Download presentation
Presentation is loading. Please wait.

1
Dr. Aya M. Serry Non Steroidal Antiinflammatory Drugs (NSAIDs) 2014
 2014")
2
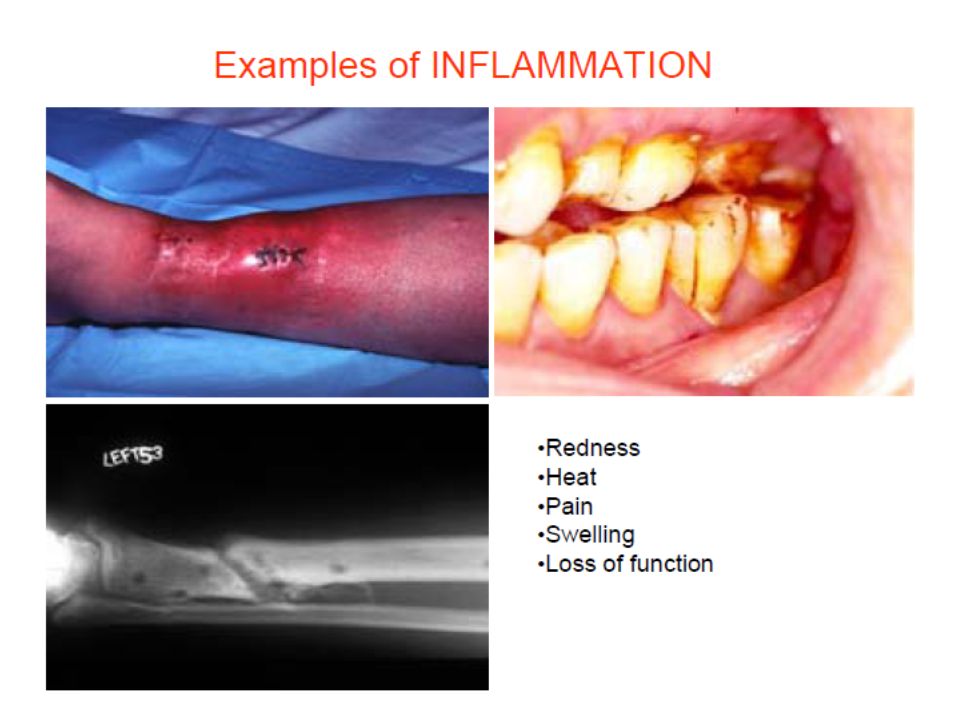
Inflammation is a defense reaction caused by tissue damage or injury Can be elicited by numerous stimuli including: infectious agents antigen-antibody interaction ischemia thermal and physical injury

