:4743–50.")
47
ATLAS: bevacizumab plus erlotinib as sequential therapy following bevacizumab plus CT in first line
Bevacizumab + erlotinib PD Off study Chemotherapy naïve stage IIIb/IV non-squamous NSCLC Bevacizumab + chemotherapy* Non-PD 1:1 (n≈800) Bevacizumab+ placebo Erlotinib PD or significant toxicity PD Primary endpoint = PFS (time from randomisation until disease progression or death) Status: ongoing planned n=1,150 Off study AVG3671g (phase IIIb) Bevacizumab 15mg/kg every 3 weeks; erlotinib 150mg/day *Either carboplatin/paclitaxel, carboplatin/gemcitabine or carboplatin/docetaxel CT = chemotherapy
 Bevacizumab+ placebo. Erlotinib. PD or significant toxicity. PD. Primary endpoint = PFS (time from randomisation until disease progression or death) Status: ongoing. planned n=1,150. Off study. AVG3671g (phase IIIb) Bevacizumab 15mg/kg every 3 weeks; erlotinib 150mg/day *Either carboplatin/paclitaxel, carboplatin/gemcitabine or carboplatin/docetaxel CT = chemotherapy.")
48
BETA LUNG: erlotinib ± bevacizumab in the second-line setting
Erlotinib 150mg/day orally + bevacizumab 15mg/kg every 3 weeks PD* Previously treated advanced non-squamous NSCLC Erlotinib 150mg/day orally + placebo PD Double‑blind, randomised study Primary endpoint = OS (increase by 33%; from 8.0 to months) Secondary endpoints = PFS, RR and duration, safety and PK Status: ongoing; planned n=650 OSI-3364g (phase III) *No cross over permitted
 Secondary endpoints = PFS, RR and duration, safety and PK. Status: ongoing; planned n=650. OSI-3364g (phase III) *No cross over permitted.")
49
The future treatment algorithm for NSCLC?
Early (stage I/II/selected IIIA) NSCLC Advanced (stage IIIB with PE/IV) Suitable for standard chemotherapy? PS Age Controlled/uncontrolled brain metastases Concomitant medical condition Initiate biomarker testing at diagnosis stage? Surgery ± chemotherapy First line Yes No Radiotherapy (if unfit for surgery) Add erlotinib first line in suitable patients? Fit elderly/ PS 2? Frail elderly/ PS 3 PS 4 Locally advanced (stage IIIA/IIIB no PE) Platinum-based doublet chemotherapy ± bevacizumab Best supportive care Single agent Relapse Chemotherapy (platinum doublet) + concomitant radiotherapy or sequential Add bevacizumab to second- and third-line regimens? Chemotherapy – docetaxel – pemetrexed – vinorelbine – gemcitabine EGFR-targeted therapy – erlotinib – gefitinib Second/third line
 NSCLC. Advanced (stage IIIB with PE/IV) Suitable for standard chemotherapy PS. Age. Controlled/uncontrolled brain metastases. Concomitant medical condition. Initiate biomarker testing at diagnosis stage Surgery ± chemotherapy. First line. Yes. No. Radiotherapy (if unfit for surgery) Add erlotinib first line in suitable patients Fit elderly/ PS 2 Frail elderly/ PS 3. PS 4. Locally advanced. (stage IIIA/IIIB no PE) Platinum-based doublet chemotherapy ± bevacizumab. Best supportive care. Single agent. Relapse. Chemotherapy. (platinum doublet) + concomitant. radiotherapy. or sequential. Add bevacizumab to second- and third-line regimens Chemotherapy – docetaxel. – pemetrexed. – vinorelbine. – gemcitabine. EGFR-targeted therapy. – erlotinib. – gefitinib. Second/third line.")
50
Erlotinib in second-line NSCLC: conclusions
Erlotinib is a well-established and effective treatment option for second-line NSCLC favourable safety profile provides survival benefit in all subgroups Extensive clinical trial programme underway to establish whether biomarkers can predict clinical benefit with erlotinib includes SATURN study (data due in 2008/09) Addition of VEGF inhibitor bevacizumab also being investigated as possibility for optimisation of therapy
 Addition of VEGF inhibitor bevacizumab also being investigated as possibility for optimisation of therapy.")
Similar presentations

 vs FOLFIRI plus bev>")
 CISPLATIN 40 mg/m2 Days 1 2 22 36 50 64 92 E V A L U A.>")

 Baselga.>")




 Alone or in Combination with Carboplatin/Paclitaxel (CP) in Never or Light Former Smokers with Advanced Lung.>")
 in combination with chemotherapy: pivotal metastatic breast cancer survival data 1.>")
 Treated with Anti Vascular Endothelial Growth Factor (VEGF)>")



: investigational agents TTP = median time to disease progression OS = median overall survival.>")
 study.>")
>")
 upregulation Dose- and time-dependent upregulation of TP in human colon cancer xenografts 20 15 10 5 0 20 15 10 5 0 PaclitaxelDocetaxel.>")