3
Inflammation is Characterized by: 1.Redness: vasodilation of capillaries to increase blood flow 2.Heat: vasodilation 3.Pain: Hyperalgesia, sensitization of nociceptors 4.Swelling: Increased vascular permeability (microvascular structural changes and escape of plasma proteins from the bloodstream)
")
5
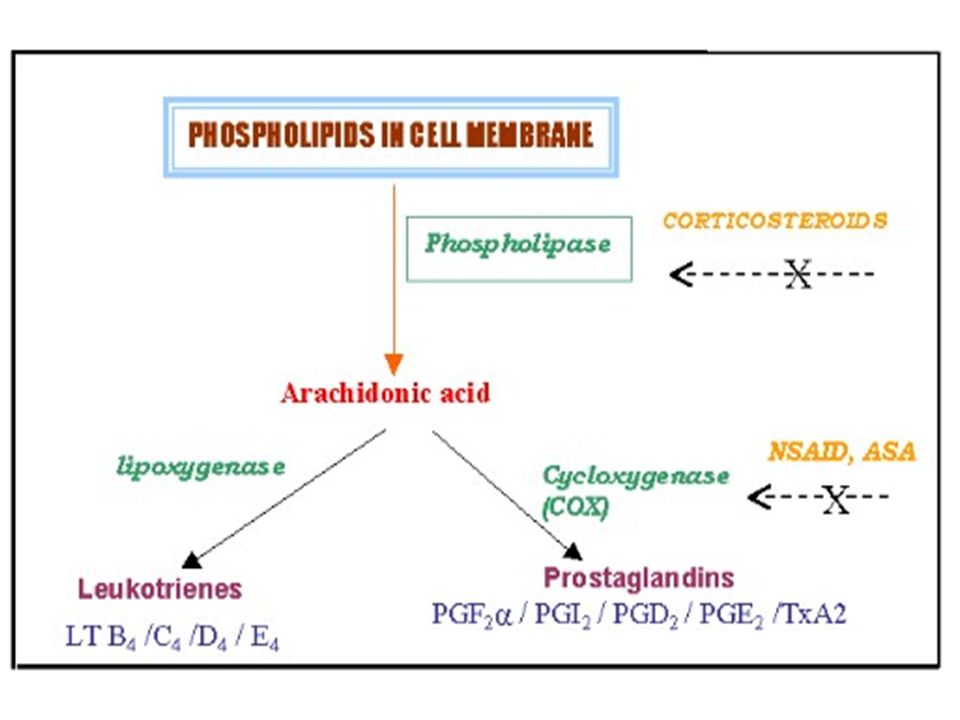
Mediators of Inflammation 1. Vasoactive amines (Histamine, Serotonin) 2. Platelet activating factor (PAF) 3. Complement system 4. Kinin system 5. Cytokines 6. Nitric oxide 7. Adhesion Molecules mediated by cyclooxygenases (COX) 8. Arachidonic acid metabolites: mediated by cyclooxygenases (COX) Prostaglandins (PGs) Thromboxane A2 (TXA2) HETE (hydroxy-eicosatetraenoic acid) Leukotrienes (LTs)
 3. Complement system 4. Kinin system 5. Cytokines 6. Nitric oxide 7. Adhesion Molecules mediated by cyclooxygenases (COX) 8. Arachidonic acid metabolites: mediated by cyclooxygenases (COX) Prostaglandins (PGs) Thromboxane A2 (TXA2) HETE (hydroxy-eicosatetraenoic acid) Leukotrienes (LTs).")
7
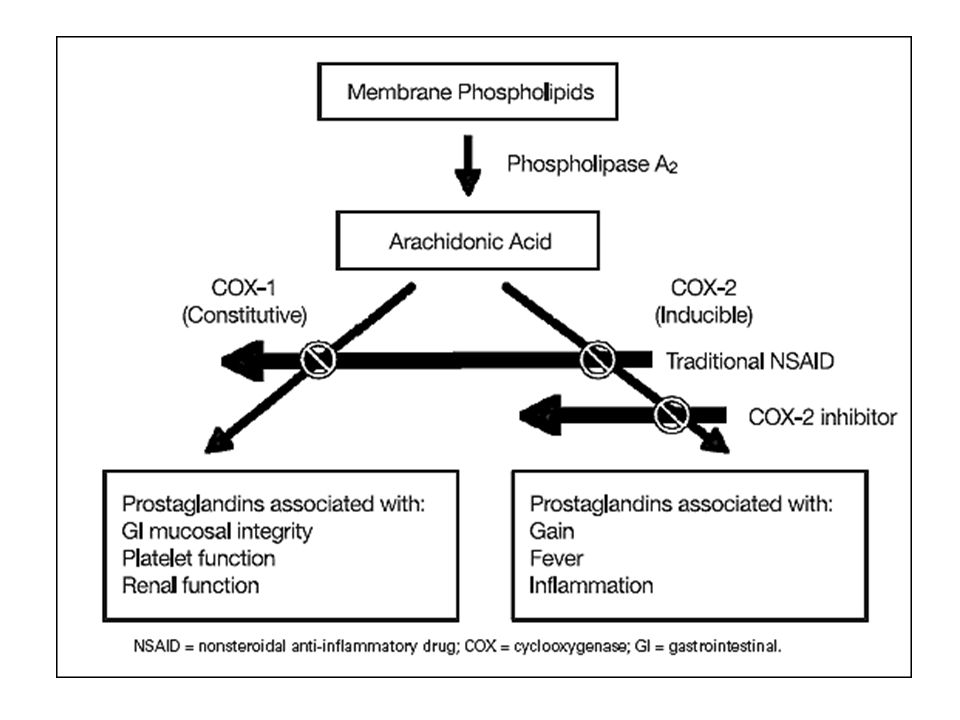
Two main forms of Cyclooxygenases (COX) Cyclooxygenase-1 (COX-1)Cyclooxygenase-1 (COX-1) Produces prostaglandins that mediate homeostatic functions Constitutively expressed Plays an important role in Gastric mucosa Kidney Platelets Vascular endothelium Cyclooxygenase-2 (COX-2)Cyclooxygenase-2 (COX-2) Produces prostaglandins that mediate inflammation, pain, and fever. Induced mainly in sites of inflammation by cytokines

8
Inflammatory responses occur in three distinct phases: transient phase 1.An acute transient phase, characterized by: –local vasodilation –increased capillary permeability subacute phase 2.A delayed, subacute phase, most prominently characterized by: –infiltration of leukocytes and phagocytic cells proliferative phase 3.A chronic proliferative phase, in which: –tissue degeneration and fibrosis occur

10
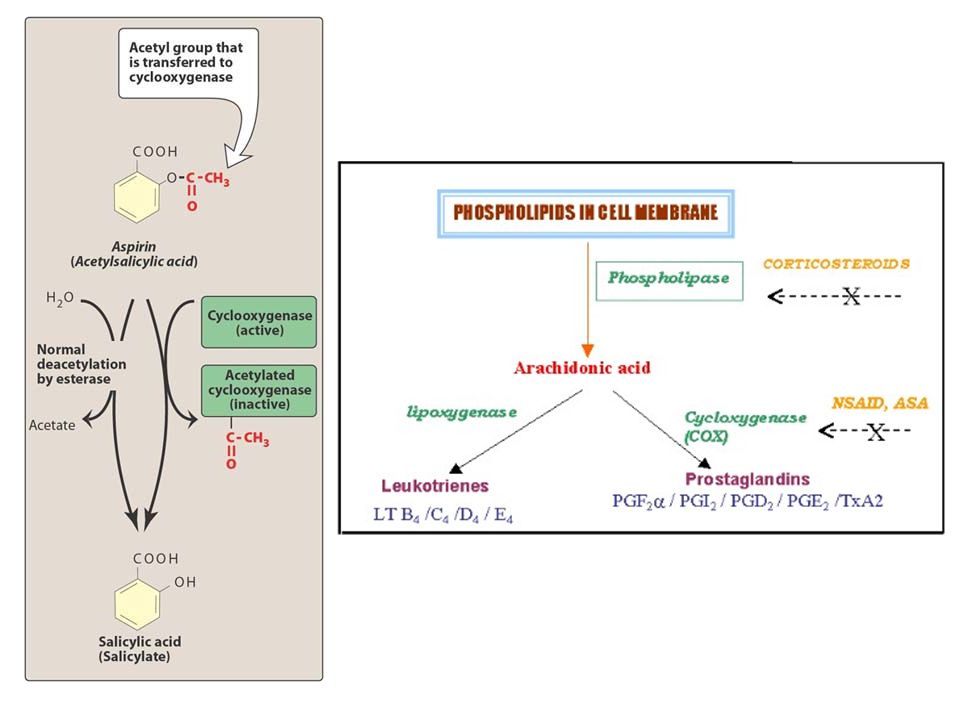
1.Anti-inflammatory effect –due to the inhibition of COX 1, or COX 2, which converts arachidonic acid to prostaglandins, and to TXA 2 and prostacyclins. –NSAIDs inactivates COX-1 and COX-2 by acetylation of a specific serine residue

11
2. Analgesic effect NSAIDs are mainly effective against pain associated with inflammation or tissue damage because they decrease production of the prostaglandins that sensitise nociceptors to inflammatory mediators such as Bradykinin Their ability to relief headache may be related to inhibition of the vasodilating effect caused by prostaglandins in the cerebral blood vessels

12
3.Antipyretic effect Normal body temperature is regulated by a centre in the hypothalamus which ensures a balance between heat loss and heat production Fever occurs when there is a disturbance of this hypothalamus “thermostat” that leads to the set point of body temprature being raised NSAIDs decrease fever by resetting this thermostat by inhibition of production of prostaglandins in the hypothalamus

13
1.Inflammation –NSAIDs are first-line drugs used to arrest inflammation and the accompanying pain of rheumatic and nonrheumatic diseases –NSAIDs do not significantly reverse the progress of rheumatic disease –they slow the destruction of cartilages and bones, allowing patients to increase mobility and use of their joints.

14
–Treatment of chronic inflammation requires use of these agents at doses well above those used for analgesia and antipyresis –the incidence of adverse drug effects is increased.

15
–Drug selection is generally dictated by the patient's ability to tolerate the adverse effects, and the cost of the drugs. –Antiinflammatory effects may develop only after several weeks of treatment.

16
2. Analgesia NSAIDs alleviate mild-to-moderate pain by: –decreasing PGE- and PGF-mediated increases in pain receptor sensitivity. They are more effective against pain associated with integument structures (pain of muscular and vascular origin, arthritis, and bursitis) than with pain associated with the viscera.
 than with pain associated with the viscera..")
17
3.Antipyresis NSAIDs reduce elevated body temperature with little effect on normal body temperature.

18
Aspirin (acetylsalicylic acid)Aspirin (acetylsalicylic acid) Nonacetylated salicylates:Nonacetylated salicylates: –sodium salicylate –magnesium salicylate –choline salicylate –sodium thiosalicylate –sulfasalazine –mesalamine –salsalate
Aspirin (acetylsalicylic acid) Nonacetylated salicylates:Nonacetylated salicylates: –sodium salicylate –magnesium salicylate –choline salicylate –sodium thiosalicylate –sulfasalazine –mesalamine –salsalate")
19
Pharmacologic properties: –Salicylates are weak organic acids; –aspirin has a pKa of 3.5. –These agents are rapidly absorbed from the intestine as well as from the stomach, where the low pH favors absorption.

20
–Salicylates are hydrolyzed rapidly by plasma and tissue esterases to acetic acid and the active metabolite salicylic acid. esterases

22
–Unmetabolized salicylates are excreted by the kidney. –If the urine pH is raised above 8, clearance is increased approximately fourfold as a result of decreased reabsorption of the ionized salicylate from the tubules.

23
Salicylates are used to treat: –rheumatoid arthritis –juvenile arthritis –osteoarthritis –other inflammatory disorders 5-Amino salicylates (mesalamine, sulfasalazine) –can be used to treat Crohn's disease.
 –can be used to treat Crohn s disease.")
24
Salicylic acid is used topically to treat: –plantar warts –fungal infections –corns

25
Aspirin –has significantly greater antithrombotic activity than other NSAIDs

26
1.Gastrointestinal effects –most common adverse effects of high-dose aspirin use (70% of patients): nausea vomiting diarrhea or constipation dyspepsia (impaired digestion) epigastric pain bleeding, and ulceration (primarily gastric).
: nausea vomiting diarrhea or constipation dyspepsia (impaired digestion) epigastric pain bleeding, and ulceration (primarily gastric).")
27
These gastrointestinal effects are thought to be due to: 1.a direct chemical effect on gastric cells or 2.a decrease in the production and cytoprotective activity of prostaglandins, which leads to gastric tissue susceptibility to damage by hydrochloric acid.

28
–The gastrointestinal effects may contraindicate aspirin use in patients with an active ulcer. –Aspirin may be taken with prostaglandins to reduce gastric damage. –Decrease gastric irritation by: Substitution of enteric-coated or timed-release preparations, or the use of nonacetylated salicylates, may decrease gastric irritation.

29
The use of aspirin and other salicylates to control fever during viral infections (influenza and chickenpox) in children and adolescents is associated with an increased incidence of Reye's syndrome It’s an illness characterized by vomiting, hepatic disturbances, and encephalopathy that has a 35% mortality rate. Acetaminophen is recommended as a substitute for children with fever of unknown etiology.

30
In adults, salicylism (tinnitus, hearing loss, vertigo) occurs as initial sign of toxicity after aspirin or salicylate overdose or poisoning. In children, the common signs of toxicity include hyperventilation and acidosis, with accompanying lethargy and hyperventilation.

32
–Paracetamol has an analgesic and antipyretic activity but minimal anti-inflammatory effect –It’s possible that its antipyretic action is due to a selective effect on a specific COX enzyme in the CNS –it causes minimal gastric irritation –has little effect on platelet adhesion and aggregation –Acetaminophen has no significant antiinflammatory activity.

33
–Acetaminophen is administered orally and is rapidly absorbed. –Acetaminophen is a substitute for aspirin to treat mild- to-moderate pain for selected patients who are: intolerant to aspirin have a history of peptic ulcer are using anticoagulants are at risk for Reye's syndrome.

34
accumulation of a minor metabolite, N-acetyl-p-benzoquinone, which is responsible for hepatotoxicity.

36
–Celecoxib [Celebrex] –Rofecoxib [Vioxx] –Valdecoxib [Bextra] –They are drugs that inhibit COX-2 more than COX-1 have been developed and approved for use. –The rationale behind development of these drugs was that: A.inhibition of COX-2 would reduce the inflammatory response and pain B.not inhibit the cytoprotective action of prostaglandins in the stomach, which is largely mediated by COX-1.
![–Celecoxib [Celebrex] –Rofecoxib [Vioxx] –Valdecoxib [Bextra] –They are drugs that inhibit COX-2 more than COX-1 have been developed and approved for use.](http://images.slideplayer.com/26/8454637/slides/slide_36.jpg "–The rationale behind development of these drugs was that: A.inhibition of COX-2 would reduce the inflammatory response and pain B.not inhibit the cytoprotective action of prostaglandins in the stomach, which is largely mediated by COX-1..")
37
–Rofecoxib and valdecoxib –Rofecoxib and valdecoxib have been removed from the market due to a doubling in the incidence of heart attack and stroke –Celecoxib –Celecoxib remains on the market and is approved for: –Osteoarthritis and rheumatoid arthritis –Pain including bone pain, dental pain, and headache

Similar presentations














. Inflammation is a defense reaction caused by tissue damage or injury Can be elicited by numerous stimuli.>")




